

Reason for posting: Dihydroergotamine and ergotamine are ergot alkaloids commonly used to treat migraines.1 Many clinicians may be unaware of recently recognized interactions of these ergot derivatives with several commonly used antibiotic, antiviral and antifungal drugs.2
The drugs: Ergot alkaloids are derived from the grain fungus Claviceps purpurea. In the Middle Ages, contaminated grain caused plagues of ergotism characterized by gangrene and an intense peripheral burning pain (known as “St. Anthony's fire”), spontaneous abortion and occasional episodes of mania and hallucinations.3 Initially used therapeutically by European midwives to hasten labour (with many untoward effects), ergot derivatives eventually found a life-saving role in the treatment of post-partum hemorrhage.3 Ergotamine was first used in the treatment of acute migraine in 1926.4
Unlike triptan medications, which have a more selective affinity for serotonin 5-HT1 receptors, ergotamine and dihydroergotamine are nonselective 5-HT1 agonists.1 They also have affinities for dopamine and noradrenaline receptors.4 Common adverse effects of ergotamine and dihydroergotamine are nausea, vomiting, abdominal pain, diarrhea, peripheral paresthesias, swollen fingers, generalized weakness, and peripheral and coronary vasoconstriction.4 The drugs are contraindicated in people with peripheral vascular disorders, coronary artery disease, stroke, severe hypertension, pregnancy, hepatic or renal failure, or sepsis.4
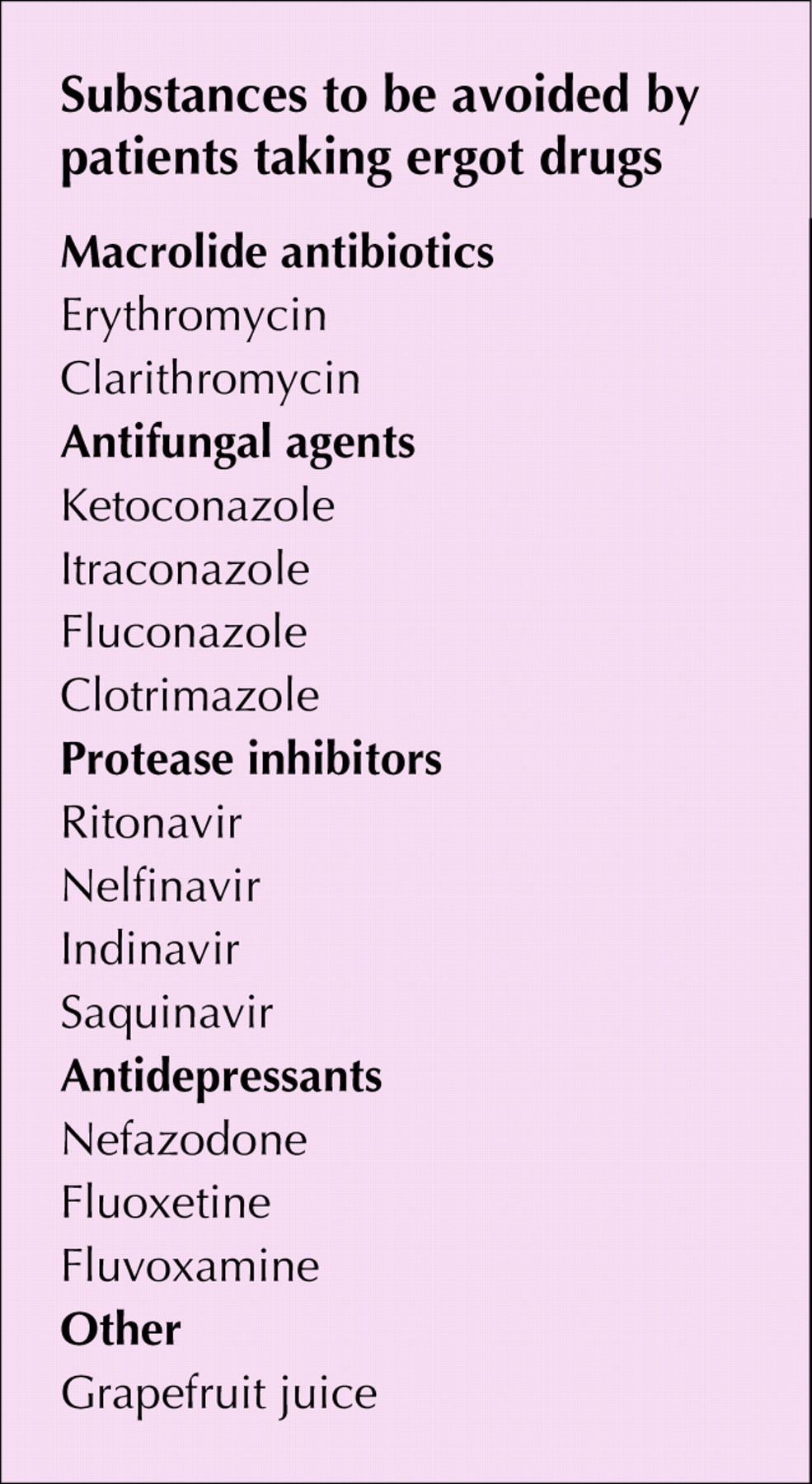
Ergotamine and dihydroergotamine are metabolized in the liver by the cytochrome P450 (CYP) 3A4 enzyme. Several medications (see box) are CYP 3A4 inhibitors and slow the metabolism of ergotamine, causing serious toxic effects, including stroke, gangrene and death.2,5,6 Other CYP 3A4 inhibitors, such as grapefruit juice,7 and drugs including heparin, cyclosporine, tacrolimus and ampicillin present at least the theoretical possibility of drug interactions.8 Ergotamine and dihydroergotamine are marketed in Canada in several preparations, including Migranal, Cafergot and Bellergal.
{kind=link}
What to do: Physicians are often unaware of all the medications their patients take, especially those prescribed by other physicians and those taken only intermittently. Thus, common CYP 3A4 inhibitors (see box) may inadvertently be prescribed to patients taking ergot derivatives, increasing their risk of serious adverse effects. Other migraine therapies could be considered. Physicians prescribing ergot-related drugs should advise their patients to watch for persistent numbness, tingling, ice-cold limbs, muscle cramps and weakness, and to seek medical attention if these occur.
Eric Wooltorton CMAJ
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.