

Abstract
IN 1996 WE ESTABLISHED A DAY HOSPITAL DEDICATED to acute respiratory care, as an alternative to emergency department and inpatient treatment. The unit is staffed by respirologists, family physicians and specialized nurses; patients have access to all standard inpatient treatments and services. Between 1996/97 and 1998/99 the annual number of admissions to the day hospital increased from 658 to 922. By 1998/99 more than 75% of patients were referred for acute treatment, with a mean stay of 2.3 days. The most common diagnoses were asthma and chronic obstructive pulmonary disease, which accounted for 58% and 32% respectively of treatment-related admissions. Treatment most often involved intravenous corticosteroid therapy and inhaled bronchodilator therapy. Between 1996/97 and 1998/9 the proportion of patients requiring transfer to overnight care decreased from 22% to 14%; complications and unscheduled return visits were rare. We believe that a respiratory day hospital provides a useful alternative to emergency department and inpatient care.
Obstructive airways diseases (chronic obstructive pulmonary disease [COPD] and asthma) remain a leading cause of death and illness and account for a large proportion of health care costs.1,2,3 In Montreal, emergency department occupancy has peaked during recent winters. Each peak has been clearly associated with a sharp rise in hospital admissions because of respiratory disease, primarily pneumonia, bronchitis and asthma (Direction de la santé publique, Montréal-Centre: unpublished data, 1999).
In the early 1990s the Montreal Chest Institute (MCI) experienced a similar surge in admissions and emergency department visits each winter. During the fiscal year 1994/95, there were 1148 visits to the emergency department. There were 789 admissions to 41 acute care beds, with unadjusted mean lengths of stay for people with COPD (37% of admissions) and uncomplicated asthma (13% of admissions) that were significantly longer than the mean lengths of stay for the province of Quebec (13.0 v. 9.7 days for COPD and 6.9 v. 4.2 days for asthma) (Régie de l'assurance maladie du Québec, MED-ECHO: unpublished data, 1995). Despite undoubted referral bias, we judged these lengths of stay to be excessive. From chart reviews, we estimated that 25% of inpatient days could potentially be transferred to a less resource-intensive level of care. Moreover, most emergency care was delivered in 2 small “walk-in” rooms in our outpatient clinic, where space and patient supervision were inadequate. Hence, alternatives to emergency department and inpatient treatment warranted careful consideration.
Recent reports from the United Kingdom have described “hospital at home” or “supported early discharge” for exacerbations of uncomplicated COPD.4,5,6 Patient outcomes were similar to those with traditional inpatient care, and one discharge program also suggested substantial cost savings. However, our own personnel could not efficiently provide home care to fluctuating numbers of patients who were geographically dispersed, and community resources for home acute care did not exist.
The concept of a day hospital, offering acute or subacute care over a series of days, is well established in psychiatry and geriatrics.7,8 It implies ongoing assessment or intervention, or both, in contrast to relatively brief encounters in the standard outpatient setting. In various specialty practices, there are facilities dedicated to acute, labour-intensive interventions conducted on an ambulatory basis (e.g., day surgery and hemodialysis). Such units can provide high-quality care at reduced cost, although interventions are planned rather than emergent.9
A French group reported a day hospital devoted to the investigation and diagnosis of respiratory disease.10 Researchers at Cook County Hospital, Chicago, conducted a randomized controlled trial of admission to a short-stay “emergency diagnostic and treatment unit” versus direct inpatient admission for patients with asthma (mean age 36 years).11,12 Of the patients randomly assigned to the unit, 59% were discharged home. Compared with the inpatient care group, patients referred to the unit had a shorter mean hospital stay (36.7 v. 59.0 hours), higher patient satisfaction scores, higher health-related quality-of-life scores and lower costs. There was no difference between the 2 groups in rates of relapse or death during 8 weeks of follow-up. These results highlight successful acute respiratory care in an intensive ambulatory setting.
In 1996 we established a day hospital with a major focus on the acute treatment of obstructive airways disease. In this article we describe the program, its initial outcomes and its costs.
