


Abstract
Background: Cannabis use among pregnant and lactating people is increasing, despite clinical evidence showing that cannabis use may be associated with low birth weight and childhood developmental deficits. Our objective was to understand why pregnant and lactating people use cannabis and how these motivations change across perinatal stages.
Methods: Using qualitative, constructivist grounded theory methodology, we conducted telephone and virtual interviews with 52 individuals from across Canada. We selected participants using maximum variation and theoretical sampling. They were eligible if they had been pregnant or lactating within the past year and had decided to continue, cease or decrease their cannabis use during the perinatal period.
Results: We identified 3 categories of reasons that people use cannabis during pregnancy and lactation: sensation-seeking for fun and enjoyment; symptom management of chronic conditions and conditions related to pregnancy; and coping with the unpleasant, but nonpathologized, experiences of life. Before pregnancy, participants endorsed reasons for using cannabis in these 3 categories in similar proportions, with many offering multiple reasons for use. During pregnancy, reasons for use shifted primarily to symptom management. During lactation, reasons returned to resemble those expressed before pregnancy.
Interpretation: In this study, we showed that pregnant and lactating people use cannabis for many reasons, particularly for symptom management. Reasons for cannabis use changed across reproductive stages. The dynamic nature of the reasons for use across stages speaks to participant perception of benefits and risks, and perhaps a desire to cast cannabis use during pregnancy as therapeutic because of perceived stigma.
Cannabis use by pregnant and lactating people is increasing, though it is difficult to establish the prevalence of cannabis use in pregnancy. Reported prevalence varies from 2% to 36%, depending on the methodology used to detect use, the population studied and the definition of use.1–12 Pregnant people have reported using cannabis to manage pregnancy-related conditions (e.g., nausea, weight gain, sleep difficulty)13–19 and pre-existing conditions (e.g., mental health, insomnia, chronic pain),13,14,18 as well as to improve mood, mental, physical and spiritual well-being,16,18 provide pleasure and manage stress.13–16 Recent systematic reviews have not found empirical data on reasons for cannabis use during lactation.20,21
Evidence is still emerging about clinical outcomes related to cannabis use during pregnancy and lactation, and well-controlled studies are lacking.22–24 The available evidence is limited by reliance on self-reported data about dose, composition and timing of exposure, the changing nature of tetrahydrocannabinol levels in cannabis over time, and a lack of studies that control for known confounders such as polysubstance and tobacco use.25–31 The available evidence does suggest that cannabis use during pregnancy may be associated with complications such as low birth weight, childhood neurodevelopmental outcomes and preterm birth.22–24,32,33 Very few studies have analyzed the outcomes associated with cannabis exposure through breastmilk, with 1 study suggesting decreased infant motor development and another showing no effects on developmental outcomes.34–36 Given the potential harms identified, and in the absence of high-quality evidence available to guide practice, most clinical guidelines recommend abstinence from cannabis during pregnancy and lactation.37–39
People who perceive benefits from cannabis may wish to or may be motivated to continue using it through pregnancy and lactation, however. Counselling that explores the reasons patients are considering cannabis use and suggests related alternatives or harm reduction strategies has been identified as a helpful strategy to minimize potential harm.13,40,41,42 Such an approach requires that clinicians understand the motivations to use cannabis before pregnancy, during pregnancy and during lactation. We sought to explore why people use cannabis during pregnancy and lactation.
Methods
Study design
Given the socially constructed nature of concepts such as risk, safety and health, which are key to the phenomenon under study, we conducted a qualitative study using constructivist grounded theory.43
Participants
Eligible participants were English-speaking Canadian residents who were at least 19 years old, had been pregnant or lactating in the past year, and had used cannabis during this time or in the 3 months before pregnancy.
