

Abstract
Edward Jenner's first treatise in 1798 described how he used cowpox material to provide immunity to the related smallpox virus. He sent this treatise and some cowpox material to his classmate John Clinch in Trinity, Nfld., who gave the first smallpox vaccinations in North America. Dissemination of the new technique, despite violent criticism, was rapid throughout Europe and the United States. Within a few years of its discovery, vaccination was instrumental in controlling small-pox epidemics among aboriginal people at remote trading posts of the Hudson's Bay Company. Arm-to-arm transfer at 8-day intervals was common through most of the 19th century. Vaccination and quarantine eliminated endemic smallpox throughout Canada by 1946. The last case, in Toronto in 1962, came from Brazil.
On Dec. 1, 1796, Dr. John Clinch, a medical missionary at Trinity, then the second largest settlement in Newfoundland, sent a letter to Dr. Edward Jenner in Gloucestershire. Clinch asked for further information about using cowpox pustule matter as a vaccination against smallpox.1 Jenner had vaccinated his first subject only 6 months earlier. By June 1800, when Jenner published his famous pamphlet, An Inquiry into the Causes and Effects of the Variolae Vaccinae, describing his vaccination experiments on 23 subjects, Clinch probably had been vaccinating people in Newfoundland for a year or more.
Jenner and Clinch, both born in 1749, had been classmates at Reverend Dr. Washbourn's school in Cirencester, Gloucestershire, before they went to London together to be pupils of the distinguished surgeon John Hunter.2 Jenner returned to his home area, but Clinch practised 3 years in Dorset near Poole, the main shipping port for Newfoundland. In 1775 Clinch moved to Newfoundland to practise in Bonavista. After 8 years he moved to Trinity, where he also preached the Anglican sermons on Sundays. Jenner's nephew, George Jenner, aiming for a similar church-medicine career, very likely began his medical apprenticeship under Clinch at Trinity in 1789.2
On July 15, 1800, a second shipment of vaccine from Edward Jenner reached Clinch; one of these two vaccine shipments, most likely the first, came via George Jenner, by then the Anglican minister at Harbour Grace, on the intervening peninsula between Trinity and St. John's.2 By the first week of October 1800 Clinch had vaccinated additional people in the adjacent settlements of St. John's and Portugal Cove, and by the end of 1801 he had vaccinated 700 people.2 William R. LeFanu's definitive bibliography of Jenner3 credits Clinch with being the first vaccinator in North America, before Benjamin Waterhouse, who vaccinated his own sons in July 1800 and then popularized vaccination in Boston.4 Sadly, exact dates for Clinch's first vaccinations are unavailable for conclusive proof of his priority. Clinch is honoured by a memorial plaque in Trinity.1
Transportation of cowpox vaccine
How was Jenner's vaccine sent to Newfoundland? Transportation of the vaccine, whether in the form of lymph or dried material, was an uncertain enterprise. It might be stored and transported on narrow pointed slivers of ivory about 3 cm long, called "points," or on squares of glass with a thin coat of gum arabic mucilage.5 Clinch received his cowpox matter from Jenner within quills and on impregnated threads.[1, 2] Colonel George Landmann, living in Quebec City in November 1801, received his "precious yellowish lymph" between small squares of plate glass.6 Dr. John Warren of Boston received it from England "in a closely sealed phial."7
Communal vaccination was made practicable by transferring lymph 8 days after vaccination from the original person vaccinated with cowpox to a succession of people. The longest duration of vaccine transport using children was the 3-year Balmis expedition from Spain that began in 1803.8 The Maria Pita carried 22 orphan boys 3 to 9 years of age, Balmis, a deputy surgeon, 2 assistants, 2 first-aid practitioners, 3 male nurses and the rectoress of a Santiago orphanage. The boys were vaccinated in sequential pairs every 9 or 10 days. At ports along the route to South America and the Philippines, homes were found for the orphans and more children were brought on board. Thereby vaccination "girdled the world."8 In British India only boys of low caste were considered suitable for the purpose.9
