


Abstract
Background: Decisions about organ donation are stressful for family members of potential organ donors. We sought to comprehensively explore the donation process from interviews conducted with family members of patients admitted to pediatric and adult intensive care units in Canada.
Methods: We conducted a qualitative study using semistructured, in-depth interviews with 271 family members asked to make an organ donation decision. We recruited participants from all provinces with an organ donation organization (n = 10), and analyzed themes using a modified grounded theory approach. On the basis of these interviews, suggestions were made by researchers and family members on how to improve the process of organ donation.
Results: We identified 3 main themes and 9 subthemes. Families need more comprehensive support around the time of donation, including having access to someone with shared experiences, support during specific moments as needed and better support during critical transitions (e.g., when the donor body goes to the operating room). The theme of better connection to recipient(s) included receiving information about the donation surgery (e.g., which organs were recovered), establishing connection with recipients (e.g., via social networks or letters) and planned encounters. Support after donation, such as updates on organ transplantation, early mental health checks and continued connection to donor organizations, could be improved. We derived 20 suggestions for improving the organ donation process, derived from interviews with family members of pediatric and adult organ donors.
Interpretation: We found gaps in family support during end-of-life and donation care. Feelings of abandonment, lack of support and poor-to-little follow-up provide the empirical findings needed for hospitals and organ donor organizations to provide better support to donor families.
In Canada, 2 pathways to deceased organ donation exist. Families can be approached about organ donation after either neurologic determination of death or a decision to withdraw life-sustaining therapy. Family is defined by the patient or, in the case of minors or those without decision-making capacity, by their surrogates. They are people who provide support and with whom the patient has an important relationship.1 Families in the intensive care unit (ICU) who experience sudden or traumatic loss of a loved one and then face complex decisions around organ donation have unique experiences, and they depend upon health care professionals to support them throughout the process.2
Each Canadian province has its own registry or method for indicating a person’s intent to donate organs and tissues, with variability in the practices of the different provincial organ donation organizations, particularly about policies for identifying the recipient to donor families.
We aimed to explore the organ donation journey from the perspectives of the family members of potential pediatric or adult organ donors who had consented to organ donation across Canada. We also sought to make suggestions to improve the organ donation process, informed by the data from researchers and family members.
Methods
Study design and setting
We recruited participants through Canadian organ donation organizations, which are not-for-profit agencies responsible for supporting, managing, promoting and facilitating organ donation in all Canadian provinces. We conducted in-depth interviews with family members who were invited to consider organ donation after either neurologic determination of death or a decision to withdraw life-sustaining measures (donation after circulatory death) from their loved one. Family members were eligible for inclusion in the study 2 months to 3 years after they were approached about donation. An earlier publication outlined the detailed study protocol.3 This study is reported using the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220508/tab-related-content).
Each organ donation organization except those in Ontario and Quebec compiled a database of eligible family members, including their names, telephone numbers, address, sex, relationship to the patient, the donation decision and the manner of death determination (neurologic or circulatory criteria). Staff from these organizations contacted the family members by mail to inform them of the study. About 2 weeks after the mailing, the staff telephoned the family members (3 attempts maximum) to explain the purpose of the study and to request their permission to be contacted by research staff. Next, research staff contacted the family members who agreed, to further explain the study and to schedule a telephone interview with those who consented to participate. In Ontario, staff from organ donation organizations contacted family members by telephone within 6 months to 1 year after the patient’s death. In Quebec, letters were sent to eligible family members informing them of the study and requesting a reply by mail if they were interested in participating; only family members who mailed a reply were contacted by the staff from organ donation organizations.
Data collection
Informed by a previous pilot study of experiences of family members in Ontario,4 we developed a semistructured interview guide. An interdisciplinary team of investigators with experience in critical care, palliative care, organ donation, medical education, and sociological and qualitative research methods refined the interview guide. Next, we solicited feedback on the guide from a committee of family members, members of the Canadian Critical Care Trials Group and organ donation leaders representing every organ donation organization in Canada, and revised the guide based on their feedback (Appendix 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220508/tab-related-content).
