


Primary Sjögren syndrome can affect multiple organ systems, and initial presentations may vary greatly in symptomology.
Electrolyte abnormalities, particularly hypokalemia, must be considered in patients presenting with generalized weakness.
In cases of type I renal tubular acidosis, consideration must be given to identifying the underlying cause, particularly autoimmune diseases and drugs.
Atypical causes, including autoimmune disorders, should be considered with a history of rapid cognitive decline.
A 71-year-old woman presented to the emergency department with a fall resulting from generalized weakness. Her medical history included hypothyroidism (levothyroxine 0.05 mg daily), hypertension (amlodipine 5 mg daily) and depression (venlafaxine 37.5 mg twice daily), all well managed in the community. Her spouse described an 8-month history of cognitive decline before her fall. This had begun with difficulties in simple tasks such as forgetting passwords and making bookkeeping errors, but progressed to disorientation, word-finding problems, visual hallucinations and dependency in all instrumental activities of daily living and some activities of daily living. Her appetite was reduced and she had lost 4.5 kg in the month before admission.
On examination, the patient was thin and disoriented. Her conversation was tangential and she had difficulty following instructions. We noted major weakness in all her extremities with no focality, such that she was unable to walk without assistance. Her reflexes and plantar responses were normal. Her examination was otherwise unremarkable.
Investigations showed a serum potassium of 1.2 (normal range 3.5–5.5) mmol/L, with associated electrocardiogram changes (Figure 1) and a phosphate of 0.32 (normal range 0.81–1.58) mmol/L. Inflammatory markers were also mildly elevated: her erythrocyte sedimentation rate was 28 (normal < 10) mm/h, C-reactive protein 26 (normal < 10) mg/L, creatine kinase 1455 (normal < 250) U/L, and troponin I 582 (normal < 15) μg/L. The results of her other routine investigations were normal (including complete blood count, remaining electrolytes, creatinine, urea, glucose and thyroid-stimulating hormone).

Electrocardiogram in a patient with serum potassium of 1.2 mmol/L. Black arrows show U-wave in lead aVF and multiple ST-segment depressions in leads aVL, V3–V6.
We postulated that her weakness was secondary to profound hypokalemia and began oral and intravenous potassium supplementation. Although this helped to improve her generalized weakness, she remained persistently hypokalemic (2.5–3.5 mmol/L) with a nonanion gap metabolic acidosis (bicarbonate persistently between 14 and 20 mmol/L). Urine studies were consistent with a type I renal tubular acidosis, showing an elevated transtubular potassium gradient (16), urine potassium concentration (23 mmol/L), as well as positive urine charge (+17). We started her on amiloride (a diuretic that inhibits epithelial sodium channels and consequently reduces potassium excretion) and potassium citrate. This helped stabilize her serum potassium concentrations and her strength improved, suggesting her weakness was secondary to her hypokalemic state.
In order to determine whether her type 1 renal tubular acidosis was primary (hereditary) or secondary (medication-induced, autoimmune or hypercalciuric conditions), we reviewed her history and conducted relevant investigations; we excluded hereditary, and medications-related and hypercalciuric conditions.
Upon further questioning, the patient described having dry mouth for months but no notable ocular symptoms, dental caries, arthralgias or skin changes. Given no other explanation for her hypokalemia, and in light of her elevated inflammatory markers, we tested the patient for autoimmune conditions associated with type I renal tubular acidosis, of which Sjögren syndrome is a potential cause. Surprisingly, Schirmer test was highly positive (i.e., no tear production), as was autoimmune testing for Sjögren (antinuclear antibody 1:320, anti-Ro52 1534 CU, anti–SS-A > 1375 CU and anti–SS-B 141 CU, normal < 20 CU). Testing for anti-neutrophil cytoplasmic antibodies, rheumatoid factor (< 10 IU/L) and anti–cyclic citrullinated peptide antibodies (< 16 U/mL) (serological markers for rheumatoid arthritis), as well as anti–double stranded DNA (< 12 IU/mL) and anti-Smith (< 20 IU/mL) (markers for systemic erythematous lupus), was all negative. On further inquiry, we found that the patient had undergone rheumatologic investigations 17 years earlier, which were negative (for which the indication remains unclear).
