

Case
A 50-year-old woman with type 2 diabetes mellitus identified 5 years earlier presents for an annual physical examination. She has no history of hypertension and is not known to have had a previous cardiovascular event. She visits the ophthalmologist annually. Her medications include an over-the-counter multivitamin, an oral hypoglycemic agent and a statin for known hypercholesterolemia. She is otherwise well, and the findings on physical examination are unremarkable. Her physician is aware of recent Canadian Diabetes Association guidelines advising microalbuminuria screening for diabetic patients. Should the woman be screened for microalbuminuria on this visit? What is the best way to screen for it? If the test result is positive, what does this mean in terms of the patient's risk for cardiovascular and renal disease? Is there anything that can be done medically for microalbuminuria? What follow-up is required, including management of other risk factors?
The incidence of diabetes mellitus in North America is reaching epidemic proportions and is expected to double by 2025.1 Over 5% of the population is known to have diabetes, and as many as another 2.5% are estimated to have the disease without knowing it.2 The prevalence of diabetes is increasing faster in the First Nations population than in the general population, and the onset is occurring at ever earlier ages.3 Diabetes is the most common cause of end-stage renal disease (ESRD) in Canada and is a major risk factor for cardiovascular disease and blindness.4
Microalbuminuria represents an abnormally elevated urine albumin level that cannot be detected with the use of a urinalysis dipstick. The presence of microalbuminuria predicts worsening of renal disease to overt diabetic nephropathy5 and an elevated risk of cardiovascular disease.6,7,8,9 Up to 30% of people with newly diagnosed type 2 diabetes will already have abnormally high urine albumin levels; about 75% of these people will have microalbuminuria and about 25% will have overt diabetic nephropathy.10,11,12,13,14 Patients with type 2 diabetes who were enrolled in the MICRO-HOPE study, for example, had a risk of progression from normal to diabetic nephropathy of 2% and a risk of progression from microalbuminuria to diabetic nephropathy of 20% over 5 years.15 These rates are similar for type 1 and type 2 diabetes.16,17,18,19,20,21
Early detection of microalbuminuria through screening allows interventions aimed at preventing diabetic nephropathy. In this article we review strategies for microalbuminuria screening in diabetic patients and for introducing therapies to prevent the progression of renal disease.
Diagnosis
Patients with diabetes are at risk of microalbuminuria if they have any of the following factors:
· the urine albumin excretion is in the upper range of normal (20–30 mg/d);
· the systolic blood pressure is greater than 130 mm Hg;
· the glycosylated hemoglobin level is greater than 0.09; or
· the total cholesterol level is greater than 5.24 mmol/L.
Several methods for screening for microalbuminuria are available, including timed urine collections (over 24 hours or overnight) to measure protein levels and random urine tests using laboratory tests, dipsticks or special devices (e.g., automated urine analyzers) to measure microalbumin levels or to calculate the microalbumin:creatinine ratio (MACR). Regular urinalysis dipsticks are not sensitive enough to detect early microalbuminuria.