Members of the research team with specific training and previous experience conducted the telephone interviews following the semistructured interview guide, which was designed to follow a broad but predetermined line of inquiry that was flexible and could evolve as data collection unfolded, permitting exploration of emerging themes. Interviews with family members were extensive: we asked participants to detail the totality of their experience from first learning of the patient’s acute illness, describing the end-of-life process, the organ donation experience and their bereavement. We also solicited their suggestions for improvements to the donation process. If requested, 2 family members were interviewed together, such as a mother and father.
Telephone interviews took place from July 2018 to June 2020, and lasted from 45 to 90 minutes. We continued interviews past the point of saturation (i.e., when existing theoretical categories account for new data) to ensure we interviewed participants from all provinces and we could explore (in subsequent publications) various perspectives, such as comparing adult with pediatric donors. We had estimated that about 250 family members would need to be interviewed.3
Data analysis
All interviews were audio-recorded, transcribed verbatim and uploaded into ATLAS.ti (a qualitative research software program; AtlasTi software, Scientific Software Development) to facilitate data management and analysis. We used a modified grounded theory approach to guide the analysis.5 Our analysis team comprised 5 researchers (A.J.S., S. Sutherland, A.L., B.V-W. and S.V.) who participated in coding meetings to iteratively develop the codebook and make refinements throughout the data analysis process (Appendix 3, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220508/tab-related-content). At first, all team members coded the same transcript separately. They then met to discuss the codes, their definitions and to resolve any disagreements. 6 This process, which took about 4 months, was repeated until the level of agreement among the coders (measured using Krippendorff α) reached a value of 0.858%;7 thereafter, coding was independent. The team had regular email communication and monthly meetings to discuss the coding process, including agreeing on codes that might be created, expanded or collapsed.
We applied qualitative data analysis techniques consistently to the interview data.6 Our analysis included generating a query report from the ATLAS.ti program based on the code “recommendations from families.” Coding followed 3 consecutive stages.5 In the initial stage, the entire team collaborated to code the complete data set. In the focused coding stage, 2 coders (A.J.S. and S. Sutherland) pulled a query report based on the code “family recommendations” and recoded the data. Finally, in the theoretical coding stage, 2 authors (A.J.S. and S. Sutherland) explored topics among the various themes. We achieved triangulation across analysts and participants.
We extracted family suggestions for improving the donation process directly from the data set. Our procedure involved the research team taking the themes and subthemes and writing short, action-oriented statements that could be feasibly implemented in Canadian hospitals. Next, we reviewed the statements with the family member committee by teleconference and then revised if necessary. The final step was a review by all of the authors about the feasibility of implementation and approval of the final set of suggestions.8