Variolation using live smallpox virus
Before Jenner pioneered use of the safer cowpox vaccine, the technique of variolation, or "smallpox inoculation," was an established practice in parts of Asia and Africa. In China, insufflation of dried smallpox crusts into the nostrils caused a less severe form of smallpox than that occurring naturally.5 A second method, of rubbing liquid from a smallpox pustule into a small scratch on the arm, found favour in the rest of the world and reached Constantinople in 1679.10 Either method of variolation provided life-long immunity. These practices were reported verbally to a meeting of the Royal Society in 170011 but were not published in Philosophical Transactions in London until 1713 and 1717.[12, 13]
After Lady Mary Wortley Montagu, wife of the British Ambassador to Turkey, variolated her 6-year-old son at Adrianople on Mar. 18, 1718, Europeans sat up and took notice. On her return to England, Lady Mary gained the support of the Princess of Wales.14 In 1721, 6 condemned convicts, 3 men and 3 women, were inoculated with live smallpox virus in the presence of the royal physicians Sir Hans Sloane and Dr. John George Steigertahl. In return, all 6 lives were spared from hanging. One of the women later lay for 6 weeks in the same bed with a 10-year-old boy with smallpox, to demonstrate her immunity.10
The disease produced by "scratch" variolation was appreciably milder than naturally occurring smallpox: the fever was milder, the disease was of shorter duration, and there were fewer pustules.15 However, fatal smallpox often resulted among contacts, and it was some years before either inoculation of the entire community or isolation of those receiving variolation became standard practice.5 Variolation had a death rate of 2% in the first 8 years of practice through 1729,10 a notable improvement over the 20% to 30% from naturally occurring smallpox, which in that era was encountered at some time in almost everyone's life.5
The first known use of variolation in what is now Canada was in Quebec in 1765.16 In 1769, James Latham, a British military surgeon, instructed by Robert and Daniel Sutton in England, variolated 303 people, including prominent members of English and French families in Quebec City and, later, 200 people in Montreal, without fatality. By the time of his departure in 1770, Latham had variolated 1250 people in Canada.17
To a large extent, British troops in Canada had been variolated. In contrast, several of the 13 colonies, before the American revolution, had passed laws against variolation. Although George Washington's troops were variolated during the siege of Boston, and later the practice was made compulsory for all new army recruits, such was not the case for American troops involved in the assault on Quebec. The severity of the smallpox outbreak among them caused them to retreat in July 1775. "Indeed, smallpox saved Canada for the British Empire."10
In 1796, the authorities allowed the variolation of Mohawk Indians in Upper Canada, and of Indians near Kingston.17 Variolation continued for over half a century after the introduction of smallpox vaccine, effectively ceasing in Canada only by an Act of Parliament in 1853.16
Smallpox in eastern Canada
