


A 4-year-old nonverbal boy with autism-spectrum disorder, presents with a 6-month history of gradually refusing to eat preferred foods, intermittently hitting his abdomen for 1 month, lethargy and no bowel movement for 5 days. He currently eats crackers, chicken nuggets and dirt. His diet is supplemented with 2 bottles of pediatric nutrition drink per day. He has lost 6 kg over the last 6 months (weight 12.8 kg, < 3rd percentile; height 99.5 cm, 25th percentile).
What further history is needed?
A detailed dietary and medical history with an emphasis on gastrointestinal symptoms will clarify the diagnosis in this patient. Abdominal pain in nonverbal children with autism-spectrum disorder may manifest as self-injurious behaviours, aggression, sleep disturbances and unusual posturing.1 Alarm symptoms for abdominal pain include substantial vomiting and diarrhea, gastrointestinal blood loss, unexplained fever and deceleration of linear growth.2 Gastroesophageal reflux disease may present with feeding refusal, history of wheezing, hematemesis, dysphagia, regurgitation, hoarseness and recurrent coughing. In addition, medications such as stimulants, antacids and phenobarbital may affect gut motility and food intake.1 Physicians should ensure that feeding disturbance is not due to dieting, religious fasting or lack of food availability.
What physical findings will help with the diagnosis?
Facial swelling may indicate a dental abscess or cavities. The presence of angular stomatitis, koilonychia and pallor may indicate iron deficiency anemia. Constipation should be considered in the presence of a spinal dimple or tuft of hair, distended abdomen, palpable mass, skin tags, anal fissures or perianal erythema and, if a rectal examination is possible, fecal mass, explosive stool on withdrawal of finger or occult blood in stool.1 On auscultation of the lungs, wheezing or stridor may indicate gastroesophageal reflux disease. Abdominal pain localized to the right upper or lower quadrant may suggest an organic cause such as cholecystitis or appendicitis.
What diagnoses should be considered?
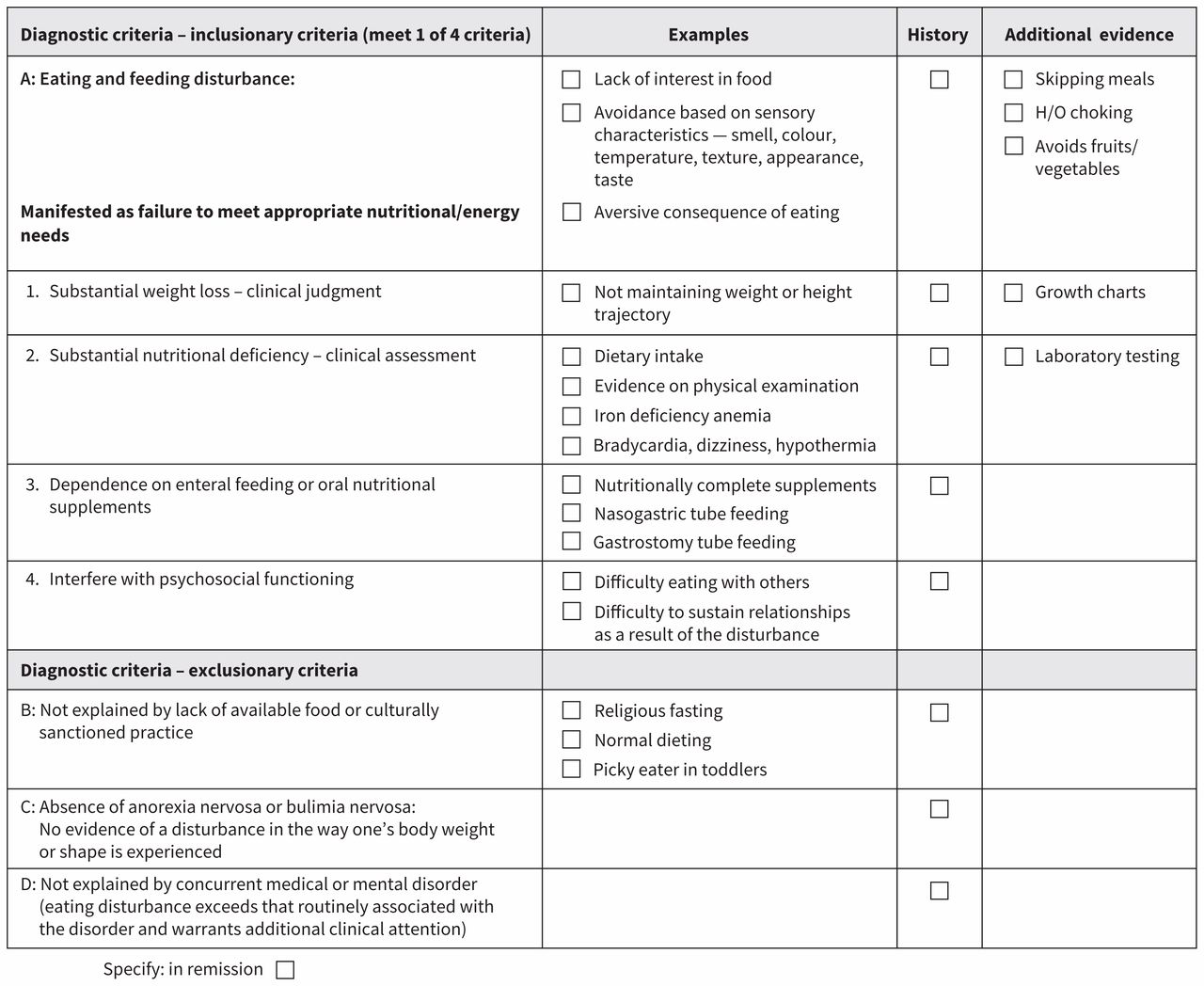
One diagnosis to consider in this patient is constipation. Given the patient’s history of restricted diet, weight loss and use of nutritional supplement, avoidant/restrictive food intake disorder is also likely (Figure 1).

Diagnostic checklist for avoidant/restrictive food intake disorder.7 Note: Checklist created by the author. H/O = history of.
Are investigations needed?
Food selectivity may lead to inadequate intake of calcium, protein, vitamin D, zinc, vitamin B12 and iron, and poor bone growth.3 If iron deficiency anemia is suspected, a complete blood cell count, tests for iron and ferritin levels, and a blood smear should be considered.4