Sampling and recruitment
We recruited participants through study advertisements posted in prenatal clinics, on Facebook and on other social media forums relevant to parenting and pregnancy (e.g., Babycentre, The Bump). Some existing participants circulated study invitations to others. Advertisements directed potential participants to an online screening and consent form, which allowed us to select participants for diverse demographic and experiential features (i.e., maximum variation sampling) and then for features identified as theoretically relevant during initial phases of analysis (i.e., theoretical sampling).43,44
Data collection
We collected data via semi-structured interviews by phone or videoconference from November 2020 to March 2021. Four authors (A.P., J.P., S.T., M.V.) who were trained in qualitative interviewing and were unknown to participants conducted the interviews. Three interviewers were research assistants (A.P., J.P., S.T.) and 1 was the faculty member leading the study (M.V.). Interviewers wrote memos throughout the project that detailed emerging insights and documented ideas for interview guide refinement and preliminary analysis. These memos contributed to reflexive conversations and the formation of an audit trail. Interviews were transcribed verbatim and deidentified.
We developed the interview guide (Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211236/tab-related-content) based on 2 recent systematic reviews.21,42 We piloted and refined the guide within the research team, composed of people with clinical, maternal and cannabis expertise. Interviewers asked participants to discuss their cannabis use in the 3 months before their most recent pregnancy, during pregnancy and lactation. We revised the interview guide as the study progressed to pursue areas identified as theoretically relevant.
Data collection proceeded past the point of theoretical saturation (i.e., when existing theoretical categories can account for new data43,45) to collect additional interviews from people with characteristics deemed theoretically relevant to confirm saturation.
Data analysis
We conducted data analysis concurrently with data collection, and followed a staged process from initial open coding to focused coding.43 Four authors (A.P., J.P., S.T., M.V.) completed initial coding independently. They compared their insights and devised a focused coding framework. Focused coding occurred in multiple stages. First, we sought to describe and categorize reasons for use, and then we organized those reasons by individual trajectories through the use of a matrix analysis to code per participant.46 The lead author (M.V.) led coding, and 4 authors (M.V., A.P., J.P., S.T.) operationalized the framework with regular input from the rest of the team (D.G., R.L., S.M.) We achieved triangulation across analysts and participants.
We used QSR NVivo to manage the data. We used a modified member-checking approach by sharing findings from initial stages of analysis with participants, asking them to reflect on whether our interpretation resonated with their experiences. We did not return transcripts or findings from the final analysis to participants.
Ethics approval
This study was approved by the Hamilton Integrated Research Ethics Board (#10976). All participants provided informed consent.
Results
Fifty-two people participated in this study, including 51 women and 1 nonbinary individual. Demographic information is available in Table 1. Interviews lasted about 30 (range 12.5–67) minutes. At the time of the interview, 30 participants were pregnant and 22 were lactating. Thirty-one had other children, and we encouraged these participants to discuss their cannabis decision-making as it related to previous pregnancies. All 52 participants used cannabis before pregnancy and 30 continued to use cannabis during their current or most recent pregnancy. Thirty-three participants discussed lactation, either with their current or a previous child. Of these, 28 used cannabis during lactation.
Participant demographics
Participants described 3 categories of reasons for using cannabis (Table 2). Categories included sensation-seeking (i.e., recreational, to create an altered state or mood), symptom management (i.e., to alleviate a medical condition) and coping (i.e., to alleviate unpleasant aspects of life). Participants often offered multiple reasons for use that spanned more than 1 category. Patterns of use varied according to reproductive stage (Figure 1). Many participants described reasons for use before pregnancy in each of the 3 categories, which shifted in pregnancy, when all but 1 participant reported that they used cannabis for symptom management. Reasons given for use during lactation, however, resembled the prepregnancy distribution. Table 3 provides illustrative quotes for the findings.