Based on these findings, we established a diagnosis of primary Sjögren syndrome in accordance with the 2017 American College of Rheumatism/European League Against Rheumatism criteria (specifically, 3 points for anti–SSA/Ro positive and 1 point for the positive Schirmer test).1
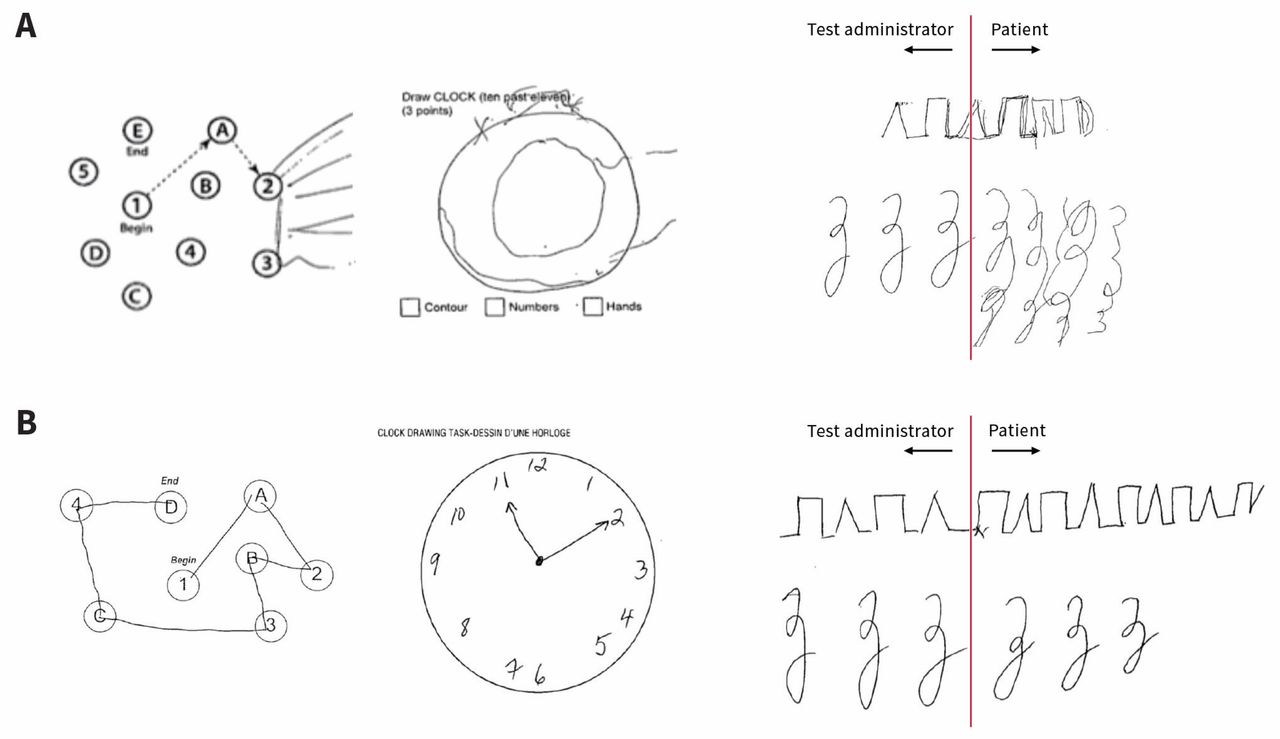
We also investigated the patient’s cognitive decline. A Montreal Cognitive Assessment test showed substantial visual–spatial dysfunction (9/30, Figure 2). Neurological computed tomography imaging was unremarkable, but brain magnetic resonance imaging (MRI) showed periventricular and subcortical white matter changes suggestive of small vessel disease, possibly consistent with a vasculitic process. An electroencephalogram was noncontributory. A lumbar puncture, although negative for a panel of infectious causes, Creutzfeldt–Jakob disease and paraneoplastic antibodies, showed oligoclonal immunoglobulin bands in the cerebral spinal fluid — a finding occasionally noted in patients with Sjögren.

