


A 75-year-old man presented with a 50-year history of a thick, red, scaly plaque covering more than 50% of the bottom of his right foot (Figure 1). The patient reported that the eruption had grown steadily over the years, with no response to a variety of creams prescribed to treat psoriasis, none of which were a potent steroid. The patient described no other lesions, no joint pain and no family history of psoriasis.
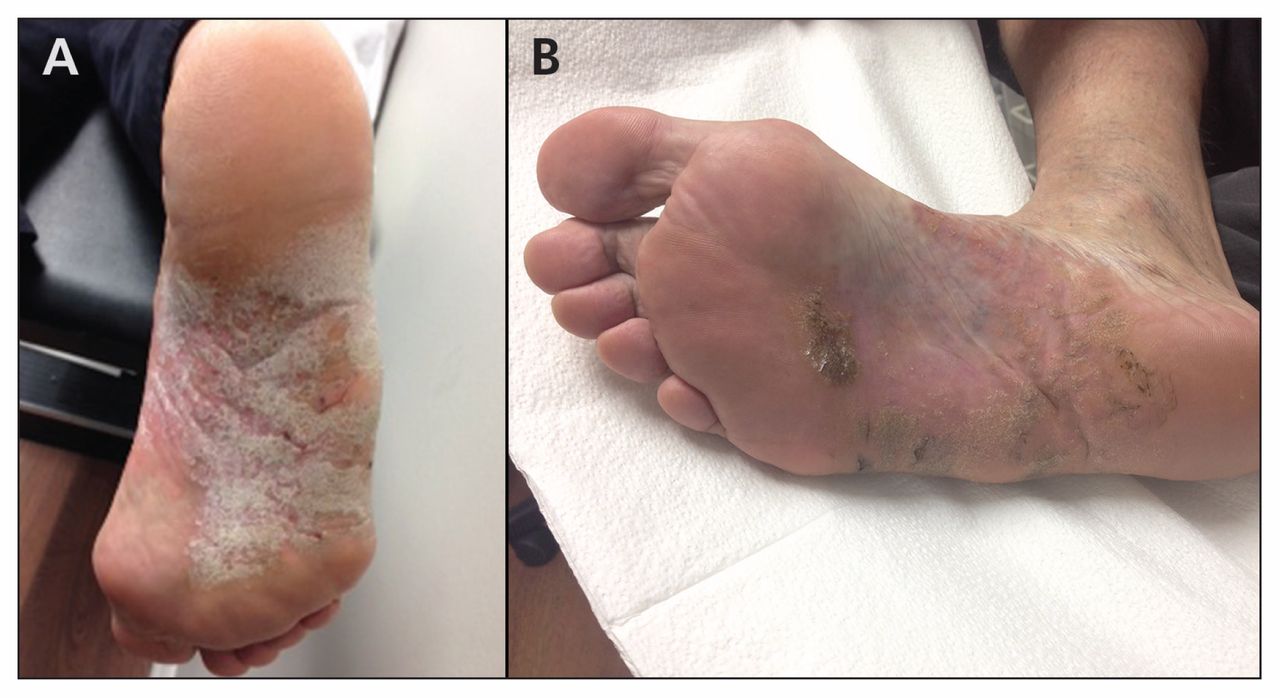
A 75-year-old man presented with a 50-year history of a thick, erythematous, scaly plaque covering more than 50% of the plantar aspect of his right foot. (A) Initial presentation, at which Woringer–Kolopp disease was diagnosed. (B) Follow-up after three months’ treatment with topical clobetasol showed greater than 80% improvement in the patient’s condition.
A biopsy of the lesion showed epidermal acanthosis and prominent lymphocytosis with atypia (Appendix 1, available www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.141318/-/DC1). A full skin examination showed no other lesions suggestive of lymphomatoid papulosis or mycosis fungoides. No lymphadenopathy was found on physical examination, and computed tomography showed no evidence of adenopathy. Based on these clinical, immunohistologic and radiologic findings, we diagnosed Woringer–Kolopp disease.
The patient was given clobetasol proprionate ointment (0.05%) to be used twice daily. He responded well to treatment, with greater than 80% improvement in his condition after three months (Figure 1). Other treatment options, including radiation and phototherapy, were discussed; however, the patient preferred to continue using the topical steroid alone.
Woringer–Kolopp disease, also known as pagetoid reticulosis, is classified as an indolent cutaneous T cell lymphoma under the European Organisation for Research and Treatment of Cancer system.1 This uncommon condition was first described by Woringer and Kolopp in 1939 and is often misidentified as psoriasis, dermatitis, parapsoriasis or dermatophytosis.2
Effective treatment of Woringer–Kolopp disease includes topically applied corticosteroids, localized radiation therapy and phototherapy using either psoralen and ultraviolet A radiation or narrow-band ultraviolet B radiation.1 The prognosis of patients with limited patch-stage Woringer-Kolopp disease have a similar life expectancy to an age-, sex-, and race-matched control population.1
Owing to the rarity and indolent nature of Woringer–Kolopp disease, and its mimicry of more common scaly skin disorders, the condition is often misdiagnosed, and patients may receive inappropriate treatment for years.
Woringer–Kolopp disease should be suspected in patients with persistent or progressive plaques refractory to treatment.2,3 We recommend a biopsy in cases of unilateral involvement that lack other features of psoriasis, including no nail involvement, no arthritis and no family history of psoriasis.
Acknowledgements
The authors thank Dr. Roland Jong for his pathology expertise.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

