


Nipple discharge is common and can be physiologic
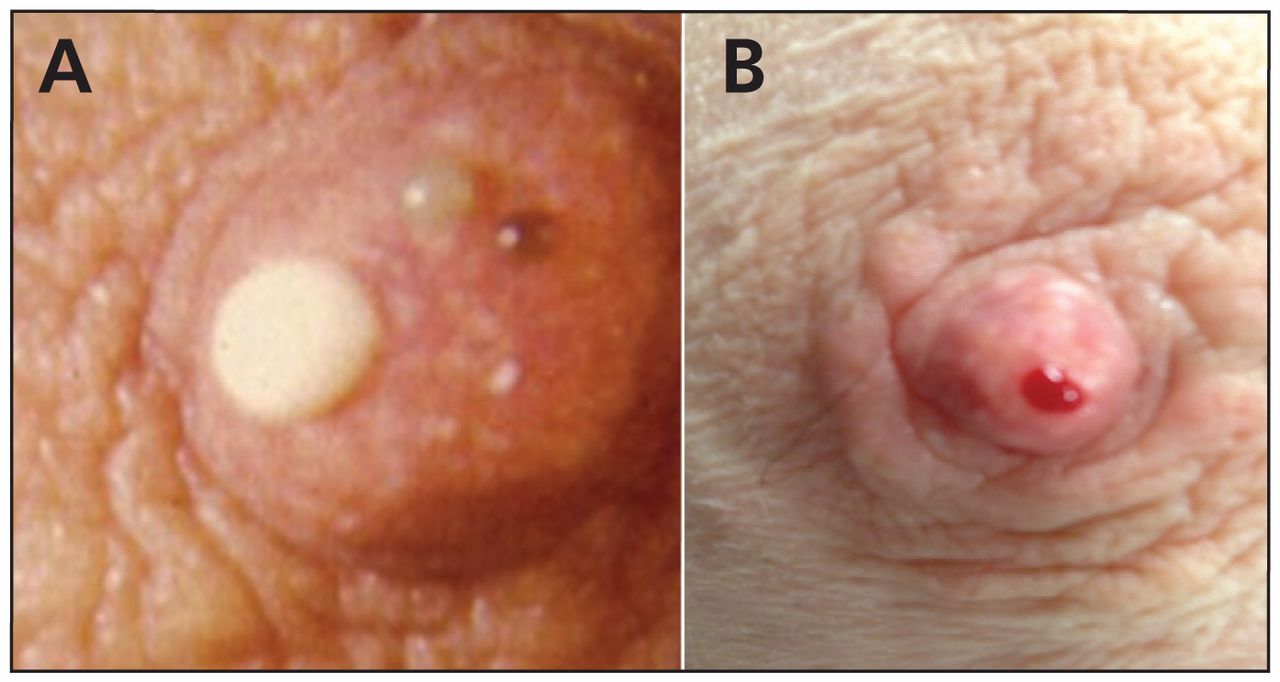
Nipple discharge is benign in most instances and is the third most common breast-related complaint, after breast pain and breast mass.1 About 50% of women in their reproductive years have physiologic nipple discharge that is characterized by bilateral, milky, green or yellow fluid expressed from multiple nipple duct openings and often associated with nipple stimulation (Figure 1).2
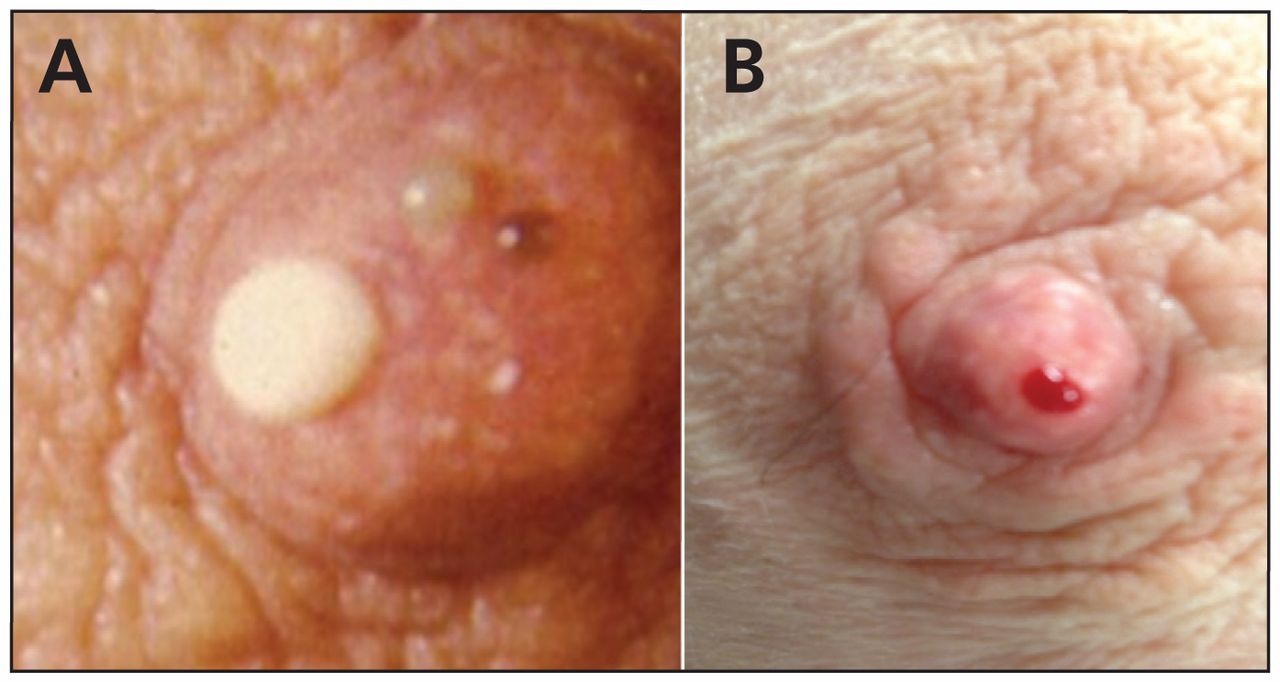
Nipple discharge from (A) multiple ducts (physiologic) and (B) a single duct (pathologic).
History and physical examination can distinguish physiologic from pathologic nipple discharge
Pathologic nipple discharge is spontaneous and often unilateral. It may arise from a single duct or be associated with a mass or new skin changes. It can be bloody, serous, green or black.1–3 Benign intraductal papilloma (48%), ductal ectasia (15%–20%) and carcinoma (10%–15%) are the most common causes.1
Patients with pathologic nipple discharge should be referred for imaging to exclude carcinoma
Mammography (sensitivity may be decreased in younger patients) and retroareolar ultrasonography should be performed in all cases of pathologic nipple discharge.4,5 Galactography, and more recently magnetic resonance imaging, can be helpful in identifying an involved duct or papilloma.2,4 Patients with a palpable mass or a mass identified on imaging should undergo needle biopsy to exclude carcinoma.3,5
All cases of pathologic nipple discharge need tissue diagnosis
