


Understanding the effect of resident duty hour reform
Concerns about resident fatigue affecting patient safety have prompted regulatory changes that limit resident duty hours in the United States and Canada, including Quebec. With a recent report from the National Steering Committee on Resident Duty Hours in Canada recommending restrictions on duty hours, it is likely that similar regulatory changes will apply to residency training programs across Canada.
In this qualitative study, the authors interviewed 18 participants, including program directors, division directors and department chiefs, in one Canadian medical school. The key theme articulated by the participants was that changes in resident duty hours could lead to gaps in providing clinical care and that programs that are mostly inpatient-based will be affected to a greater extent (Box).
Potential strategies to address the gaps include resident-based solutions, faculty-based solutions and solutions based on other providers. However, each of these strategies has its advantages and disadvantages in terms of its effect on the other four areas identified as being affected by changes to duty hours (i.e., education, preparedness for practice, continuity of care and provider well-being). CMAJ Open 2014;2:E115–E120
Perceived effects of changes to resident duty hours
“Restructuring of the entire call schedule … would force a reexamination of how residents are allocated and how services are covered at night.” Med-Peds faculty — Respondent 2
“It’s rare that [residents] would work a 16-hour day in [our specialty]. … As I say, this hasn’t really been a topic of conversation in [our specialty] very much.” Other faculty — Respondent 11
“It’s obvious to me that it’s not one size fits all. … I think that it’s a complete fallacy to think that the training needs and requirements of a family doctor are the same as for a neurosurgeon.” Surgical faculty — Respondent 7
Trends in hospital admission for patients on dialysis
After cardiovascular disease, infection is the second leading reason for admission to hospital among patients receiving long-term dialysis. Because infection-related hospital admissions are potentially preventable, it is important to assess their frequency and associated risk factors to inform prevention strategies aimed at improving patient care.
In this retrospective cohort study, the authors looked at the incidence of infection-related hospital admissions for all new and long-term patients (n = 9822) receiving dialysis from 2001 to 2007 in Quebec. The rate of admission to hospital for infection during the study period remained stable among patients on long-term dialysis, independent of age, sex and length of time on dialysis. However, decreases in admission rates for all causes by 22.9% and those related to cardiovascular complications by 46.7% during the same period meant that the proportion of admissions related to infection increased from 13.1% to 16.1% (Figure 1).
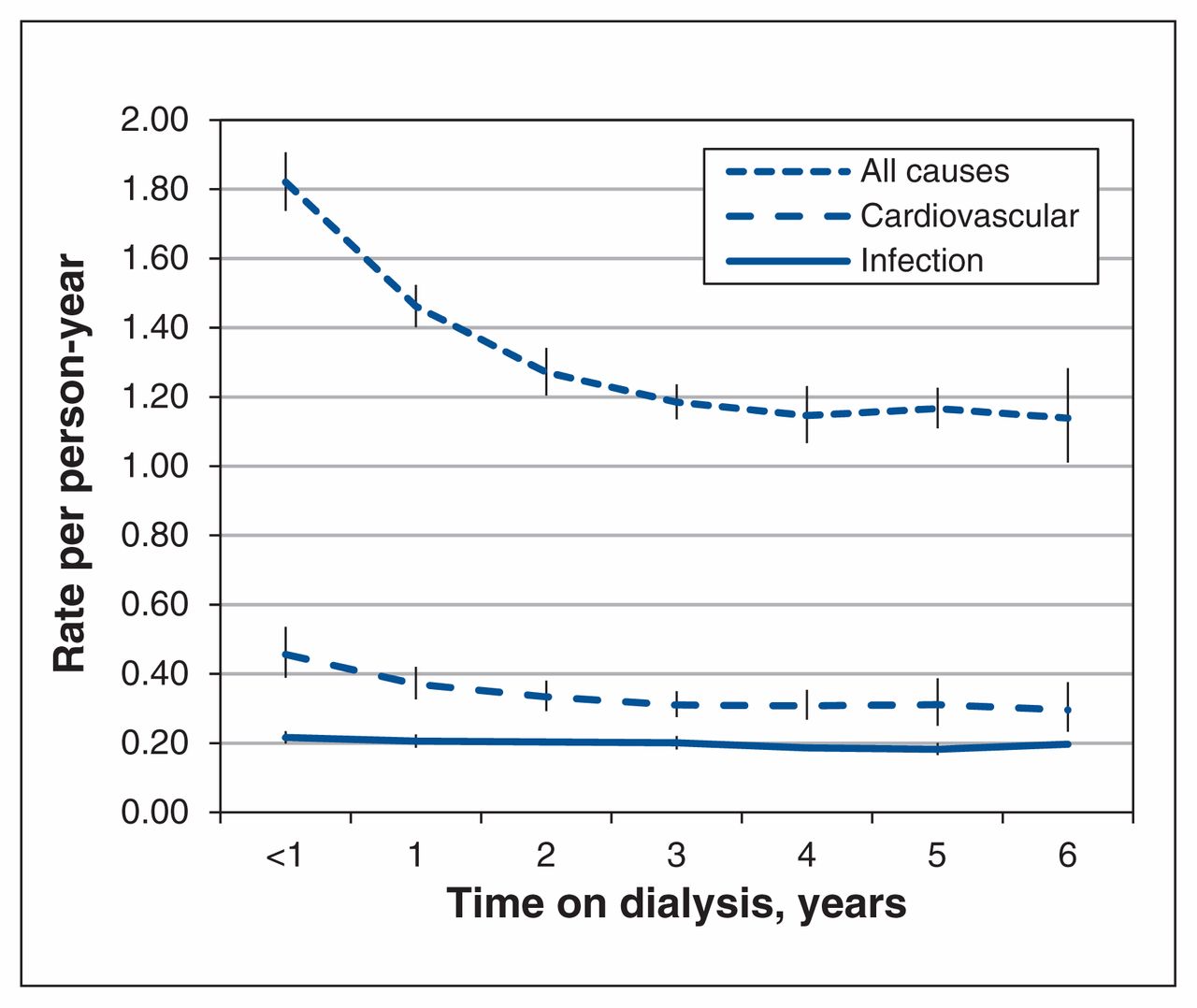
Unadjusted rates of admission to hospital among patients on dialysis, by length of time on dialysis. Error bars = 95% confidence intervals.
The decreasing trend in all-cause admissions may be explained by increased use of outpatient settings for interventions, and the similar trend in hospital admission related to cardiovascular causes may be a result of more aggressive treatment of cardiovascular risk factors, say the authors. Infections may be hard to prevent; however, some associated risk factors are modifiable, and intervention strategies may help reduce infection rates. CMAJ Open 2014;2:E109–E114
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

