


A previously healthy 34-year-old woman was admitted to hospital for new mucocutaneous eruptions leading to severe odynophagia. One week before admission, she had experienced a cough with generalized malaise, confirmed by radiography as community-acquired pneumonia (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.190850/-/DC1). An emergency department physician in urgent care prescribed amoxicillin–clavulanic acid, a medication she had taken previously without incident. Within 48 hours, she experienced vaginal discomfort with labial erythema and edema. She was thought to have vulvovaginitis, and fluconazole was prescribed by an emergency department physician on a repeat assessment. The vaginal lesions progressed, with development of oral mucosal lesions and papular lesions on her trunk and upper and lower extremities (Figure 1). After a third assessment, her family physician prescribed acyclovir for possible varicella infection. Worsening mucocutaneous eruptions and resultant odynophagia led to hospital admission.
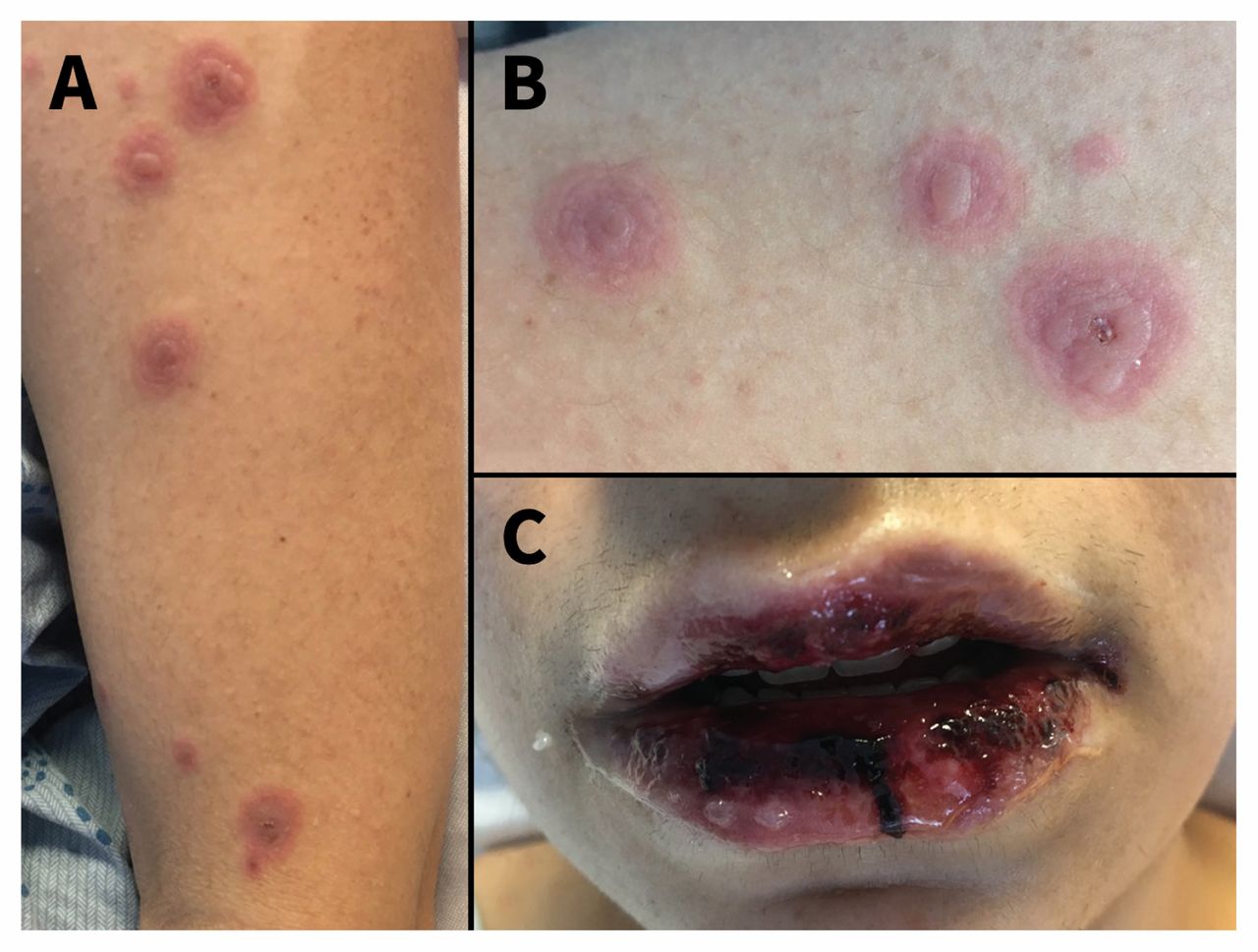
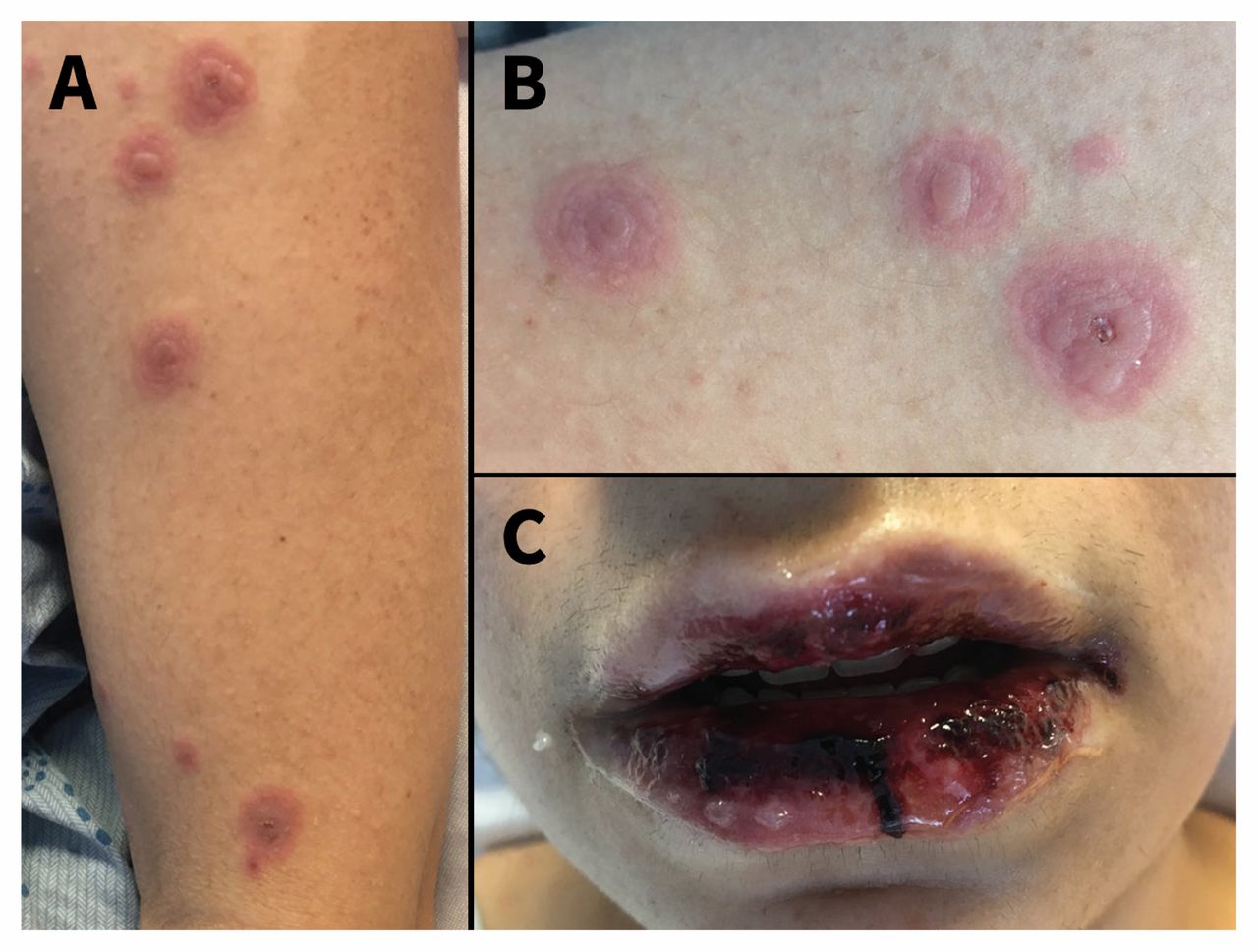
Images of cutaneous (A and B) and oral mucosal (C) lesions of a 34-year-old woman after admission to hospital. The cutaneous lesions have the distinctive target rings with a raised central area (often referred to as a blister). Oral and vaginal (not shown) mucosal involvement was also present, with inflammation and sloughing.