Ethics approval
Ten institutional regional ethics boards approved this study (the full list can be found in Appendix 4, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220508/tab-related-content).
Results
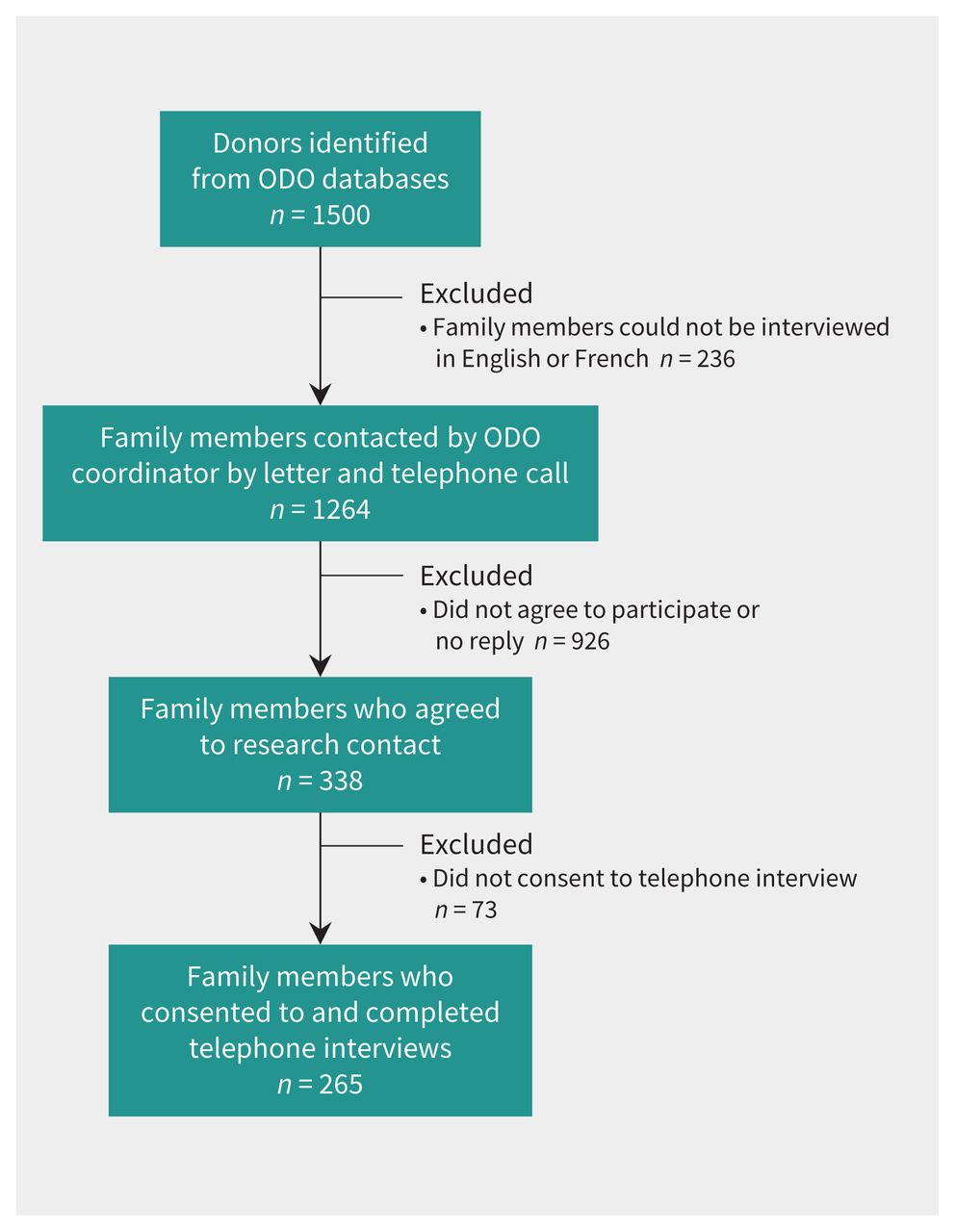
Of all eligible family members, 338 agreed to be contacted by the research team, 271 consented and participated in 265 telephone interviews, and 2 family members participated in 6 interviews (Figure 1). We did not include the family members who declined donation (n = 13) because they did not experience the donation process and could not comment or make suggestions about it. Most of the interviewed family members were women (185 of 258); 112 were parents and 74 were a spouse or partner of the deceased donor (Appendix 5, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220508/tab-related-content). Most organ donors were male (167 of 252); 53 were 19–30 years of age, 46 were 51–60 years of age and 43 were 61–70 years of age. Most had death declared by neurologic criteria (n = 167) (Appendix 6, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220508/tab-related-content).

Flow chart for family member recruitment process. Note: ODO = organ donation organization.
Figure 2 illustrates the 3 broad and overlapping themes and subthemes that emerged from the families’ suggestions to improve the donation process: more comprehensive support around the time of donation, connection to recipient(s) and improving support after donation.

Qualitative themes and subthemes.
Theme 1: more comprehensive support around the time of donation
Many family members expressed the desire for support from people outside of the hospital, specifically from someone who had lived through a similar donation experience, who they could have met with within or outside the hospital (Box 1, quote 1). Other family members explained they would have wanted to spend more time with hospital staff and spoke of how these people could have better helped them (Box 1, quotes 2 and 3).
Participant quotes — Theme: need for a support person (subthemes: shared experiences, specific moments, critical transitions)
Shared experiences
1. … maybe a mom that went through the same thing I did, to talk to, and tell me what’s coming next and what to expect because there is a lot to take in. It’s like, “Okay. I’m losing my son, now you want his organs?” I had time to soak all that in, but it would just be nice to have somebody to sit with you and talk to you. Just mom on mom, not a coordinator, not a doctor, not a nurse. I just don’t think there’s enough support of that nature.
2. The close family members are operating at a mental capacity of 2, like they are not thinking, they are not processing. So, whoever the support person is, they would be very useful, and I don’t have the answer as to who that should be, but maybe more time with that social worker, and by the way, she was useful for us, not only leading up to the decision-making, she was almost immediately, if I remember this right, after they made some hard decisions about the transplant, she circled back and asked if we were okay. Generally, the experience was as good as it could be, but it’s just a lot to figure out.