The respiratory day hospital
Our mission is to provide high-quality medical and nursing care, within a multidisciplinary framework, to patients requiring specialized treatment, investigation or teaching with respect to respiratory disease. Specific goals are (a) to avoid hospital admission where possible, (b) to permit earlier discharge from hospital by using the day hospital as a “step-down” facility, (c) to unburden the emergency treatment and observation area and (d) to foster an integrated approach to patient care, by serving as a bridge between the outpatient clinic and the inpatient wards. This approach promotes systematic patient teaching, better liaison with the treating physicians and nurses, and better coordination with community resources.
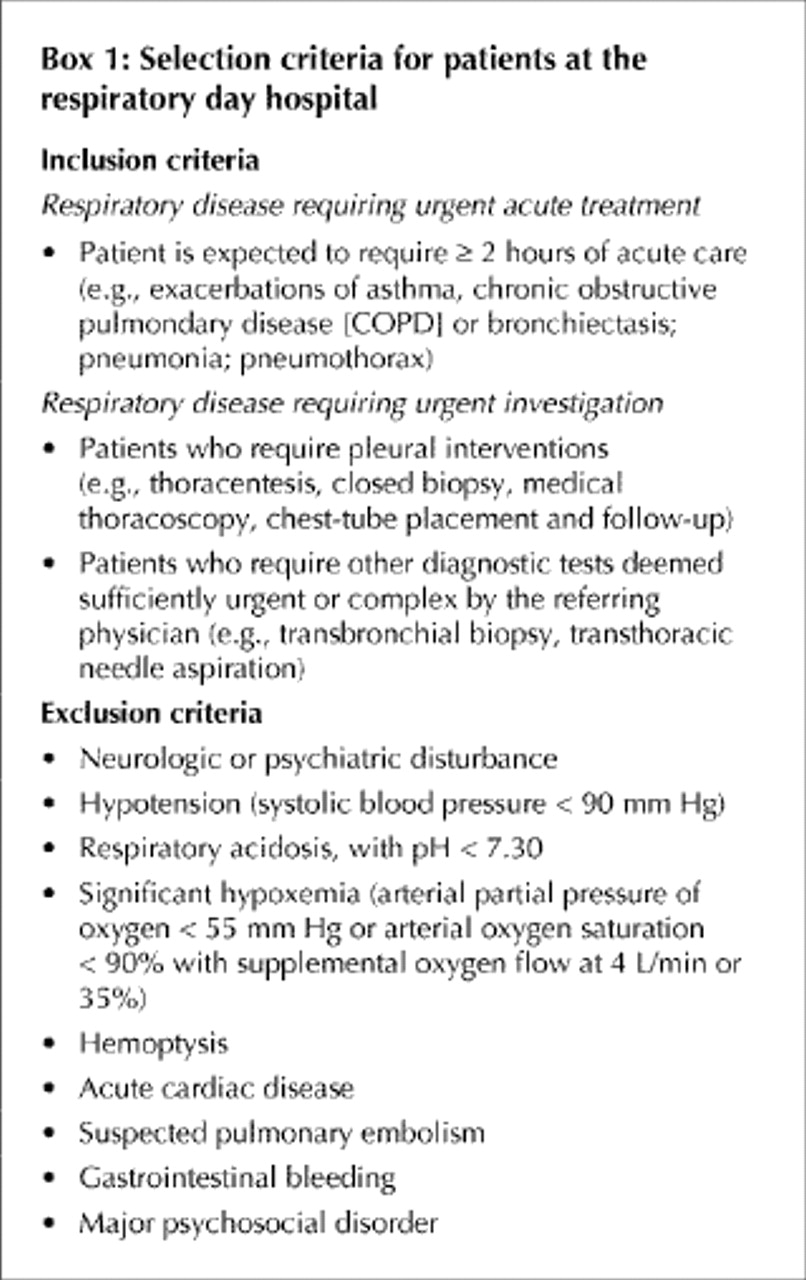
Box 1 summarizes eligibility criteria for patient referral to our day hospital. During day-hospital hours, any suitable patient seen in our outpatient clinic or emergency department who is expected to require 2 or more hours of care is transferred to the day hospital, unless the patient is judged to be so ill as to require immediate admission to an inpatient ward or the intensive care unit. Patients may also be transferred to our day hospital from inpatient wards, from other emergency departments and hospital clinics and from physicians' private offices.