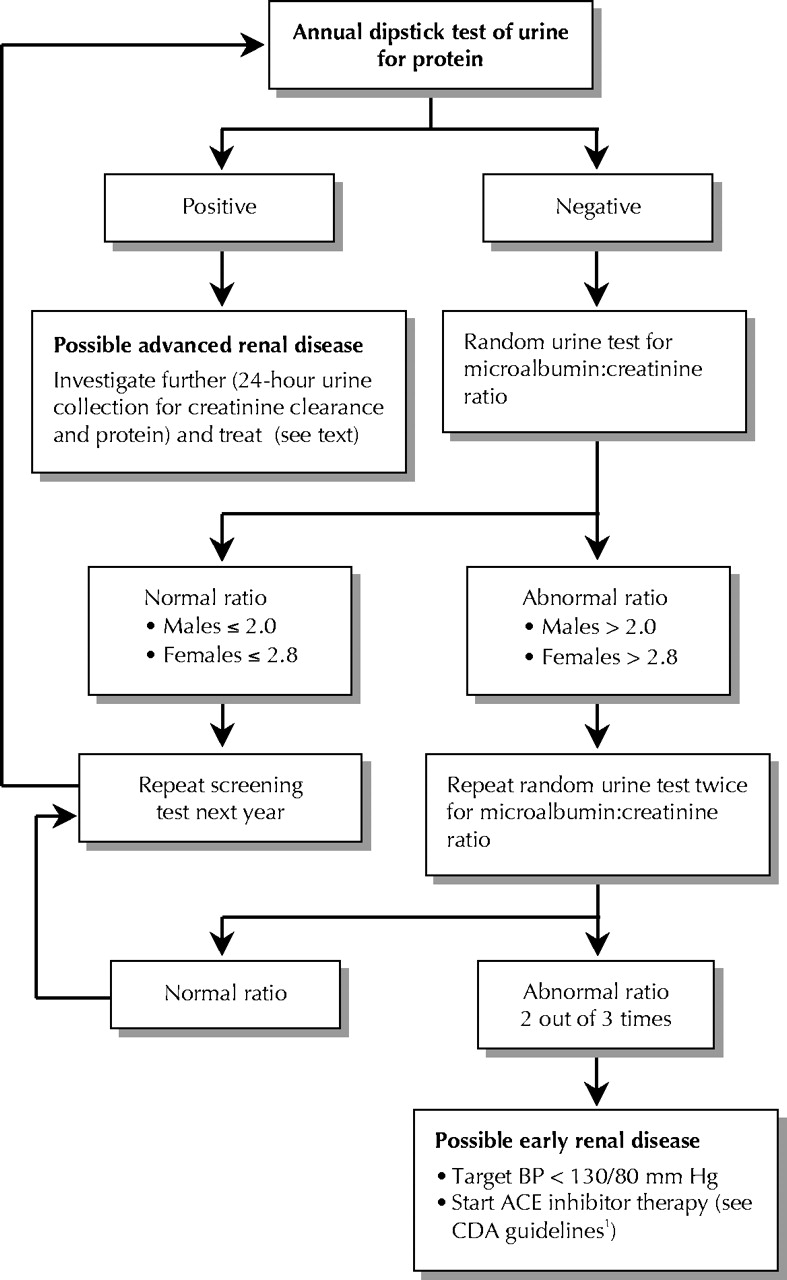
Microalbuminuria is diagnosed when the urine albumin level is 30 mg/d or greater (Table 1). This can be expressed either as a quantity of albumin excreted per time (> 20 μg/min) or as a concentration (> 20 mg/L urine). The Canadian Diabetes Association recommends the calculation of the MACR from a random urine sample (Fig. 1).1 The MACR is preferable to a simple measure of albumin excreted in urine because the latter can be distorted by the effects of urine concentration. The MACR is more convenient to perform than a 24-hour urine collection, and the results of these 2 tests have been shown to correlate highly.22 Given that there is significant variability in the daily amount of albumin excreted in urine, the Canadian Diabetes Association recommends that microalbuminuria be diagnosed only if the MACR is abnormal in 2 out of 3 tests.1
Table 1.

Fig. 1: Guidelines for screening microalbuminuria in patients with diabetes mellitus. BP = blood pressure, ACE = angiotensin-converting-enzyme, CDA = Canadian Diabetes Association.
Because urine albumin excretion is a continuum, we have indicated ranges that define normal, microalbuminuria and overt diabetic nephropathy (Table 1). Higher albumin excretion within each range is predictive of the risk of progression to the next.23 Worsening of renal disease in people with diabetes is also predicted by the severity of other traditional cardiovascular risk factors, including blood pressure, cholesterol level and blood glucose level.24
Management
Glycemic control can prevent progression to microalbuminuria. Preventing the progression of each step of renal disease in patients with diabetes — microalbuminuria, diabetic nephropathy, and ESRD or death — can be achieved with blood pressure control25 and the use of antiangiotensin therapies such as angiotensin-converting-enzyme (ACE) inhibitors and angiotensin II receptor blockers (Fig. 2, Table 215,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41).
Table 2.

Fig. 2: Prevention of progression of renal disease in people with diabetes mellitus. ARB = angiotensin II receptor blocker, ESRD = end-stage renal disease.