A diagnosis of erythema multiforme major secondary to Mycoplasma pneumoniae infection (confirmed by polymerase chain reaction testing of a nasopharyngeal swab) was made. The patient’s prior antimicrobials were discontinued, and azithromycin was started given the earlier incomplete coverage and ongoing cough and malaise. Prednisone was also started given her substantial mucosal involvement. Her lesions showed early resolution, and she was discharged home after 9 days.
Erythema multiforme is an acute, immune-mediated condition affecting the skin and mucosal surfaces.1 By definition, less than 10% of the body surface area is affected. The disease is typically self-limiting. The most common causes include infection such as herpes simplex and mycoplasmal infection (> 90% of cases), autoimmune conditions and medications.2 In our patient, amoxicillin–clavulanic acid was considered as a possible cause but was inconsistent with the rapidity of development of her mucocutaneous symptoms. Patients may present with distinctive papular target lesions less than 3 cm in size distributed over the extremities and trunk, which typically appear 3–14 days after exposure.3 In the minor variant, patients have involvement of no or 1 mucosal site, whereas those with the major variant have extensive mucosal involvement (≥ 2 sites) and systemic symptoms, such as fever and arthralgia.4 Systemic glucocorticoid therapy may be used, although evidence remains poor,3,5 and, typically, conservative management is required.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