Physiologic nipple discharge tends to resolve spontaneously. Patients with pathologic discharge should have histologic evaluation through surgical excision of the involved duct (if no lesion is identified), or targeted excision of the lesion (if papilloma is identified) via open or needle biopsy.4,5
Milky discharge in patients who are not pregnant or lactating (galactorrhea) is often due to medications
Bilateral milky nipple discharge is appropriate during pregnancy and lactation, and it can last up to one year after delivery or after breastfeeding has stopped. Prolactin levels must be assessed to exclude endocrinopathy (> 20 ng/mL) in patients who are not pregnant or lactating.2 Medications such as psychotropics, antihypertensives (e.g., reserpine, methyldopa, verapamil), opiates, prokinetics (e.g., metoclopramide) and H2-blockers (e.g., cimetidine) can cause galactorrhea.1,2
CMAJ invites submissions to “Five things to know about …” Submit manuscripts online at http://mc.manuscriptcentral.com/cmaj
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Jump to section
- Article
- Nipple discharge is common and can be physiologic
- History and physical examination can distinguish physiologic from pathologic nipple discharge
- Patients with pathologic nipple discharge should be referred for imaging to exclude carcinoma
- All cases of pathologic nipple discharge need tissue diagnosis
- Milky discharge in patients who are not pregnant or lactating (galactorrhea) is often due to medications
- Footnotes
- References
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