Cognitive testing before (A) and after (B) beginning corticosteroid therapy, patient’s drawings (v. test administrator’s).
We started the patient on prednisone (40 mg daily) and with this, her type I renal tubular acidosis, visual hallucinations and cognitive status substantially improved. She was discharged home for follow-up after a 3-week stay in hospital.
Discussion
Sjögren syndrome is a chronic, multisystem autoimmune condition, typically affecting the exocrine glands and resulting in the classic sicca symptoms of dry eyes and mouth. This is owing to the infiltration of lymphocytes into secretory glands. Other organ systems, including skin (xerosis), endocrine (primarily thyroid), musculoskeletal (arthralgias and myalgias), renal (renal tubular acidosis) and neurologic (both peripheral and central disease), may also be involved (Box 1).2
| System | Symptoms |
|---|---|
| Constitutional | Fatigue |
| Cardiac | Pericarditis, heart block |
| Dermatological | Xerosis, Raynaud phenomenon, cutaneous vasculitis, annular erythema |
| Exocrine | Sicca symptoms (dry mouth and eyes), parotid gland swelling |
| Gastrointestinal | Dysphagia, dyspepsia, nausea, pancreatic disease |
| Hematological | Cytopenias, increased risk of lymphoma |
| Musculoskeletal | Arthralgias, myalgias |
| Neurological | Both central and peripheral manifestations |
| Renal | Renal tubular acidosis, tubulointerstitial nephritis |
| Respiratory | Lymphocytic interstitial pneumonitis |
The incidence of primary Sjögren syndrome remains low, with estimated rates of 3–5/100 000, most commonly presenting in the fourth and fifth decade of life.3 Several studies have noted that incidence of Sjögren in older adults (age > 65 yr) ranges from 6% to 14%,3 with an estimated 9:1 predilection in women.3
The pathogenesis of Sjögren syndrome remains unclear, but both genetic and infectious causes may be involved. It is also highly associated with other autoimmune diseases (defined as secondary Sjögren), and the incidence varies broadly.3 In systemic erythematous lupus, the incidence has been shown to be as high as 20%, while the incidence in patients with rheumatoid arthritis may be as high as 30%. Thus, concurrent rheumatological diagnoses, particularly systemic erythematous lupus and rheumatoid arthritis, must be considered when assessing a patient for a possible diagnosis of Sjögren syndrome. Although Sjögren syndrome is considered a chronic disease, one recent survey of a large Spanish cohort found that 13% of primary Sjögren diagnoses were associated with life-threatening, systemic disease, such as lymphoma, pulmonary and renal involvement.4
The management of Sjögren syndrome is both conservative and pharmacologic.5 Ocular, oral and constitutional symptoms require tear and saliva replacements, good oral hygiene — including fluoride supplementation — and regular physical activity. Corticosteroids remain the mainstay of therapy, but disease-modifying anti-rheumatic drugs such as hydroxychloroquine, methotrexate or cyclosporine may be of benefit. The role of biologics still remains weak and should be evaluated on an individual basis, particularly in individuals with concurrent rheumatological diagnosis.5
Our patient had few symptoms other than dry mouth to suggest a diagnosis of Sjögren, and her only other autoimmune disease was hypothyroidism (which is associated with Sjögren2). Only through investigating her hypokalemia and renal tubular acidosis did we identify Sjögren syndrome as a possible cause.