Primary prevention (preventing microalbuminuria) can be achieved through good glycemic26 and blood pressure control30 and through the use of an ACE inhibitor in both type 1 and type 2 diabetes27,28 (Table 2).
Secondary prevention (preventing the progression from microalbuminuria to diabetic nephropathy) can be achieved with an ACE inhibitor in both type 1 and type 2 diabetes15,32,33,34,35,36 and with an angiotensin II receptor blocker40 in type 2 diabetes (Table 2). In the study by Parving and associates40 antiangiotensin therapy with irbesartan was found to reverse microalbuminuria in up to one-third of patients. Of interest, in that study, the higher dose of irbesartan (300 mg) was significantly more protective than the lower dose (150 mg) against progression from microalbuminuria to diabetic nephropathy (59% v. 10%).
Tertiary prevention (preventing the progression from diabetic nephropathy to ESRD) independent of the blood pressure effect can be achieved with an ACE inhibitor in type 1 diabetes42 and with an angiotensin II receptor blocker in type 2 diabetes.43,44 It is unknown whether ACE inhibitors and angiotensin II receptor blockers are equally effective or whether they are more effective when combined.
Once microalbuminuria is diagnosed in a patient with diabetes, it is time to stress to the patient the need to manage multiple risk factors for cardiovascular disease. The target blood pressure should be below 130/80 mm Hg,45 the target low-density lipoprotein cholesterol level should be below 2.5 mmol/L,46 and smoking cessation should be mandatory.
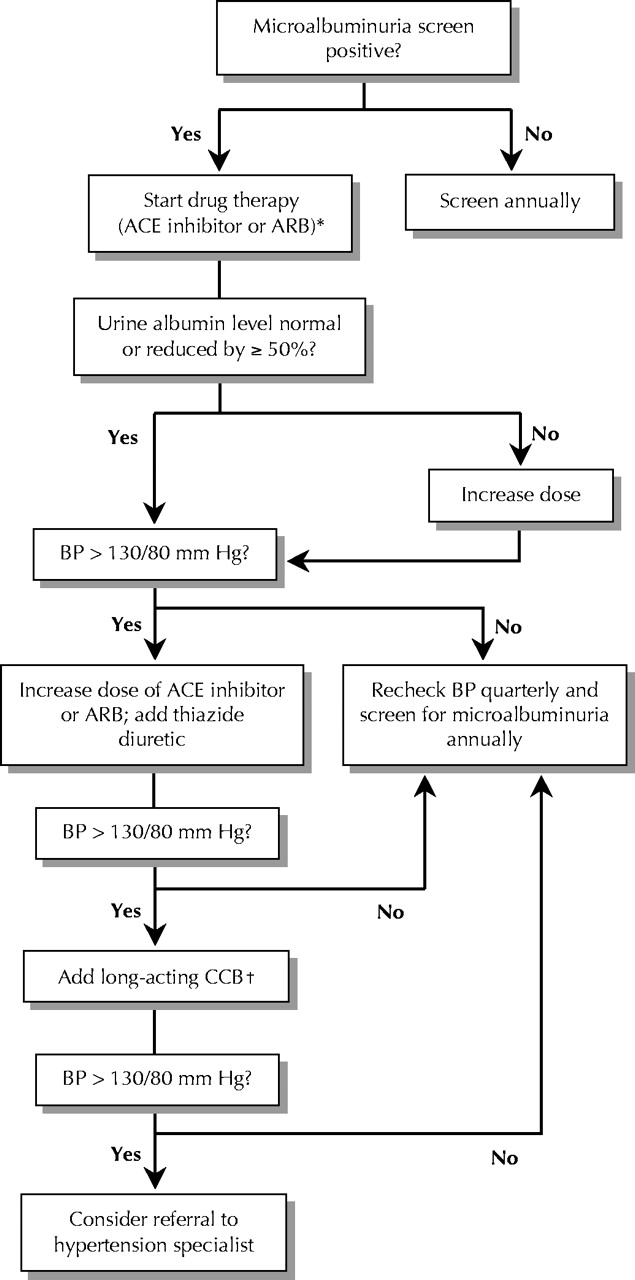
Fig. 3 outlines a potential algorithm for controlling blood pressure in people with diabetes. Combinations of antihypertensive drugs are often needed to achieve the target blood pressure.48 The algorithm represents an extrapolation from existing evidence; however, evidence concerning the most effective combination or order of medications has not yet been established in trials. Diabetic patients with microalbuminuria should have their blood pressure monitored quarterly and their renal function checked annually, or more often if they have risk factors for vascular disease. If renal function deteriorates, referral to a nephrologist is appropriate.