On Mar. 7, 1803, John Chew, superintendent of the Indian Department at Montreal, forwarded to the Lieutenant Governor of Upper Canada a message dated Feb. 27 from Père Le Noir, missioner of the Abenaquis village at St. Francis, asking "that a doctor be sent to inoculate him and his Indians and save them from the smallpox."3 At the annual meeting of the Royal Jennerian Society, held on Jenner's birthday, May 17, 1804, a survey of the progress of cowpox vaccination throughout the world reported that "The Canadian Indians came down the country many hundred miles to procure the matter and most of their tribe escaped the smallpox."3 Such a statement is evidence that the Indians had received vaccination and not variolation.
On Aug. 11, 1807, Edward Jenner mailed a formal gift of his 1803 book, Address to the Royal Jennerian Society for the Extermination of the Small-pox, to the Chiefs of the Five Nations. This was presented to them at an assembly in Fort George, Upper Canada, on Nov. 8, 1807. The chiefs were just as formal in their acknowledgement:
We send with this a belt and string of Wampum in token of our acceptance of your precious gift, and we beseech the Great Spirit to take care of you in this world, and in the land of spirits.16
Smallpox on the western plains
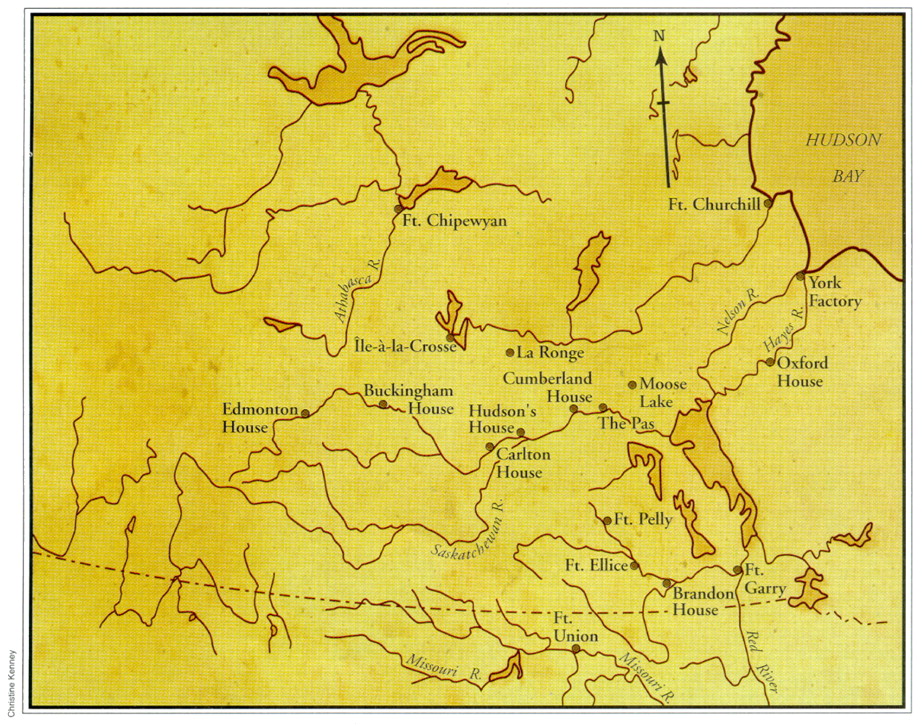
In the west, the worst and most widespread smallpox epidemic came north from the Missouri River in the summer of 1781 (Fig. 1). It reached susceptible aboriginal people, "virgin soil" for the smallpox virus, along the Saskatchewan River by the end of the year.18 Mitchell Oman met some surviving Indians in the Eagle Hills region of present-day Saskatchewan in the fall of 1781; the survivors were "weak and just recovering" from smallpox; Oman "looked into the tents, in many of which they were all dead." When he reached Fort Buckingham (near present-day Elk Point, Alta.), which he had founded a year earlier, "all was solitary silence ... there was no Indian to hunt for us. ... three-fifths had died."19

Fig. 1: Western interior of Canada in 1832. Based on a map from the Hudson's Bay Company Northern Department reproduced by Ray,22 with permission.
William Tomison arrived at York Factory on Hudson Bay on July 2, 1782, confirming news of the epidemic in the interior (Fig. 2). He was followed by 6 canoes of Indians with their season's furs; 3 Indians were ill with smallpox, which proved fatal by July 11th. Immediately, Matthew Cocking sent word to the local "Home Guard" Indians not to visit the fort. Another 3 Indians with smallpox arrived on Aug. 6; Cocking gave them food and medicine and persuaded them to camp 6 km up stream; all 3 died.20 Miraculously, this early effort at quarantine worked; these 6 were the only deaths from smallpox found by the late Dr. William B. Ewart in his careful reading of all York Factory post journals from 1714 to 1946.21 Furthermore, smallpox was unique among all epidemics in arriving at York Factory from the interior (W.B. Ewart; from an unpublished manuscript). In contrast, influenza, measles and scarlet fever were carried inland from Hudson Bay by the annual boat brigades.22

Fig. 2: York Factory in the 1770s, where early quarantine efforts in the summer of 1782 helped to prevent a smallpox epidemic. [Coloured engraving from a drawing by Samuel Hearne.]
Matthew Cocking wrote in August 1782 from York Factory:
I believe never Letter in Hudson's Bay conveyed more doleful Tidings than this. Much the greatest part of the Indians whose Furrs have been formerly & hitherto brought to this Place are now no more, having been carried off by that cruel disorder the Small Pox. ... the whole tribe of U'Basquiou Indians ... are extinct except one Child.23
Between epidemics, individual Hudson's Bay Company post journals rarely provided information about vaccination, but on July 25, 1820, Peter Fidler wrote from Swampy Lake en route from York Factory to his post at Fort Dauphin: "great numbers inocculated [sic] for the Cow Pock in Red River... ."24
A recent assessment of the smallpox epidemic at Cumberland House, 1781-1782, has demonstrated the compassion shown by William Tomison and his men.25 They took dying Indians into their already crowded quarters and provided them with food, shelter, and 24-hour care. They then dug their graves in the deeply frozen ground.