3. And I think just being able to have people around you that can explain to you what’s going on in a way that you understand. And then to have those support workers just kind of pick up on the body language. That kind of stuff.
Specific moments
4. The doctors didn’t prepare me, maybe because I didn’t ask. I think at that point they assumed, because I’m a nurse in Palliative that I had seen somebody die, but I work in Outpatient Palliative, so I haven’t. The thing that they did say to me was, because it was hard to tell, and he did have some brain function left, there wasn’t actually, like a time … like, they were actually pretty clear that it could take a while ‘cause he still did have some brain function. So that was what they did say. And then I didn’t really ask about, you know, what the physical death would be or look like. So when I … but when I got there and I kind of realized, like, “Shit, this is happening now,” it was actually the … the RT that I talked to. And he told me, like, you know, “This is what will happen,” like, if you … if you feel like he’s uncomfortable, like, let your nurse know. He really walked through what would happen with me, and I’m glad he did ‘cause it was pretty ugh … shocking.
5. After my son died, I couldn’t sleep. The transplant organization does have a website and they do have various articles on grief and I did access some of those. As I mentioned, I couldn’t sleep, so I couldn’t read books, but I could manage short articles. The 1 thing I found searching on my own were some grief podcasts; they are called “grief casts” and they have been really helpful when I am trying to go to fall asleep.
Critical transitions
6. Father: I know my wife said that’s the 1 thing that she wished would have been different was that they took him [baby boy] in and then we were left alone outside the surgical room and never felt so empty and alone.
Interviewer: There was no one? You were completely alone in the hall? Just the 2 of you?
Father: No one, it was just me and my wife in the hallway outside the door.
Interviewer: So, what did you do?
Father: We walked back to the ICU and gathered up our things and left.
7. Here’s the thing, it’s 1:00 in the morning, a blind guy using a cane trying to get out of the hospital after donating his wife’s organs, trying to call Uber … I wasn’t escorted out of the hospital, no one looked after me. It left a little bit of bitterness. It was very disappointing, you know, when I was at ICU, you know, everybody was great; however, that moment when I needed somebody, just to make sure I was safe going home.
8. Nobody told us that he might not die in time. The doctor was so convinced that he was going to die within 15 minutes … I don’t hold that against the doctor, because I recognize that we’re not so perfect and that we don’t always get that right, but what didn’t happen was an explanation. So when they extubated, the whole team was sitting outside. I kept looking at the clock. I cried. I kept saying, “Oh, please God, you take [husband’s name] and and let his organs help somebody if I’m going to lose him.” And, then I go, “What the heck am I doing? I don’t want to lose him.” So it was back and forth. And, it was all in my head as I was sitting, trying to maintain calm in that room. Anyway, when it was over and they couldn’t take his organs, I felt like I’d failed the world. I felt guilt. I felt like we failed somebody, somewhere, many somebodies. The transplant team came in and said, “We can’t use his organs.” Then, they backed out. And I never saw anybody for 3 hours. We were alone in there, not seen for 3 hours.
Note: ICU = intensive care unit, RT = respiratory therapist.
Participant quotes — Theme: connection to recipients (subthemes: awareness of recipient[s] status, mutual connection, planned encounters)
Awareness of recipient(s) status
1. I would like to know who has my daughter’s heart. It’s positive, it’s not a negative thing at all. Organ donation is an ultimately positive thing to do. It doesn’t make the grieving any worse, it makes it easier because there is a positive, there’s not just the end, there is a new beginning. Even just to know that the surgery went well, and they are doing fine. That’s all really. To know that it worked. I don’t need to know where you live or your phone number, no, I just want to know that you are doing fine, that’s all I need to know.
2. I need to know as her mother, yes, she donated her heart and we transplanted and that person is still living and is doing very well. Yes, somebody got a kidney. Somebody else got a kidney. Somebody got a double lung transplant because of your daughter and you know what, they’re living an active life. I need to know that, okay. I need to know, it’s my right. (Crying) I just think, it would be nice if you could let me know if those organs were successful.