For patients who respond to treatment for functional constipation, no investigations are required. However, for those in whom repeated treatment is ineffective, assessment of thyroxine, thyroid-stimulating hormone, calcium, lead and celiac disease antibody levels should be considered.1 Routine abdominal radiography is not indicated if large stool are found on rectal examination. However, in a child who is difficult to assess, a plain abdominal radiograph might be useful in identifying bowel gas patterns and retention of stool.
What treatment is indicated?
Food selectivity is best managed by behavioural intervention based on applied behavioural analysis. Modified cognitive behaviour and family-based therapy have shown promising results as treatment options for avoidant/restrictive food intake disorder.5
Pharmacotherapy for constipation includes lactulose (70% solution), sorbitol (70% solution) or polyethylene glycol 3350.1 Owing to variable tolerability, pharmacotherapy should be supplemented with nonpharmacological interventions including parent education, toileting regimen, use of positive reinforcers and dietary modification.
Is a referral necessary?
In this patient, referral to a multidisciplinary feeding team is warranted given the chronicity of disordered feeding behaviours in autism-spectrum disorder. This resource may not be available in some communities; therefore, a referral to a registered dietitian and behaviour consultant, or occupational therapist or speech and language pathologist to implement feeding strategies to increase food variety and volume and to monitor growth is suggested. Referral to a gastroenterologist should be considered if the child is unresponsive to treatment to address constipation through dietary modification and pharmacotherapy.6
Case revisited
On abdominal examination, the patient had no masses but did have discomfort in lower left quadrant. Rectal examination was unsuccessful. He was hemodynamically stable. Abdominal radiography showed fecal mass in the colon and rectum. Results from laboratory testing were as follows: hemoglobin 95 (normal 107–134) g/L, iron 3.85 (normal 5.2–26.6) μmol/L and ferritin 10.8 (normal 13.7–78.8) μg/L. The patient was diagnosed with constipation, iron deficiency anemia and avoidant/restrictive food intake disorder (he met 3 of the 4 inclusionary criterion A and none of the exclusionary criteria; Figure 1).7
The patient was prescribed elemental iron (6 mg/kg/d for 4 months) and polyethylene glycol 3350 (1 g/kg/d for 3 days, followed by a maintenance dosage of 1 g/kg/d for 14 days) with follow-up and referral to a feeding clinic.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The clinical scenario is fictional.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

