


A 44-year-old man presented to the outpatient department of our hospital having had 4 days of anterior chest pain. He had a history of hyperuricemia and gout flares, which had been diagnosed clinically without any evidence of crystal deposition. He had been prescribed colchicine and febuxostat, but had stopped febuxostat several months previously. He had had chest pain twice in the 4 months before the current visit; in both instances, the pain subsided within 7 days with use of diclofenac. Investigation of these episodes of chest pain with blood tests (including cardiac troponin level), electrocardiography, echocardiography and chest computed tomography (CT) showed no abnormalities, including no erosions or hyperdense tophi in the ribs.
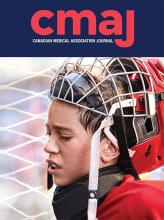
We saw no erythema or swelling on the patient’s chest wall or peripheral joints. However, we elicited marked tenderness at the second to fourth costal cartilages on his left side and saw a tophus on his right lateral malleolus (Figure 1A). His serum uric acid and C-reactive protein levels were 10.1 (reference range 2.6–7.0) mg/dL and 0.74 (reference range 0.00–0.14) mg/dL, respectively. Dual-energy CT showed monosodium urate crystal deposition in costal cartilages (Figure 1B). We diagnosed costochondral gout. After the flare subsided, the patient resumed febuxostat and continued colchicine. We followed him for 5 months and he had no further flare.
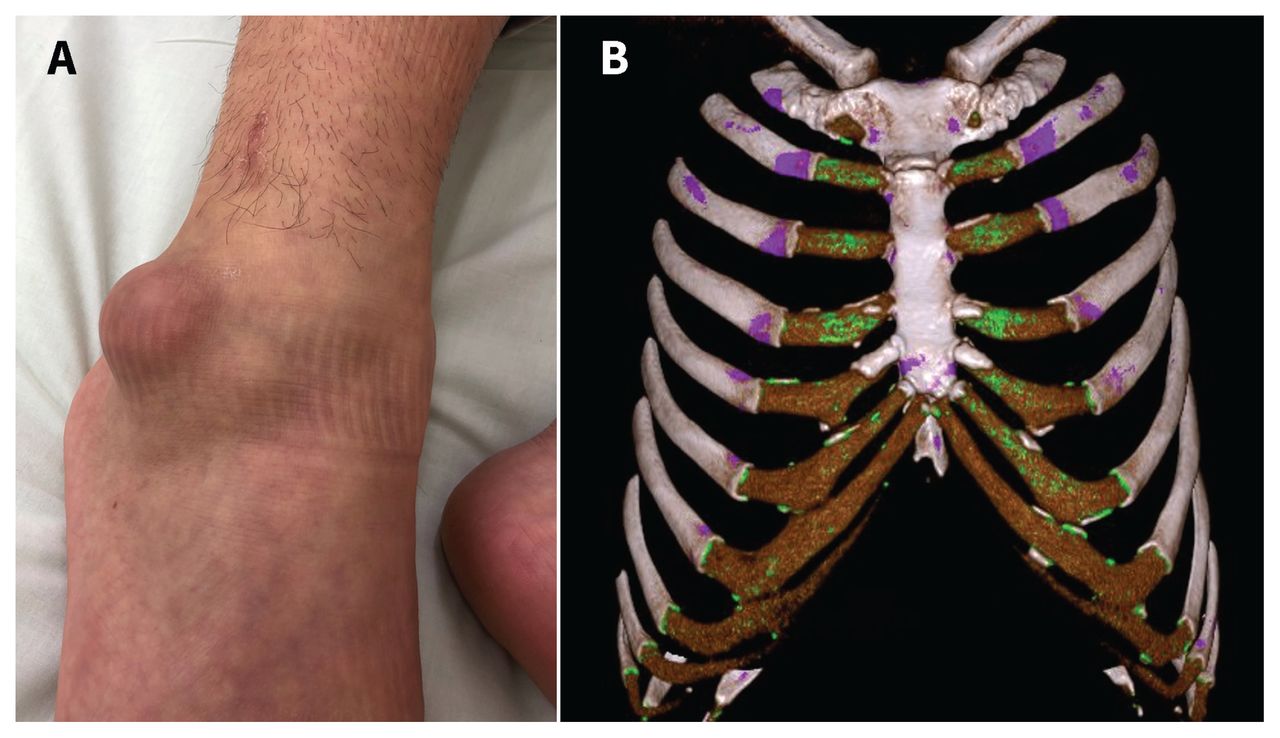
(A) A tophus in the right lateral malleolus of a 44-year-old man with costochondral gout. (B) A dual-energy computed tomography scan showed monosodium urate crystal deposition (green) in costal cartilages.
Chest pain with tenderness on physical examination suggests that the pain originates in the chest wall. The differential diagnoses include costochondral gout, costochondritis, rheumatic diseases (e.g., fibromyalgia, relapsing polychondritis, rheumatoid arthritis, axial spondyloarthritis), septic arthritis and neoplasms.1 Diagnosing gout can be challenging when synovial fluid is unavailable or when atypical sites are involved, including costal cartilage and intervertebral discs. Dual-energy CT is a useful diagnostic test because it detects urate crystal deposition,2,3 but additional tests may be needed to rule out other diseases.
Footnotes
Competing interests: Yukinori Harada reports receiving a manuscript fee from PRECISION Inc., outside the submitted work. No other competing interests were declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue
{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