Categories of pregnant and lactating people’s reasons for using cannabis
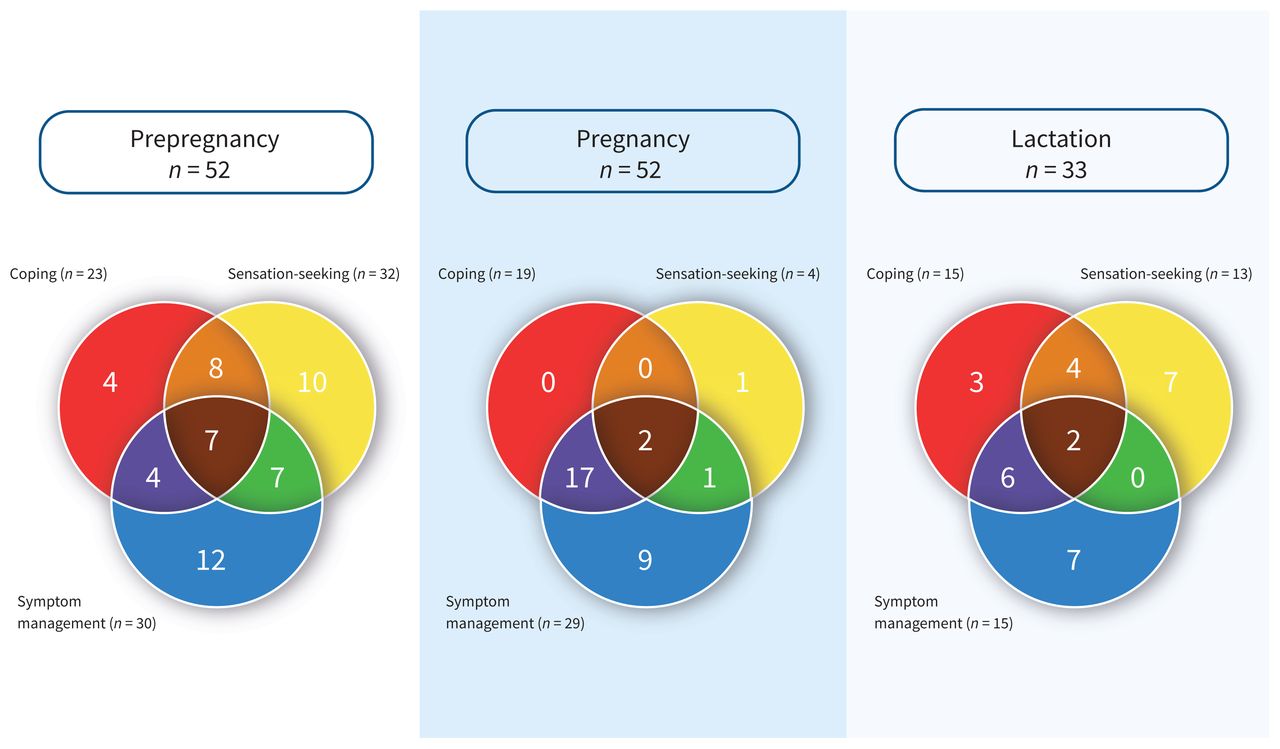
Reasons for using cannabis in each stage of reproduction, and overlap in reasons for use. Each Venn diagram depicts the number of participants who described their use as pertaining to a specific category at the described stage of reproduction. Each of the 3 categories is represented by a primary-coloured circle. The overlapping areas represent the number of participants who described their use as pertaining to multiple categories.
Illustrative qualitative data to support description of cannabis use at each stage of reproduction
Prepregnancy
All 52 participants described using cannabis before pregnancy, for a variety of reasons. Sensation-seeking was the most common reason for use before pregnancy (Figure 1). A similar proportion of participants also reported using cannabis for some type of symptom management before pregnancy. Most frequently, this was self-directed, although 11 participants reported discussing their use of cannabis for symptom management with a health care provider. Many of these participants had a current or former medical authorization, although most preferred to procure cannabis independent of the medical authorization process. Another large group of participants used cannabis before pregnancy for coping with the unpleasant or difficult aspects of life, typically to improve sleep quality, to relax or to alleviate mild anxiety. More than half of participants offered multiple reasons for cannabis use that spanned all categories.
Pregnancy
During pregnancy, motivations for cannabis use changed. Twenty-two participants stopped using cannabis upon learning they were pregnant. Most of these participants abstained because of the potential for harm to the developing fetus. Others ceased because of stigma, guilt, affordability, desire to remain alert and sober, and potential interference with other medications.
The 30 participants who continued to use cannabis during pregnancy offered different reasons for use during pregnancy than before pregnancy (Figure 1). Twenty-nine participants described using cannabis for symptom management. Most commonly, this was self-directed use to manage pregnancy-related nausea and vomiting. Many participants found cannabis to be more effective than pharmaceutical remedies, and variously supplemented and substituted it for prescribed medication.