{kind=link}
The respiratory day hospital is located on a former inpatient ward. It includes 3 rooms with 4 hospital beds each. Each bed has access to oxygen and suction. In addition, there are 3 reclining chairs in a lounge area and a 2-bed procedure room. The day hospital is routinely open Monday through Friday from 8 am to 8 pm, with weekend hours added as needed.
Staffing
Medical coverage is provided by a dedicated respirologist, on a 2-week rotation basis, with assistance from a family physician or a respirology resident. There are 2 full-time staff nurses; they alternate shifts, with the first shift running from 8 am to 4 pm and the second from noon to 8 pm. There is a full-time ward secretary and a head nurse shared with the adjacent intensive care unit. Patients have immediate access to all ancillary services, such as an inhalation therapist, a chest physiotherapist, a liaison nurse, asthma and COPD nurse specialists and a social worker. Bedside spirometry is routinely performed by an inhalation therapist, in the morning and in the late afternoon.
Patients are evaluated by the physician on admission, then as frequently as needed. At a minimum, they are seen twice daily: during the morning and again at the end of the afternoon, when they are assessed to determine whether they will (a) be discharged home definitively, (b) go home for the night but return to the day hospital the next morning or (c) require transfer to the inpatient ward for overnight stay in hospital. Physicians at the day hospital are responsible for all medical orders and all decisions regarding admission and discharge.
Treatments include intravenous and oral administration of medications and inhaled bronchodilator therapy. When patients are to return for subsequent intravenous therapy, they are sent home with an intravenous lock, to be kept overnight. All medications are supplied by the hospital without charge to patients, as are meals. The nurses provide individualized teaching to patients, most frequently involving a review of their technique for self-administering inhaled medications.
For needy patients without other means of transportation, taxi vouchers are provided; parking expenses are also covered for needy patients who park their own cars at the hospital.
Documentation
Each time a patient is admitted to the day hospital, an admission chart is prepared that resembles the standard inpatient ward chart. A brief summary is completed on discharge and is sent to the referring physician. The summary includes outstanding issues, such as teaching needs. After discharge, all documents are collated and placed in a section of the hospital chart devoted to day hospital admissions.
Preliminary evaluation
Our patient database includes age, sex, major diagnosis (as listed on admission), treatments received, procedures performed, duration of stay, transfers to inpatient care and complications. For this review, we obtained administrative and cost data from hospital reports and from our medical records department.
The day hospital opened July 1, 1996. In 1998/99 the mean age (and standard deviation [SD]) of patients admitted for asthma was 53 (SD 18) years; for patients with COPD it was 70 (SD 9) years. On admission the mean forced expiratory volume in 1 second was 64% of predicted (SD 22%) for patients with asthma and 38% of predicted (SD 14%) for those with COPD. Table 1 shows the increasing use of this facility, particularly for treatment, during the first 3 years of operation. Most patients referred for acute treatment came from the MCI emergency department or urgent care clinic.
Table 1.
The mean number of days per admission remained constant over the first 3 years of operation for patients seen for treatment (2.2 to 2.3 days), whereas it fell from 1.8 to 1.5 days for patients seen for diagnostic testing. The mean number of hours per treatment day increased slightly, from 5.9 to 6.7. Most patients admitted for treatment received intravenous corticosteroid therapy. The proportion of patients sent home with intravenous locks increased to 35% by 1998/99. Over 50% of patients received structured teaching in 1998/99.
The proportion of patients having to stay overnight in hospital fell between 1996/97 and 1998/99. This proportion did not vary by primary diagnosis (asthma v. COPD v. other). Emergency revisits and major complications were uncommon and in some instances were related primarily to diagnostic procedures.
