


Risk of intraocular foreign body is associated with mechanism of injury
Accurate history-taking that involves attention to the mechanism of ocular injury should be obtained. High-risk mechanisms for intraocular foreign bodies include grinding, hammering, metal shaving, machine yard work and exposure to explosives.1
Ophthalmic examination should include dilation of the pupil
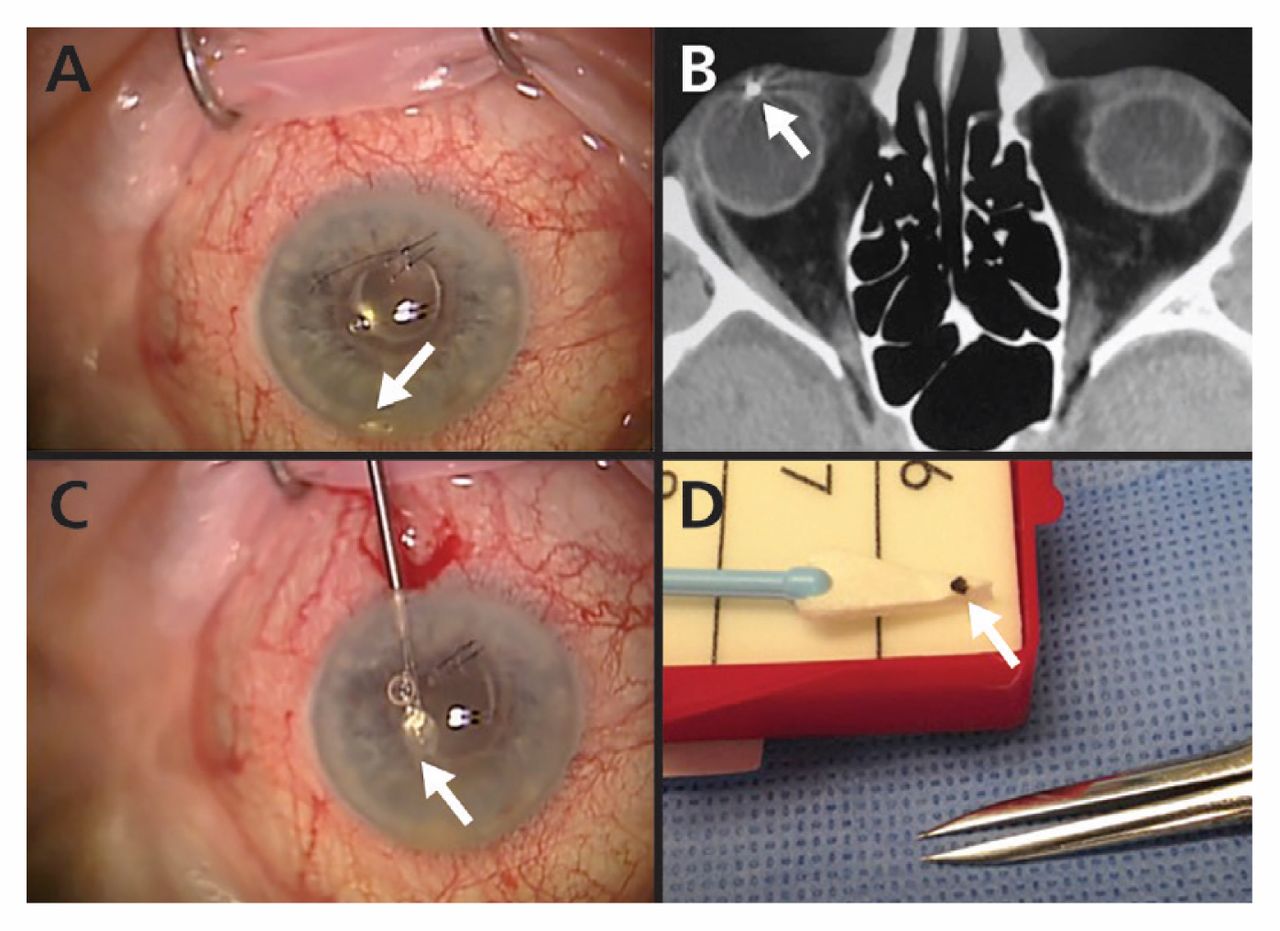
In 21%–38% of cases, intraocular foreign bodies are located in the anterior segment, allowing identification with slit-lamp examination alone.1 (Figure 1A) However, most intraocular foreign bodies are located in the posterior segment and require a dilated-pupil examination.1

Intraocular metallic foreign body embedded in the anterior chamber of the right eye. (A) Metallic foreign body in the anterior chamber (arrow). (B) Axial computed tomography scan of the orbits showing a well-defined, hyperdense foreign body producing streak artifacts in the anterior chamber (arrow). (C) Surgical removal of the foreign body (arrow). (D) The foreign body removed from the eye (arrow).
Imaging should be conducted promptly to diagnose and localize intraocular foreign bodies
Immediate computed tomography (CT) of the orbits without contrast is the modality of choice in suspected cases (Figure 1B).1 Both 1- and 3-mm cuts on CT have 100% sensitivity for detecting metallic, glass and stone intraocular foreign bodies of 0.5 mm in diameter.2 Plain-film radiography is inferior to CT, because it may miss nonmetallic intraocular foreign bodies up to 60% of the time.1
Antibiotics should be prescribed early to prevent endophthalmitis
Endophthalmitis is a complication in 3%–30% of cases involving intraocular foreign bodies.1 Therefore, patients with this injury should be given immediate treatment with prophylactic antibiotics. Systemic administration (intravenously or orally) of fluoroquinolones are good options because of their superior intraocular penetration.3
Patients with an intraocular foreign body require urgent referral to an ophthalmologist
The injured eye(s) should be protected with a rigid eye shield, and the patient should not receive anything by mouth during urgent transport to an ophthalmologist. Primary surgery to close the entry site(s) should be performed by an ophthalmologist within 12 hours after injury to reduce the risk of endophthalmitis and to prevent intraocular content extrusion.4 The foreign body must be removed; however, there is disagreement about the time frame for removal.5
Acknowledgement
The authors thank John B. Davies for providing the figures.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Jump to section
- Article
- Risk of intraocular foreign body is associated with mechanism of injury
- Ophthalmic examination should include dilation of the pupil
- Imaging should be conducted promptly to diagnose and localize intraocular foreign bodies
- Antibiotics should be prescribed early to prevent endophthalmitis
- Patients with an intraocular foreign body require urgent referral to an ophthalmologist
- Acknowledgement
- Footnotes
- References
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

