


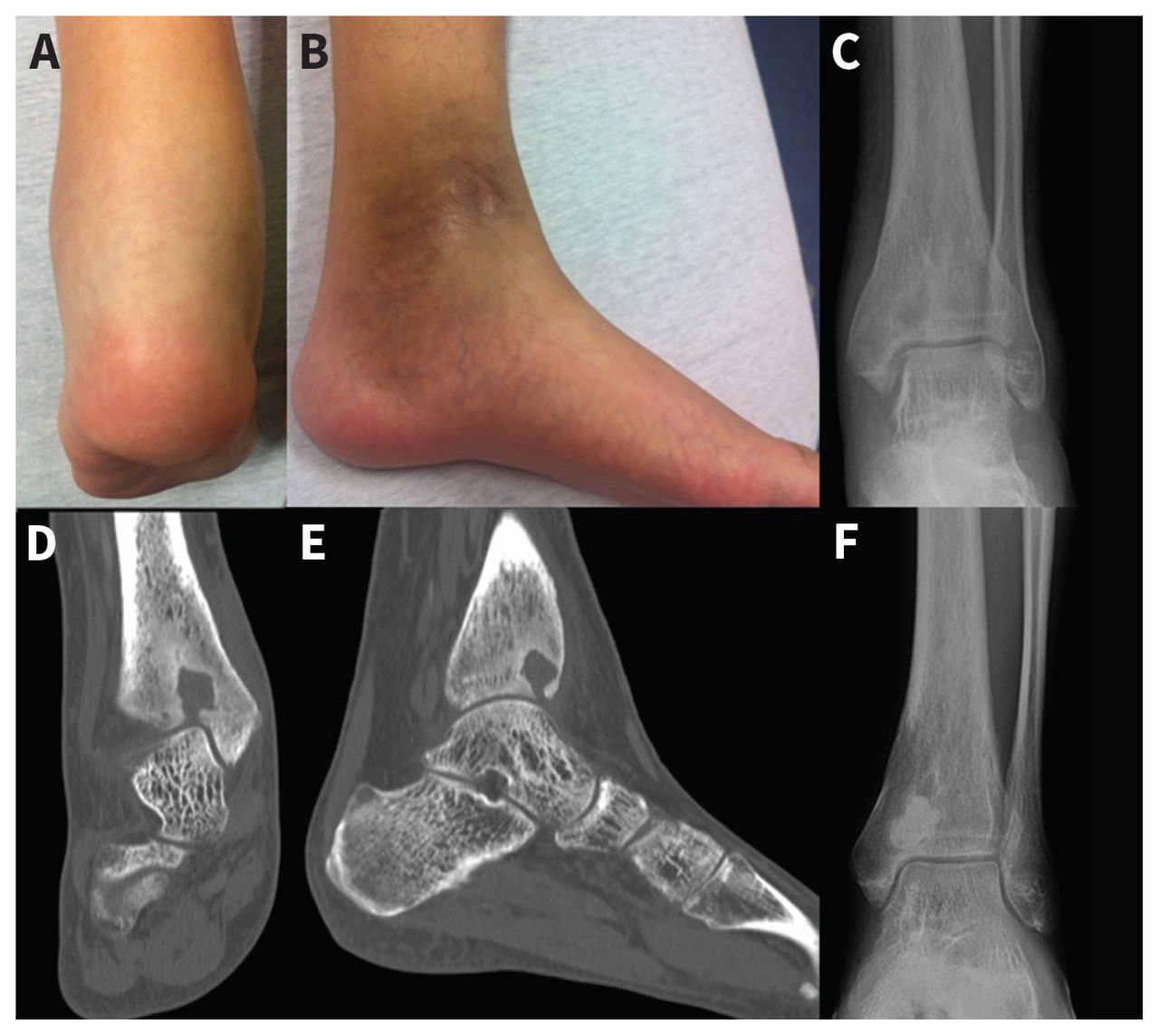
A 27-year-old man who had immigrated from China presented to the emergency department with chronic (duration 9 mo) pain and swelling in his left ankle. His medical history was notable for a prolonged stay in hospital in childhood because of an infection in his left lower extremity. He stated that he did not use intravenous drugs. Upon examination, the patient was afebrile, his left calf was atrophied, and he had swelling posterior to both malleoli (Figure 1A). He also had hyperpigmentation of the skin around the medial malleolus (Figure 1B) and limited active and passive range of movement of his left ankle.

Swelling and hyperpigmentation over the left malleoli of a 27-year-old man with Brodie abscess (A, B). Radiographs showing a radiolucent lesion in the epiphysis before (C) and after (F) placement of cement–antiobiotic bone filler. Computed tomography scans showing the lesion in the distal tibia with a tract communicating with the tibiotalar joint (D, E).
The patient’s leukocyte count was 7.9 × 109/L, with an erythrocyte sedimentation rate of 10 mm/h. He had a negative test result for HIV infection. Radiography of his left distal tibia showed a solitary, punched-out radiolucent lesion in the epiphysis (Figure 1C). A computed tomography scan showed an irregular, lobular-shaped lucent lesion in the left distal tibia, with a tract communicating with the tibiotalar joint (Figures 1D, 1E). He was diagnosed with Brodie abscess.
The patient underwent arthrotomy of the left ankle, with irrigation, débridement and placement of a cement–antibiotic bone filler (Figure 1F). He received six weeks of culture-directed antibiotics. Methicillin-sensitive Staphylococcus aureus was isolated from bone specimens. Mycobacterial and fungal cultures were negative. Six months posttreatment, the patient had recovered range of motion in his ankle.
Brodie abscess is a subacute form of hematogenous osteomyelitis that accounts for 2.5%–42% of primary bone infections.1 In general, patients are younger than 25 years of age and present with joint pain and localized swelling. Signs and symptoms of systemic disease are frequently absent.2,3 Staphylococcus aureus (30%–60%), Pseudomonas (5%), Klebsiella (5%) and coagulase-negative Staphylococcus (5%) are causative organisms.2 However, 20% of cultures are negative for these organisms.2,3 Radiographically, an intramedullary area of central lucency with sclerotic margins is characteristic.4
Differential diagnosis of Brodie abscess includes benign and malignant bone lesions such as cysts, osteoid osteoma, giant cell tumour, chondroblastoma and Ewing sarcoma.4 In addition to systemic antibiotics, surgical débridement is usually required, with bone grafting if a large cavity requires stabilization.2,3,5
Acknowledgement
The authors thank Cedric Yansouni for his help.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