Per diem costs of the day hospital for 1998/99 are summarized in Table 2. The bulk of expenditures were for nursing and clerical support. To place the estimated per diem cost ($172) in some context, the estimated per diem cost of inpatient acute care at our facility during the same period was $244.
Table 2.
The establishment and growth of the day hospital coincided with substantial reductions in inpatient length of stay at our facility (Table 3). This reduction permitted the MCI to close 16 acute care beds, which accounted for 40% of the previous total. Hence, nursing expenditures for inpatient acute care fell from $1 458 000 in 1995/96 to $1 186 000 in 1998/99. During the latter period, nursing expenditures for the day hospital totalled $237 000. There was a marked expansion in specialized asthma and COPD outpatient clinics, catering to the more severely ill members of this patient population. There was also a larger number of unscheduled “emergency” visits, often by patients new to the MCI. In 1998/99, 22% of admissions to the day hospital involved patients who had not been seen at the MCI before the index episode.
Table 3.
Interpretation
Our experience suggests that a respiratory day hospital can provide relatively intensive — albeit “low-tech” — treatment, supervision and support to respiratory patients whose conditions do not permit discharge after emergency department treatment. The therapies administered in the day hospital match those ordinarily provided in emergency departments and on inpatient acute care services. The emphasis on patient teaching and on communication with patients' usual care providers promotes the coordination of care, a major improvement over our previous walk-in facility.
Patients admitted to our day hospital were typically less severely ill than those admitted for inpatient care during the same period. Nonetheless, the intensity of treatment delivered and the fact that most patients were treated on consecutive days suggest that many day hospital patients would otherwise have been admitted to inpatient care. Indeed, many had previously been admitted to our inpatient ward for similar exacerbations.
Our data do not reflect the costs borne by patients and family members. However, the hospital provided medications, meals and, in many cases, transportation, which reduced out-of-pocket expenses. Transportation was identified early on as an important patient concern. This was addressed primarily through the use of taxi vouchers, which now account for $14 000 in annual expenditures. Although we distributed patient satisfaction questionnaires during the initial phase of operation — with strongly positive responses — response rates were inconsistent.
We expected that some patients would inevitably require transfer to overnight acute care. Hence, we relied on the consistent availability of inpatient beds. In larger facilities where an acute care day hospital is contemplated, it might be necessary to reserve several dedicated inpatient beds for such transfers. Otherwise, patients would simply return to the emergency department — a highly inefficient arrangement.
During our first year of operation, the proportion of patients requiring transfer to overnight care exceeded 20%. We determined that those most in need were patients with COPD referred late in the afternoon. We therefore stopped accepting new patients after 4 pm because many needed more than 4 hours of care. When screening potential admissions, physicians were reminded to be vigilant about psychosocial concerns (particularly patients with difficulty coping at home overnight). As patients and staff grew more familiar with our facility, a better “fit” developed. Both patients and practitioners gained a better idea of what to expect and which patients would likely benefit.
The respiratory day hospital has grown to become a mainstay of patient care at the MCI and within the McGill University hospital system. We believe that the success of this program stems from individualized and high-quality respiratory care provided by an experienced multidisciplinary team, rather than from any technical interventions. Hence, we are convinced that similar programs can be equally successful in other settings.
Acknowledgments
We thank Sylvie Belliveau, Jocelyne Bérubé, Antoinette DiRe, Richard DiLallo, Rita Giulione, Louise Lefebvre, Cordelia McNeal, Pierrette Nivoix, Yuka Numata, Isabelle Ouellet, Ziad Rahayel, Lillian Redada, the physicians of the McGill Respiratory Division and the Montreal Chest Institute Research Centre for their assistance with data collection and patient care.
The establishment of the respiratory day hospital at the Montreal Chest Institute was supported by a grant from the Fonds d'innovation of the Ministère de la Santé et des Services sociaux du Québec. Dr. Schwartzman was supported by a Chercheur-Boursier clinicien Award from the Fonds de la recherche en santé du Québec.
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.