3. Yeah, it’s been a while, but the first year I did call, and they got back to me saying that, for the kidneys, that they were doing good, but then the eyes and tissue are at another place and so for the eyes you need to call another number. I never got an answer. For the lungs they said, “Oh, I’ll get someone to call you back,” but I never did get a call back and I find that is poor. I shouldn’t be the one calling, someone should call me and say something.
Mutual connection
4. But 1 thing I wish is that [province name] would have some sort of mechanism where both the recipient and the donor opted in that after, I don’t know, 5 years or something that we could actually communicate and know who the other person is if both of us opted in.
5. I harassed them to please let me get into contact with them [recipients]. And I had to wait a year. I found that was too long. I had to wait a year to be able to correspond with my son’s recipients, which I did. I got a response from 2 of them. My only issue with this procedure is that they and we are anonymous. I’m addressing somebody who has my son’s organs and I don’t know their name? It’s like I’m dealing with an entity.
6. The organ donation organizations are very bureaucratic, very rule bound and I mean rightly so, but there’s got to be some more humanity in there, in that these people want to be connected. I think perhaps that their policies need to be revisited. I know I did get a letter from someone who got, I believe it was his kidney, and I got it right away. I was quite shocked actually and, unfortunately, I got it at a time where I didn’t write back because I couldn’t. And I keep thinking about it now and it has been 3 years and I really should write this person back and apologize for taking so long, but it was just too soon for me to answer. I was too emotional still.
Planned encounters
7. I think if both sides want to know, I don’t see why there would be the harm in it. We were interviewed for doing organ donation the last 2 years in a row, promoting organ donation on the Organ Donation Week, and the recipients on the other side sent us a picture last year of their little girl who wrote us a note saying, “Thank you for saving my daddy.” I do want to be more involved because I think it’s important. And I’ve often been, like, “Hey, this isn’t working. Something needs to change here.” And, the recipient and I even talked. We laughed, he thought I might tell him, “You can’t drink. That’s my son’s kidney.” And, we had a little chuckle about it because that’s where, yes, there are some people would go too far and I get that and in that case that’s where they would cut the ties if it’s not working, you know. But that should be an option. The impact it had was, okay, you get your little letters of how they’re doing. I can phone in and say, “Any updates, please?” And they’ll update, but they won’t tell me who. They just say “Patient with the heart doing well,” da-da-da-da-da. But the, the lung recipient passed away from, I forget.
During specific moments, family members who worked in the medical field (most were nurses) described the importance of not assuming that they did not need support (Box 1, quote 4). Many family members suggested the need for a support person. When such a person was not available, participants became proactive in searching for other supports at various points in the donation journey (Box 1, quote 5), such as online supports, books, and national and international organizations (Appendix 7, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220508/tab-related-content). Some family members were surprised to be left without any support at critical transitions during the donation process (such as when the body was taken to the operating room, or when donation after circulatory death did not happen and when leaving the hospital after the surgery; Box 1, quotes 6–8).
Theme 2: connections with recipients after the donation
Family members’ wishes varied from wanting to know that the patient’s organs had made a difference (most) to wanting to connect directly with organ recipients through a planned or facilitated meeting (Box 2, quotes 1 and 2). In some instances, family members reported having taken the initiative to try to find out the status of the donated organs (Box 2, quote 3).
Some family members, recognizing the importance of maintaining confidentiality, asked that there be opportunities to connect with recipients if both parties agreed (Box 2, quotes 4 and 5). Family members’ desire to connect with recipients is complex because it is often bound up with the grieving process. Family members reported that they wanted to know if the recipients were doing well while they were coping with the loss of the donor (Box 2, quote 6). A small number of family members described a desire to develop a relationship with the organ recipients (Box 2, quote 7).
Theme 3: improving support after donation
Suggestions made by family members for improving the donation process included more follow-up support from the organ donation organization, hospital or another organization working with bereaved people, more follow-up immediately after leaving the hospital (e.g., to find out what organs were recovered; Box 3, quotes 1 and 2) and instituting early checks on mental health (Box 3, quotes 3 and 4). Participants also described the importance of meeting families where they are in their grieving process. Many family members described the feeling of not being ready for donor-related communication and donor events at 2 and even 3 years after the death of their family member, in particular, the annual donation ceremony sponsored by some organ donation organizations, but wanting to attend when they were ready (Box 3, quotes 5 and 6).