Participants frequently described using cannabis for coping purposes, alongside symptom management. Sensation-seeking was described by only 4 participants, 3 of whom also explained they were using cannabis for symptom management as well as for coping. The only participant to offer sensation-seeking as her sole reason for use during pregnancy explained that she used cannabis only twice while pregnant.
Lactation
During lactation, cannabis use patterns reverted to resemble those described before pregnancy. Of the 33 participants who discussed lactation (i.e., breastfeeding, chestfeeding or pumping), 28 chose to use cannabis during this time. Sensation-seeking, symptom management and coping reasons were described in proportions that were similar to prepregnancy use (Figure 1). Four participants described their desire to use cannabis as influencing their decision to cease or to not initiate lactation.
For most participants, lactation represented a return to prepregnancy reasons for cannabis use. Descriptions of use for symptom management and coping reasons very closely resembled those given for using cannabis before pregnancy, with the addition of coping with the physicality, stress and monotony of parenting a newborn. Some participants commented that cannabis was more effective than pharmaceutical medication for managing symptoms. When describing cannabis use for sensation-seeking purposes, many participants compared it to use of alcohol, as a way to relax and unwind at the end of the day.
Individual trajectories
We noted little concordance between the reasons for use articulated in separate stages by individual participants (Figure 2); however, we identified 2 consistent profiles of use transitions. The first profile described sensation-seeking users who abstained during pregnancy. The second profile described participants who used cannabis for symptom management across all 3 stages for persistent conditions not related to pregnancy (e.g., depression, chronic pain). However, the most consistent pattern we identified was changing reasons for use across the 3 stages. For example, some participants who described their use as purely sensation-seeking before pregnancy described it as related to symptom management during pregnancy. Others who used it for symptom management before pregnancy stopped using altogether during pregnancy, sometimes resuming during lactation.

Illustration of variation in individual reasons for use across reproductive stages. This Sankey diagram shows the change in individual reasons for cannabis use between the stages of prepregnancy, pregnancy and lactation. Sensation-seeking is represented in yellow, symptom management is in blue, and coping is in red. The secondary colours indicate participants who described overlapping reasons for use. For example, the orange line represents people who described sensation-seeking (yellow) and coping (red) reasons for use; purple represents those who described both symptom management (blue) and coping (red) reasons for use. Participants who offered all 3 reasons for use (sensation-seeking, symptom management and coping) are represented in brown. Black indicates a participant did not use cannabis in that stage. In the lactation column, white indicates that a participant did not discuss lactation, either because they chose not to breastfeed or chestfeed, or because they had not yet given birth.
Interpretation
Individual reasons for using cannabis were dynamic between reproductive stages, even among participants using cannabis to manage symptoms of chronic conditions. The changing nature of the way participants described their reasons for using cannabis during pregnancy and lactation speaks to their perception of benefits and risks, and may reflect a desire to lessen stigma by casting use during pregnancy as therapeutic.13
Our findings have very little resonance with evidence on motivations for cannabis use identified in nonpregnant populations, suggesting that motivations for use during pregnancy and lactation are unique. Of the reasons for cannabis use during pregnancy and lactation described by our participants, only 3 reasons (i.e., enjoyment, coping, sleep) correspond to domains of the Comprehensive Marijuana Motives Questionnaire.47 The reasons for use provided by our participants more closely match those identified in studies of medical cannabis use, such as for controlling pain, anxiety, depression, muscle spasms, nausea or appetite, and for sleep, with many using cannabis to manage multiple symptoms.48–50
Some of our findings are consistent with surveys of pregnant people. Surveys of people in the United States who used cannabis during pregnancy indicate they do so to relieve stress, anxiety, chronic pain, nausea and vomiting.51,52 However, our participants differed from those in previous survey studies because nearly half of the survey participants disclosed recreational cannabis use during pregnancy, which may reflect a difference in populations, greater social desirability bias in qualitative interviews or both.
Participant-reported benefits, particularly in relation to treating severe nausea symptoms, suggest the value of future research investigating the efficacy of cannabis in relieving symptoms that are not responsive to currently available medical therapy. This is an important gap in the literature about this understudied population.
