


A 46-year-old man with a history of T2N2 right tonsillar squamous cell carcinoma was referred to the emergency department after a large aspiration event during a barium esophogram. His cancer had been treated five years previously with panitumumab, radiation and salvage surgery for residual tumour. The esophogram was arranged for a six-month history of dysphagia and periprandial coughing up of food contents. The patient was asymptomatic upon arrival in the emergency department.
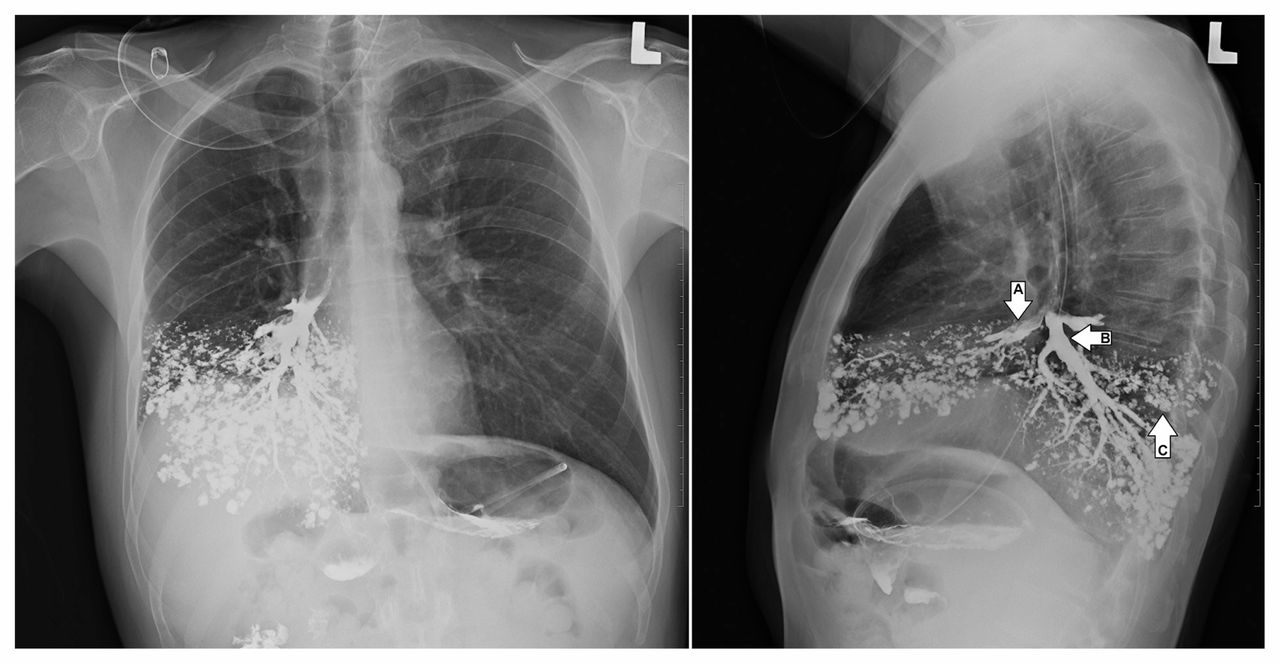
Upon examination, he appeared well and hemodynamically stable, with a respiratory rate of 20 breaths per minute, oxygen saturation of 94% on ambient air and a temperature of 38.1°C. Respiratory examination showed no increased work of breathing, with crackles in the right lung base on auscultation. Neurologic deficits included palsy of the right hypoglossal nerve and asymmetry of the soft palate. Chest radiographs conducted in the emergency department showed accumulation of barium in the right middle and lower lobes (Figure 1). Bronchoscopy confirmed localization of barium in the right lung, with no evidence of tracheoesophageal fistula. Nasopharyngoscopy showed normal vocal cord function, but absent supraglottic and glottic sensation. A videofluoroscopic swallowing examination identified uncoordinated swallowing with florid aspiration, and a diagnosis of aspiration pneumonitis was made. These findings were attributed to delayed effects from radiation treatment. He remained clinically stable and a feeding gastrostomy tube was inserted.

Radiographs of the posteroanterior (left image) and lateral (right image) chest showing barium bronchograms of the right middle (arrow A) and right lower (arrow B) lobe bronchi. Extensive tree-in-bud opacifications in the right middle and lower lobes are indicative of bronchiolar filling (arrow C).
Risk factors for aspiration include altered level of consciousness, neurologic dysfunction of the upper airway, structural esophageal disease, cancers of the aerodigestive tract and iatrogenic disruption of the airway (i.e., intubation and endoscopy).1 The anatomic configuration of the bronchial tree predisposes contents to enter the right and middle lobes on erect aspiration, as shown in our case.
Aspiration pneumonitis is an inflammatory injury to the lung triggered by exposure to noxious stimuli, typically of gastric origin. Clinical manifestations range from none to cough, wheeze, dyspnea, respiratory failure and, in severe cases, acute respiratory distress syndrome.1 Treatment is typically supportive, and routine antibiotic use is not indicated.1
Barium is chemically inert and had been used as a contrast medium for bronchography before the advent of computed tomography and bronchoscopy.2 Although historically found to be safe in this context, aspiration of barium may also produce a chemical pneumonitis in some cases.3
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
Disclaimer: Matthew Stanbrook is a deputy editor for CMAJ and was not involved in the editorial decision-making process for this article.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

