


A 36-year-old woman presented to the emergency department with a 9-month history of abdominal pain accompanied by rectal bleeding during menstruation. She was otherwise well. Her pelvic and rectovaginal examination, as well as findings on transvaginal ultrasound, were unremarkable. T2-weighted magnetic resonance imaging (MRI) showed a hypointense wall thickening in the sigmoid colon. We suspected endometriosis and our differential diagnosis included inflammatory bowel disease and cancer. Colonoscopy showed a 30-mm submucosal lesion with a red, nodular surface in the sigmoid colon (Figure 1A). Pathologic examination of biopsy specimens was nonspecific. Subsequently, biopsies performed during a second colonoscopy just before the patient’s menstrual phase showed an endometriotic gland and stroma, positive for estrogen receptor (Figure 1B). We diagnosed intestinal endometriosis. Our patient preferred to avoid long-term hormone therapy and accepted the risk associated with laparoscopic sigmoidectomy. Laparoscopic exploration showed no other endometriotic implants.
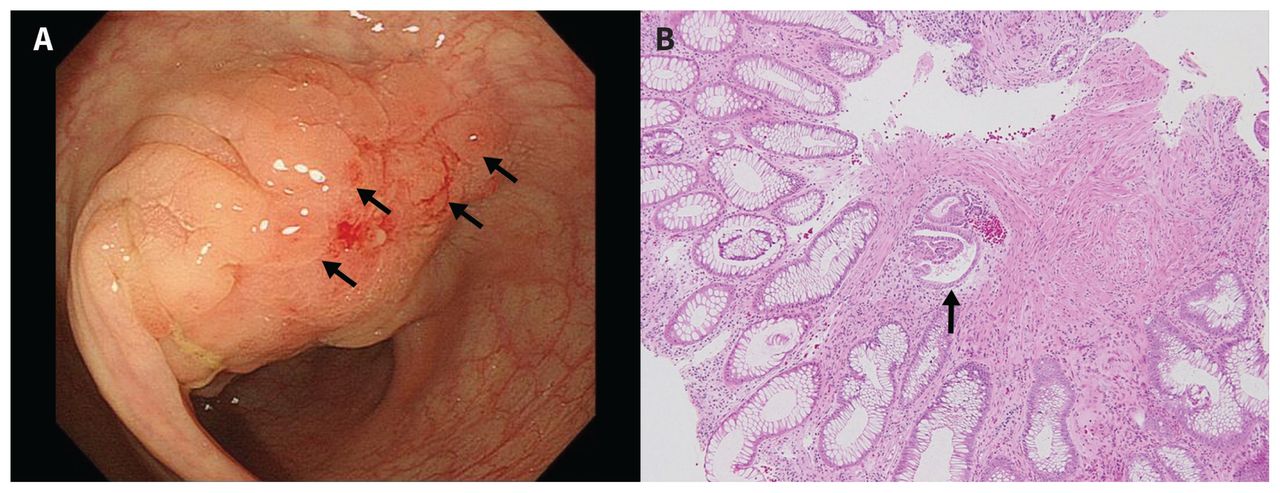
(A) Endoscopy image showing reddish nodules (arrows) atop a 30 mm submucosal lesion in the sigmoid colon of a 36-year-old woman. (B) Biopsy image obtained just before the patient’s menstrual phase, showing a gland and stroma of endometrium (arrow) (hematoxylin and eosin stain; original magnification ×100.
Intestinal endometriosis occurs in 5%–15% of women with endometriosis, and as was the case with our patient, about 20% of women with intestinal endometriosis do not have pelvic endometriosis. 1 The rectosigmoid colon is involved in 3 out of 4 patients with intestinal endometriosis. Although MRI and transvaginal ultrasound are sensitive diagnostic modalities for intestinal endometriosis, definitive diagnosis requires a biopsy. Endoscopic biopsies frequently yield insufficient tissue because the mucosal involvement is sparse.2 We performed endoscopic biopsies just before the menstrual phase, when endometriotic tissue is at its peak. First-line treatment of endometriosis is hormonal, but surgery may be performed for severe intestinal stenosis or to accommodate a patient’s preference. The rate of recurrence after surgery is about 10%.3
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

