

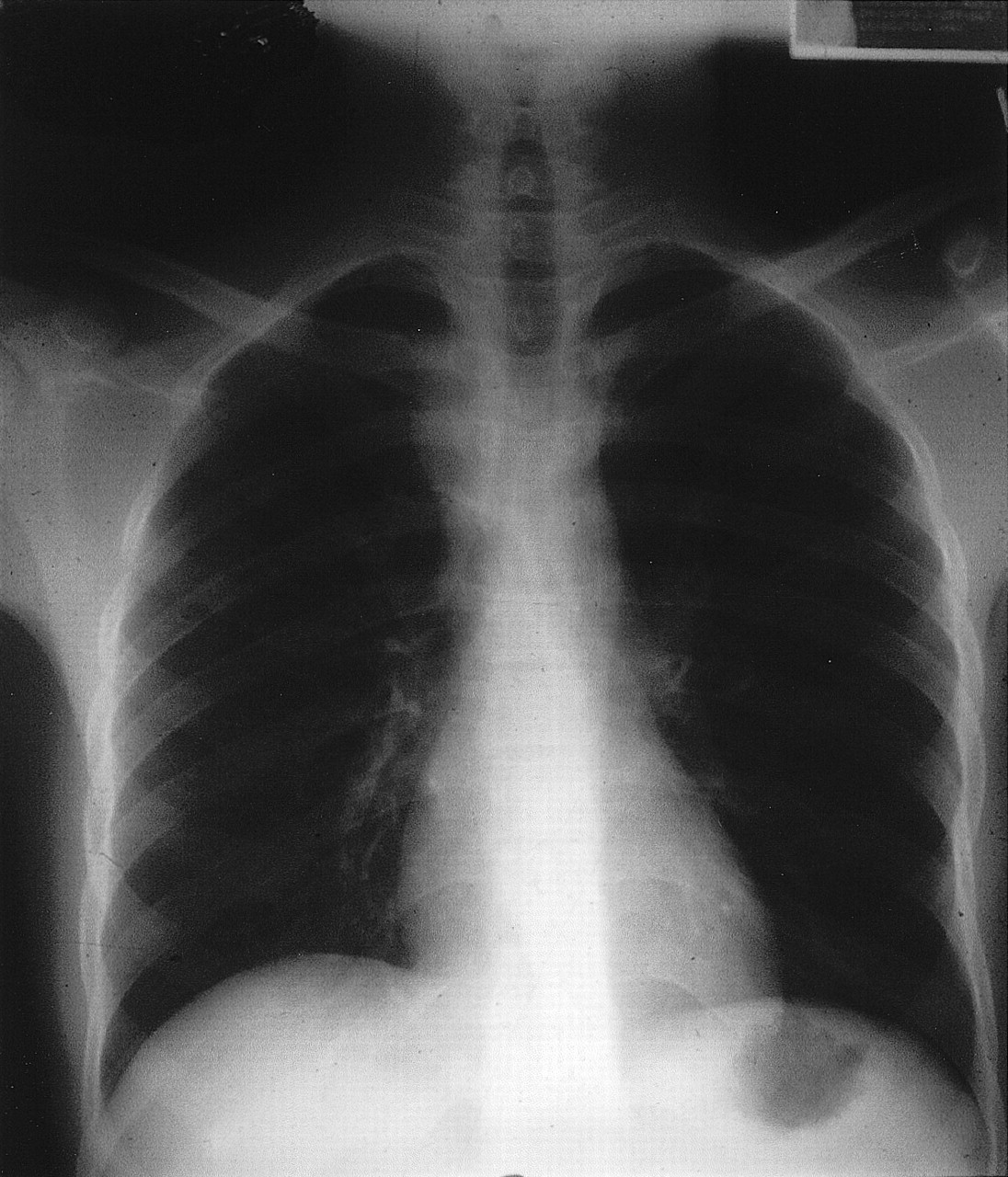
A 23-year-old man was well when he came to Canada as a refugee from northern Africa. Tuberculosis (TB) screening during the immigration process had yielded a negative Mantoux skin test result. However, 3 months later he had fever, reduced appetite and night sweats and was noted by his family physician to have a small mass in the lower right side of his neck that was moderately firm and nontender. Small lymph nodes were also palpable in his neck and axillae. A month later the neck mass had grown to 6 cm in diameter (Fig. 1), and the patient was referred to our infectious disease clinic. At this point the differential diagnosis included lymphoma, bartonellosis, trypanosomiasis and extrapulmonary TB. Several investigations, including complete blood count and liver function tests, gave normal results. With his consent the patient was tested for HIV and was found to be seropositive with a low CD4 count (25 [normally 700–1100] х 106/L). A chest radiograph showed a widened mediastinum but no parenchymal disease (Fig. 2). Thick, purulent fluid aspirated from the mass showed multiple acid-fast bacilli, and a culture was positive for Mycobacterium tuberculosis. Initial treatment was with isoniazid, rifampin, pyrazinamide and ethambutol for 2 months followed by isoniazid and rifampin, with gradual shrinking of the mass. Anti-HIV therapy with zidovudine, lamivudine and efavirenz was also given, along with trimethoprim–sulfamethoxazole for Pneumocystis carinii prophylaxis. Unfortunately 4 months after treatment was started, the patient became severely depressed and decided to return home, discontinuing all medical therapies.

{kind=link}
{kind=link}
This case highlights some of the challenges of diagnosing and managing TB and HIV coinfection. HIV infection has allowed a resurgence of TB worldwide, with HIV-positive patients being more susceptible to primary TB and to reactivated TB in those with latent disease.1 In Africa, TB is one of the most common pulmonary complications of HIV infection, with at least one-third of HIV-positive people having active TB.2 HIV-positive patients with a CD4 cell count of less than 200 х 106/L often have mediastinal adenopathy and other extrapulmonary manifestations.3 Although a 6-month course of treatment for TB lymphadenitis is effective,4 a longer course may be required in patients with HIV infection. The use of highly active antiretroviral therapy (HAART) is associated with improved cellular-mediated immune function, which leads to accelerated clearance of Mycobacteria and reduced mortality among AIDS patients with TB.5 However, problems with pill burden, drug interactions, tolerance and compliance are common. Our case also highlights the potential unreliability of tuberculin skin tests in identifying TB reactivation in HIV-positive patients. Although our patient's rapidly evolving and relatively superficial lesion was identified as extrapulmonary TB relatively quickly, significant delays in the diagnosis of both his HIV infection and TB could easily have occurred.
Chau Nguyen Department of Infectious Disease Health Sciences Centre St. John's, Nfld.
References
- 1.
- 2.
- 3.
- 4.
- 5.