Participant quotes — Theme: follow-up (subthemes: organ recovery update, early mental health checks, continued connection)
Organ recovery update
He [transplant surgeon] called and told us everything. He explained what organs they could use and what they couldn’t and told us where they went and that was fine. I needed that information.
For me, it doesn’t make the grieving worse, it makes it easier because there is a positive, there is not just the end, there is a new beginning…even just to know that the surgery went well, and they [recipients] are doing fine.
Early mental health checks
I think it honestly should be like not mandatory but it should be very much like, “Hey, you’ve just lost somebody, here’s your contacts, this is your appointment,” kind of deal because I don’t know how I would have processed any of it without a therapist.
When you go through a trauma, people are shoving cards at you from all over the place. I would have 2, 3 cards in my pocket. But when you actually go to physically look for help, it’s months away!
Continued connection
It would be nice if it came from the organization to the family just to check in. And then especially for siblings, I think siblings really get lost in the world of grief of a loved one. There are more supports for the parents or if it’s a husband or a wife.
I did receive 2 invitations to go to the donor ceremony. I was invited twice. I mean he died in December so personally I just wasn’t ready to go. I didn’t go to the first one and I didn’t go to this last either. I do want to go but I just wasn’t ready. I’m not sure if the invitations have been sent out for this year but she said she’d let me know, but I never got that phone call back. I assume I have to wait till next year now because it’s been a couple of months and I haven’t heard.
Suggestions for improvement
Based on the interviews, researchers and family members developed 20 practice-based suggestions to guide improvement in the donation process (Table 1).
Twenty suggestions for improving the organ donation process, derived from interviews with family members of pediatric and adult organ donors
Interpretation
We explored the experience of family members across Canada who had agreed to deceased organ donation for adult or pediatric patients. We considered their experience from first learning of the patient’s traumatic event, the end-of-life process, the organ donation experience and their subsequent bereavement.
Our findings have direct implications for how to improve the organ donation process for families. We found gaps in the way families are supported during end-of-life and donation care. Families need better support at key moments during the donation process, such as when their family member’s body is taken to the operating room, when organs cannot be used and when decision-makers are leaving the hospital after donation surgery. Participants’ feelings of abandonment and poor-to-little support after their family member’s organ donation provides empirical evidence needed to catalyze structured changes in the way hospitals and organ donation organizations provide support to families of organ donors. Many family members indicated that they wanted to play a role in supporting future donor families. There is evidence from other health care domains, such as patients with cancer9–11 or spinal cord injury,12–14 that such an approach works well; there should be little resistance to endorsing and advancing this practice for transplant donation.
The impact of the organ donation process on the psychological well-being of family members of organ donors during the months to years after the donor’s death has received little attention.15 Unable to find or access the support they needed, at times family members created their own informal support groups and networks. Family members who consent to donation have a high risk of complicated bereavement that exceeds 50% in some studies.16–19 However, consenting to organ donation itself is not a risk factor for complicated bereavement and may even be beneficial insofar as it helps families make sense of a tragic death.18,19 Some risk factors for complicated bereavement, such as negative experiences during the time at the hospital21 and poor understanding of the concept of brain death,22–27 could be addressed by interventions offered during or after the time at the hospital.2,20 Therefore, we have suggested that enhancing bereavement support should be the cornerstone of any organ donation program,2,28 and our findings suggest that a long-term individualized approach is needed.
We found that families need access to various resources, on an “as needed” basis, rather than at prespecified times. Health care professionals supporting families need to appreciate the unique and individual journeys of donor families as they cope with bereavement.28 In an earlier study,4 we learned that the provision of empathic care supports families in the decision-making process and aids in their bereavement.29
We, and others,12,15,28,30–32 have found that donor families want to know how organ recipient(s) are doing, to confirm that their loved one’s organs had made a difference. Some family members were concerned that donation organizations were withholding information in the name of protecting the anonymity of the recipients but, in so doing, added to their grief. Most donor family members and recipients are satisfied with anonymous correspondence, finding it comforting and reassuring, whereas some family members feel the need to meet organ recipient(s) in person. 31,33,34 Family members who want but do not receive information about the transplantation outcomes experience more stress throughout their grief as well as uncertainty about their decision to donate.35 Our study confirms that for some family members, a lack of information about transplantation outcomes added stress to their bereavement and grief.30,31
Limitations
We did not evaluate whether there were differences in the views of subgroups, such as family members of pediatric compared with adult donors, and we did not approach families who decided not to agree to donation. We conducted the interviews in English and French, so we were unable to include the experiences of family members who were not comfortable speaking those languages. Other studies have shown that different cultures view donation differently.36,37 We did not obtain an in-depth understanding of diverse cultural perspectives about donation in Canada, including from Indigenous family members. There may have been selection bias in who agreed to be interviewed; it is possible that family members who had relatively good experiences and trusted researchers, or those who had bad experiences and wished to describe them, were more likely to agree to participate.