The second great smallpox epidemic again originated on the Missouri River. This time it began with the arrival of the American Fur Company's steamboat at Fort Union on June 24, 1837.26 On Sept. 20, Dr. William Todd, hired as a surgeon by the Hudson's Bay Company in 1816 but now chief factor at the Swan River District, received news of "some bad disease." He guessed correctly that it might be smallpox, and the next day vaccinated 60 Indians in the vicinity of Fort Pelly, using new cowpox vaccine from England, and taught them the technique.[18, 27] Todd sent fresh vaccine to William Small at Carlton House, R. Mackenzie Simon at Île-à-la-Crosse, John Rowand at Edmonton House and Alexander McLeod at Fort Chipewyan.18 John Richards McKay at Fort Ellice vaccinated "all the Indians belonging to the post."27 From Cumberland House, Chief Factor John Lee Lewes extended vaccination to The Pas, Moose Lake and La Ronge. On Feb. 20, 1838, 2 natives whom Lewes had vaccinated 3 days earlier left the post, taking with them on their arms "the means of giving the same to all attached to Moose Lake."28 At Oxford House on Apr. 15, 1838, John Todd described explicitly how arm-to-arm vaccination was performed: "The subjects were vaccinated with fresh serum taken from the previously vaccinated eight days before."29 The northward spread of smallpox was stemmed successfully, despite occasional lack of cooperation and earlier failures from ineffective vaccine.[18, 22]
A third, less serious epidemic occurred in 1870. At Fort Garry, where on Nov. 5 there were as yet no cases of smallpox, an ample supply of vaccine matter arrived by mail on Nov. 27.30 Arm-to-arm transfer was again used successfully, but farther west at Carlton House smallpox once more caused havoc among the Indians. On Jan. 22, 1871, the Board of the Hudson's Bay Company wrote: "[We] notice with deep regret the fearful mortality which has taken place among the Indians and half-breeds throughout the country from the scourge of smallpox."31
Final years of smallpox
Meanwhile, arm-to-arm vaccination remained the common practice in France until 1864 and was popular in Britain until 1881; calf lymph suspended in glycerol then came into use. In Britain the Vaccination Act of 1898 finally prohibited arm-to-arm vaccination.5
Canada owed its vaccine production mainly to an energetic, enterprising general practitioner in Palmerston, north of Belleville, Ont. In response to the 1885 smallpox epidemic in Montreal, Dr. Alexander Stewart founded a vaccine farm; his cows provided a dependable vaccine supply for 31 years. In 1916, the fledgling Connaught Laboratories took over the manufacture of sterile vaccine of uniform, enduring potency.32
Because vaccination and revaccination programs achieved less than perfect coverage, endemic smallpox persisted in Canada until 1946. For example, Saskatchewan had peaks of 598 cases (4 deaths) in 1913 and 961 cases (8 deaths) in 1921 (Fig. 3), the same year that Ottawa reported 1352 cases.[33, 34] In Saskatchewan, the last serious but nonfatal outbreak of 568 cases occurred in 1931, with the last death in 1938 and the last 4 cases in 1943.33

{kind=link}
{kind=link}
{kind=link}
Fig. 3: Number of cases of smallpox in Saskatchewan from 1910 to 1943.
Concerted vaccination campaigns were successful in eliminating endemic smallpox from Canada by 1946, 26 years later than from Norway, Sweden, Denmark and Holland.[5, 34] Nova Scotia had a suspected case in 1949, evidently brought by a visitor from the United States; with rigid quarantine the disease did not spread. The final, laboratory-confirmed case in Canada, in 1962, involved the 15-year-old son of a Canadian missionary who returned to Toronto by air from Brazil.34
In retrospect, variolation and vaccination in turn were impressive achievements. The 10-year smallpox eradication program of the World Health Organization led on schedule to the final case diagnosed in Somalia on Oct. 26, 1977. The entire program cost only $112 million and now saves $1 billion annually in global health expenditures.10
We thank Anne Morton, Head, Research and Reference, and Judith Beattic, Keeper, of the Hudson's Bay Company Archives, Provincial Archives of Manitoba, for their extensive help. The late Dr. William B. Ewart shared his unpublished typescript, "Smallpox at York Factory: Epidemic Disease, Burial Practises, and the York Factory Cemetery," another copy of which has been deposited in the Hudson's Bay Company Archives. Christopher J. Rutty provided background information on the origins of the Connaught Laboratories. Drs. Paul Gully and Paul Varughese, of the Laboratory Centre for Disease Control, Health Canada, provided details of the last person in Canada to have laboratory-confirmed smallpox. Dr. Stan Houston and Adam Houston provided constructive criticism.
Acknowledgments
The Canadian Cancer Society (National) will award $1000 for the best paper on a topic in oncology or cancer control written by a student enrolled in an undergraduate medical program in Canada. Essays should be no longer than 3000 words and will be judged on relevance, originality and scientific merit. The winning paper(s) will be considered for publication in CMAJ.
For more information and submission forms contact Ms. Monika Dixon, Junior Administrator, Essay Prize for Oncology or Cancer Control, Canadian Cancer Society, 10 Alcorn Ave., Suite 200, Toronto, ON M4V 3B1; tel 416 961-7223; fax 416 961-4189; mdixon{at}cancer.ca OR visit their Web site (www.cancer.ca).
DEADLINE: January 28, 2000
Footnotes
-
This article has been peer reviewed.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.