Renal manifestations of Sjögren syndrome remain poorly defined, with a wide prevalence of up to 70% depending on type of renal injury.7 Tubulointerstitial nephritis is most commonly found on biopsies, and can manifest with pathologies including a distal (type I) renal tubular acidosis, isolated hypokalemia and nephrogenic diabetes insipidus. In extreme cases, Sjögren-related potassium wasting may lead to hypokalemic paralysis.8 Our patient, although not paralyzed, was very weak on admission to hospital and had trouble walking, which most likely led to her fall.
Although a distal renal tubular acidosis may be the presenting feature in Sjögren syndrome, it can be attributed to several other causes, including other autoimmune diseases, medications (particularly nonsteroidal anti-inflammatory drugs), and hypercalciuric conditions. Therefore, patients with a confirmed type I renal tubular acidosis should be investigated fully (Box 2).6,7,11 Management typically requires treatment of the underlying condition, and in the case of potassium wasting mediated by Sjögren syndrome, corticosteroids and other immunosuppressive agents. Amiloride and potassium citrate (which we used in our patient) have also been noted to be effective.8
Causes of type I renal tubular acidosis6,7,11
Primary
Idiopathic/sporadic
Genetically transmitted disease
Autosomal dominant and recessive variants
Marfan syndrome, Ehlers–Danlos, Wilson disease, Fabry disease
Secondary
Medications or drugs
Amphotericin B
Lithium
Ibuprofen
Ifosfamide
Foscarnet
Toluene
Autoimmune conditions
Sjögren syndrome
Systemic erythematous lupus
Rheumatoid arthritis
Thyroiditis
Primary biliary cholangitis
Hypercalciuric conditions
Idiopathic hypercalciuria
Hyperparathyroidism
Hypervitaminosis D
Medullary sponge kidney
Sarcoidosis
The neurologic manifestations of Sjögren syndrome are wide ranging. The peripheral nervous system may be affected in up to 25% of patients,9 including sensory neuropathies of the limbs, cranial neuropathies and autonomic dysfunction. Central findings are more controversial, with a wide range of presentations from seizures, cerebellar dysfunction, psychiatric manifestations and cognitive impairments.10,11 There are no definitive tests that can be used to conclusively confirm central involvement with Sjögren disease. Analysis of cerebral spinal fluid has been shown to have oligoclonal banding, lymphocytosis and elevated immunoglobumin levels.12 Imaging (i.e., MRI) has been used, but generally shows nonspecific changes. Thus, central neurologic presentations of Sjögren syndrome remain ill defined, with treatments and reversibility even more elusive.
In our case, in addition to the cognitive dysfunction, the patient had oligoclonal banding present in her cerebral spinal fluid. Large randomized control trials, and specific treatment regimens and guidelines for treating neurologic manifestations of Sjögren are unavailable. Therefore, standard treatment with immunosuppressive therapies, as is given for other autoimmune diseases, continues to be the mainstay of treatment.
Case revisited
Two months after diagnosis and beginning of treatment, repeat cognitive testing showed marked improvement (MOCA 26/30, Figure 2). The patient no longer had visual hallucinations and biochemically, her renal tubular acidosis, hypokalemia and inflammatory markers had resolved. She had regained much of the weight she had lost during her illness and was able to resume her activities of daily living. She was subsequently started on hydroxychloroquine (Plaquenil), but did not tolerate the adverse effects, leading to discontinuation. The patient considered beginning other disease-modifying antirheumatic drugs, including cyclophosphamide, although at present, she remains on prednisone monotherapy with good effect. Although we can conclude that this patient’s presentation was a result of primary Sjögren syndrome, her underlying neurologic features (and their reversibility) will remain a diagnosis of exclusion.
The section Cases presents brief case reports that convey clear, practical lessons. Preference is given to common presentations of important rare conditions, and important unusual presentations of common problems. Articles start with a case presentation (500 words maximum), and a discussion of the underlying condition follows (1000 words maximum). Visual elements (e.g., tables of the differential diagnosis, clinical features or diagnostic approach) are encouraged. Consent from patients for publication of their story is a necessity. See information for authors at www.cmaj.ca.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
Contributors: All of the authors contributed to the conception and design of the work, drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

