


A painful vesicular rash limited to the V1 dermatome of the trigeminal nerve should be considered herpes zoster ophthalmicus until proven otherwise
Herpes zoster has a lifetime risk of 33%, and older adults and patients who are immunocompromised are at higher risk.1 Herpes zoster ophthalmicus occurs in 10% to 20% of cases of herpes zoster, with ocular involvement in 50% of those of herpes zoster ophthalmicus.1 Lesions on the tip, side or root of the nose (Hutchinson sign, Figure 1A) confer a high risk of ocular complications because of the shared innervation by the nasociliary branch of the V1 nerve.2
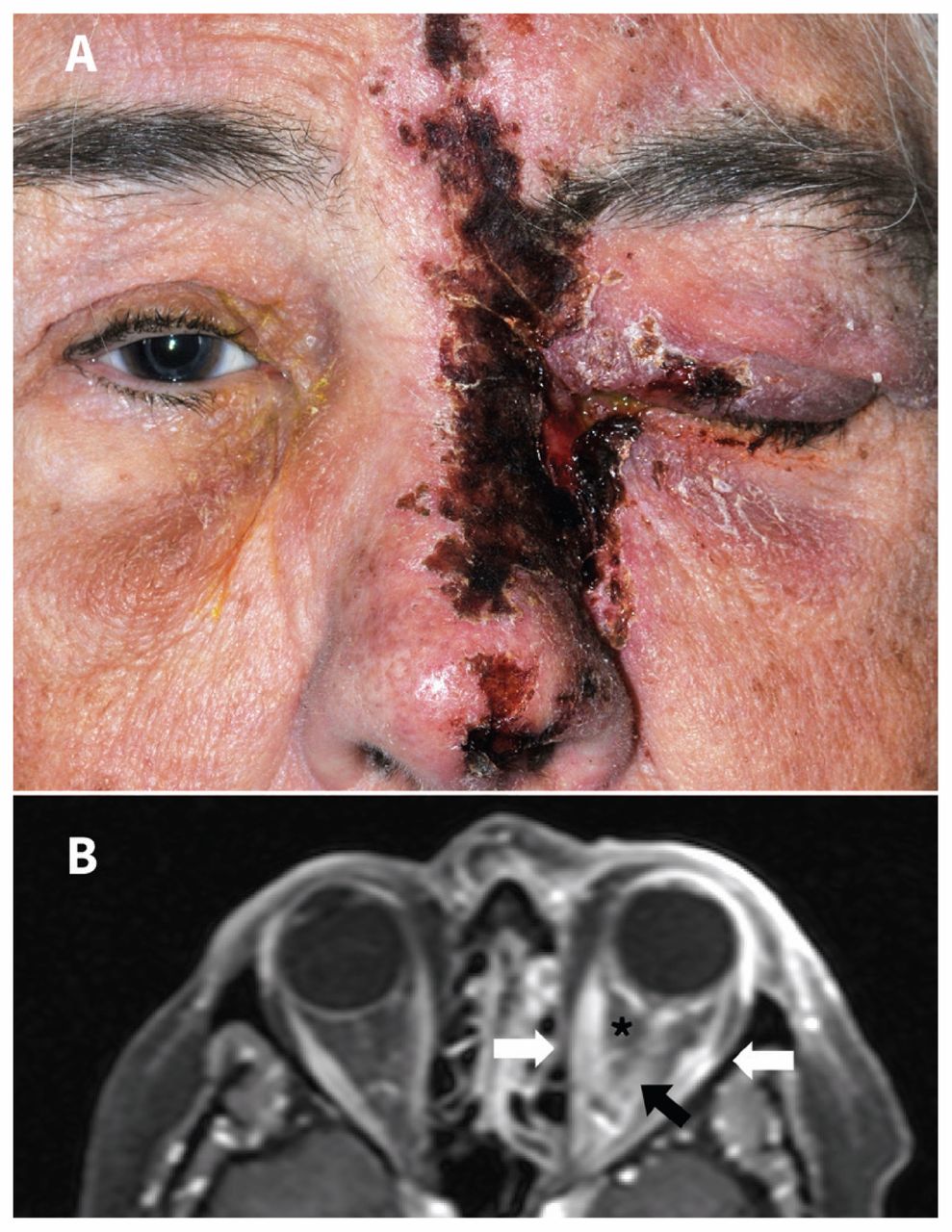
(A) Positive Hutchinson sign shown by a healing vesicular rash in the V1 dermatome on the left side of the nose of a 68-year-old woman with herpes zoster ophthalmicus. (B) T1-weighted magnetic resonance image (axial view) with gadolinium (fat saturated) of the same patient showing enhancement of the optic nerve (black arrow), extraocular muscles (white arrows) and fat stranding (*) within the orbital soft tissue, consistent with optic neuritis, myositis and orbital inflammation.
Ocular complications can threaten vision and require assessment by an ophthalmologist
Patients with decreased visual acuity, a red or painful eye, neurologic involvement (e.g., an afferent pupillary defect or ophthalmoplegia) or those who are immunocompromised should be referred urgently to an ophthalmologist.1 Ocular sequelae include infectious or inflammatory keratitis or uveitis, necrotizing retinopathy or orbital inflammation (Figure 1B).
Antiviral therapy can be started by primary care physicians
Starting antiviral agents within 72 hours of onset of the rash minimizes complications in herpes zoster ophthalmicus; however, given the risk of vision-threatening and other complications, antiviral agents may be started beyond this window.1 Valacyclovir (1 g taken orally three times a day for seven days) or famciclovir (500 mg taken orally three times a day for seven days) are as effective as acyclovir (800 mg taken orally five times per day for seven days), with more convenient dosing and lower costs.3
Systemic sequelae require multidisciplinary management
Uncommon complications of herpes zoster ophthalmicus include encephalitis and cerebral vasculitis, which require neurologic consultation and intravenous antiviral therapy.1 Postherpetic neuralgia after ophthalmic involvement is more common and difficult to treat, often requiring prolonged treatment.1,4
Vaccination reduces but does not eliminate the risk of herpes zoster
The adjuvanted herpes zoster subunit vaccine is more effective (97% v. 51%) than the live attenuated herpes zoster vaccine in preventing herpes zoster.5
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Jump to section
- Article
- A painful vesicular rash limited to the V1 dermatome of the trigeminal nerve should be considered herpes zoster ophthalmicus until proven otherwise
- Ocular complications can threaten vision and require assessment by an ophthalmologist
- Antiviral therapy can be started by primary care physicians
- Systemic sequelae require multidisciplinary management
- Vaccination reduces but does not eliminate the risk of herpes zoster
- Footnotes
- References
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