Few studies have explored reasons for use during lactation, although some have noted that many people are likely to resume their prepregnancy use after giving birth.53,54 Our findings provide empirical support for this observation, with many participants who used cannabis ceasing use during pregnancy and resuming in lactation. Another small group of participants chose to cease or forego lactation to resume cannabis use. This is worrying, given that the benefits of lactation are well established.55–57
We suggest that our findings have 3 implications for practice. First, for some people, cannabis is perceived as helpful for symptom relief and coping during pregnancy. Recognizing the perceived benefits of cannabis use may assist clinicians in finding opportunities to offer alternatives or substitutes.42 These conversations may present an opportunity to weigh the perceived benefits of cannabis use, the emerging data about the potential for harm, and the safety and efficacy of other alternatives.22–24 In some cases, the pregnant or lactating person may decide that continued cannabis use has self-perceived benefits for their health and the health of the pregnancy that outweigh the risk of potential harm to the fetus or infant. Second, postpartum people will often wish to resume cannabis for similar reasons to their prepregnancy use. Counselling about the risks and benefits of cannabis use during lactation may help to reduce harm. Exploring reasons for cannabis use during lactation and offering alternatives may benefit those who would otherwise choose to avoid or abbreviate lactation in order to resume cannabis use. Third, the way people explain their cannabis use during pregnancy and lactation is dynamic. This could be an artifact of social desirability bias, or it may reflect the changing nature of symptoms across pregnancy and lactation. Counselling approaches that specifically address patients’ motivations for use, focusing on symptom management and harm reduction, may be most likely to be successful.
Limitations
We conducted this study in Canada, where recreational and medical cannabis is legal and readily available. Qualitative researchers do not strive for representative samples, but rather for samples of participants likely to yield rich experiential data. Our sample was diverse in age, geography, education and occupation, but, similar to other studies of medical cannabis, participants were more likely to be white or Indigenous than the general population.48,50 Findings may have limited transferability to pregnant and lactating people with other racial identities.
Conclusion
Of the 52 pregnant and lactating people interviewed in this qualitative study, those who chose to use cannabis during pregnancy did so mainly to manage symptoms of pregnancy and pre-existing conditions. During lactation, participants used cannabis for reasons that resembled their prepregnancy use, including for enjoyment and relaxation. A small number of participants ceased lactation to resume cannabis use. Most participants who ceased using cannabis during pregnancy or lactation did so because they were worried about the risk of harm to their fetus or infant. Recognizing that many pregnant and lactating people endorse cannabis for symptom management may provide opportunities for clinicians to discuss alternatives that have been proven safe for this population.
Footnotes
Competing interests: From April to December 2019, Janelle Panday was employed as a research analyst at PureSinse Inc. (a licensed cannabis producer), outside the submitted work. She does not hold any remaining financial or personal connection to PureSinse, which is no longer in operation. Since May 2021, after her involvement in data collection for this study, Janelle Panday has been employed as a freelance research coordinator by Avail Cannabis Clinics, a privately owned network of medical clinics, outside the submitted work. She is compensated hourly for this work, which involves preparing and submitting ethics applications, and does not have any other financial interests related to Avail or its research. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Meredith Vanstone, Devon Greyson, Robin Lennox and Sarah McDonald designed the study. Meredith Vanstone, Shipra Taneja, Anuoluwa Popoola and Janelle Panday collected data. All authors contributed to data analysis. Meredith Vanstone drafted the manuscript. All authors critically revised it, gave approval of the final version to be published and agree to be accountable for all aspects of the work.
Funding: This research was funded by the Canadian Institutes of Health Research (FRN 167972). Sarah McDonald is supported by a Tier II Canada Research Chair.
Data sharing: This data set is not available for sharing. When participants consented to participating in the study, they did not consent to access to transcripts or data beyond the research team. Some complete qualitative transcripts may be identifiable. Readers are welcome to contact the corresponding author for further clarification.
- Accepted October 19, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Coping with Cannabis During Pregnancy: Trajectories of Depression, Stress, and Cannabis Use across the Prenatal Period
- Prenatal exposure to THC vapor influences feeding, bodyweight and glucose metabolism under both basal conditions and following high fat diet
- Acute care related to cannabis use during pregnancy after the legalization of nonmedical cannabis in Ontario
- Correction to "Reasons for cannabis use during pregnancy and lactation: a qualitative study"
More in this TOC Section
Similar Articles
Collections