{kind=link}
{kind=link}
{kind=link}
Fig. 3: Possible algorithm for controlling blood pressure in diabetic patients with microalbuminuria. [This algorithm is based on the opinions and practice of the authors.] CCB = long-acting calcium-channel blocker. *On the basis of results of recent clinical trials, start with an ARB40 or ACE inhibitor.15 †Possible agents to add are a long-acting dihydropyridine CCB44,47 and a β-blocker if necessary; another possibility instead of these agents is a nondihydropyridine CCB, with no β-blocker, particularly if the patient's heart rate is greater than 80 beats/min.48
Case revisited
The patient should have a random urine test to determine the MACR. If the ratio is greater than 2.8 the test should be repeated twice. If the ratio is greater than 2.8 in 2 out of 3 tests, microalbuminuria should be diagnosed and antiangiotensin therapy started with an ACE inhibitor or angiotensin II receptor blocker. Because of the patient's increased risk of cardiovascular and renal disease, her blood pressure and hypercholesterolemia should be closely monitored and managed as necessary.
Comments
Microalbuminuria screening meets the fundamental requirements for a screening test,49 and because it is cost-effective it will help to relieve some of the burden on our health care system. In our view, the Canadian Diabetes Association practice guideline regarding microalbuminuria screening1 is an important contribution to the management of patients with diabetes. In conscientiously applying the guideline, physicians may be able to prevent progressive renal disease, and ultimately renal failure, in many patients with diabetes.
Key points
-
Diabetes mellitus is becoming increasingly common.
-
Microalbuminuria is likely to be found in one-third or more of diabetic patients.
-
Microalbuminuria is a risk factor for cardiovascular and renal disease.
-
Antiangiotensin therapy and blood pressure control can reduce urine albumin levels and give renal protection.
-
All patients with type 2 diabetes should be screened annually for microalbuminuria.
-
Determine the microalbumin:creatinine ratio from a random urine sample. Microalbuminuria is present if the ratio is abnormal (> 2.0 in men, > 2.8 in women) in 2 out of 3 tests.
Additional resources
-
American Diabetes Association: www.diabetes.org
-
Canadian Diabetes Association: www.diabetes.ca
-
Canadian Hypertension Society: www.chs.md
-
National Institutes of Health diabetes site: www.niddk.nih.gov/health/diabetes/diabetes.htm
Drugs in classes referred to in this article
-
Angiotensin II receptor blockers: candesartan, eprosartan, irbesartan, losartan, telmisartan, valsartan
-
Angiotensin-converting-enzyme (ACE) inhibitors: benazepril, captopril, cilazapril, enalapril, fosinopril, lisinopril, perindopril, quinapril, ramipril, trandolapril
-
Dihydropyridine calcium-channel blockers (CCBs): amlodipine, felodipine, nifedipine
-
Nondihydropyridine CCBs: diltiazem, verapamil
-
Thiazide diuretics: hydrochlorothiazide, indapamide
-
β-Blockers: atenolol, bisoprolol, metoprolol
Footnotes
-
This article has been peer reviewed.
Contributors: All of the authors contributed substantially to the content of the article, participated in the drafting and revising of the manuscript and approved the final version.
Competing interests: Dr. Tobe has received speaker fees from and has attended meetings sponsored by most of the major pharmaceutical companies. Dr. McFarlane has received speaker fees from Aventis Pharma, Bristol-Myers Squibb and Merck Frosst. Dr. Naimark has received speaker fees from Janssen-Ortho Biotech.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.