Conclusion
We have provided information that health care professionals and policy-makers can use to ensure more family and patient-centred rhetoric and protocols. We have generated suggestions on how to improve the donation process that were derived directly from interviews with donor families. Some of these suggestions are not new, and hospitals and organ donation organizations should urgently implement them.
Acknowledgements
The authors extend their sincerest appreciation to all the family members who took the time to share their thoughts and experiences. The authors thank all participating organ donation organizations for incredible contributions in helping to organize this study and, most importantly, for reaching out to family members to invite them to participate in an interview — BC Transplant; Transplant Manitoba, Gift of Life Program and Winnipeg Regional Health Authority; New Brunswick Organ & Tissue Donation Program; Critical Care Organ Donation Program (Nova Scotia); The Organ Procurement Exchange of Newfoundland and Labrador and the Eastern Regional Health Authority; Trillium Gift of Life Network; Transplant Québec; Saskatchewan Transplant and Saskatchewan Health Authority; and Southern Alberta Organ and Tissue Donation Program. This manuscript underwent an internal peer-review process with the Canadian Critical Care Trials Group, and the authors are greatly appreciative of the contributions made by both Dr. Kirsten Fiest and Dr. John Basmaji.
Footnotes
Competing interests: Sam Shemie has received consultant fees from Canadian Blood Services. Sean Keenan is the Medical Director of Donation Services at BC Transplant. Andreas Kramer is the medical director for the Southern Alberta Organ and Tissue Donation Program and lead, Southern Alberta Specialist in End-of-Life Care, Neuroprognostication, and Donation Program. Sonny Dhanani is the chair of the Canadian Blood Services Deceased Donation Advisory Committee and associate director of the Canadian Donation and Transplantation Research Program. He has also received a stipend from Ontario Health as a Hospital Donation Physician, Trillium Gift of Life, and holds U.S. Patent No. 10, 172, 569. Ken Lotherington is an employee of Canadian Blood Services. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Aimee Sarti, Stephanie Sutherland, Sam Shemie, Sean Keenan, Matthew Weiss, Kim Werestiuk, Andreas Kramer, Joann Kawchuk, Stephen Beed, Sonny Dhanani, Ken Lotherington, Mary Gatien, Kim Parsons, Peter Nickerson and Pierre Cardinal contributed to study conception, design and acquisition of data. Maureen Meade, Jennifer Chandler, Giuseppe Pagliarello and Michaël Chassé contributed to study conception and design. Aimee Sarti, Stephanie Sutherland, Angele Landriault, Brandi Vanderspank-Wright and Sabira Valiani contributed to data analysis. Aimee Sarti and Stephanie Sutherland contributed to drafting of the article. All of the authors contributed to interpretation of the data, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was financially supported by Canadian Blood Services.
Data sharing: As this data is purely qualitative, the authors do not publicly share the database (as stipulated by their research ethics board).
Disclaimer: Canadian Blood Services receives funding from the provincial and territorial Ministries of Health and the federal government through Health Canada. The views expressed herein do not necessarily represent the views of the federal, provincial or territorial governments or of Winnipeg Regional Health Authority. Canadian Blood Services is a national, not-for-profit charitable organization that manages the supply of blood and blood products in all provinces and territories in Canada (with the exception of Quebec), and oversees the Canadian Blood Services Stem Cell Registry. In 2008, Canadian Blood Services became responsible for national activities related to organ and tissue donation and transplantation, which includes national system development and operation of interprovincial organ-sharing programs. Canadian Blood Services is not responsible for the management or funding of any Canadian organ donation organization or transplant program.
- Accepted July 14, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

