


Article Figures & Tables
Figures
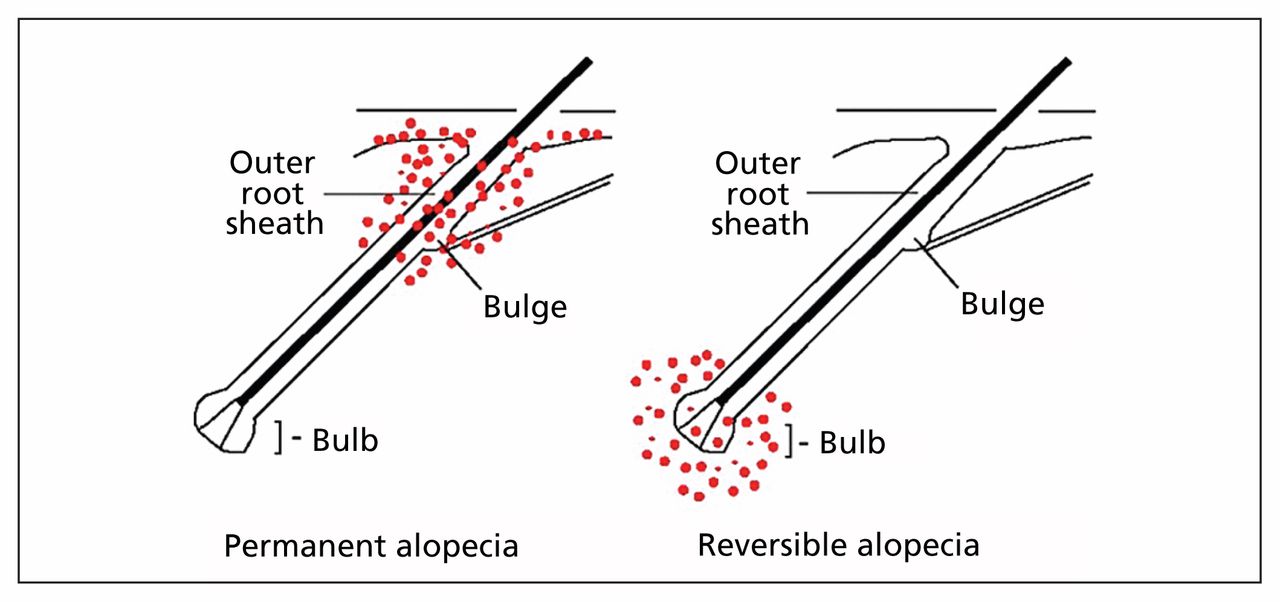
- Figure 1:
Illustration of the hair follicle. Reversible alopecia (right) is characterized by damage to the hair bulb from inflammation. The hair bulge remains healthy and the hair follicle is able to regenerate with effective treatment. Cicatricial alopecia (left) is characterized by inflammation that causes irreversible damage to the hair bulge of the outer root sheath.
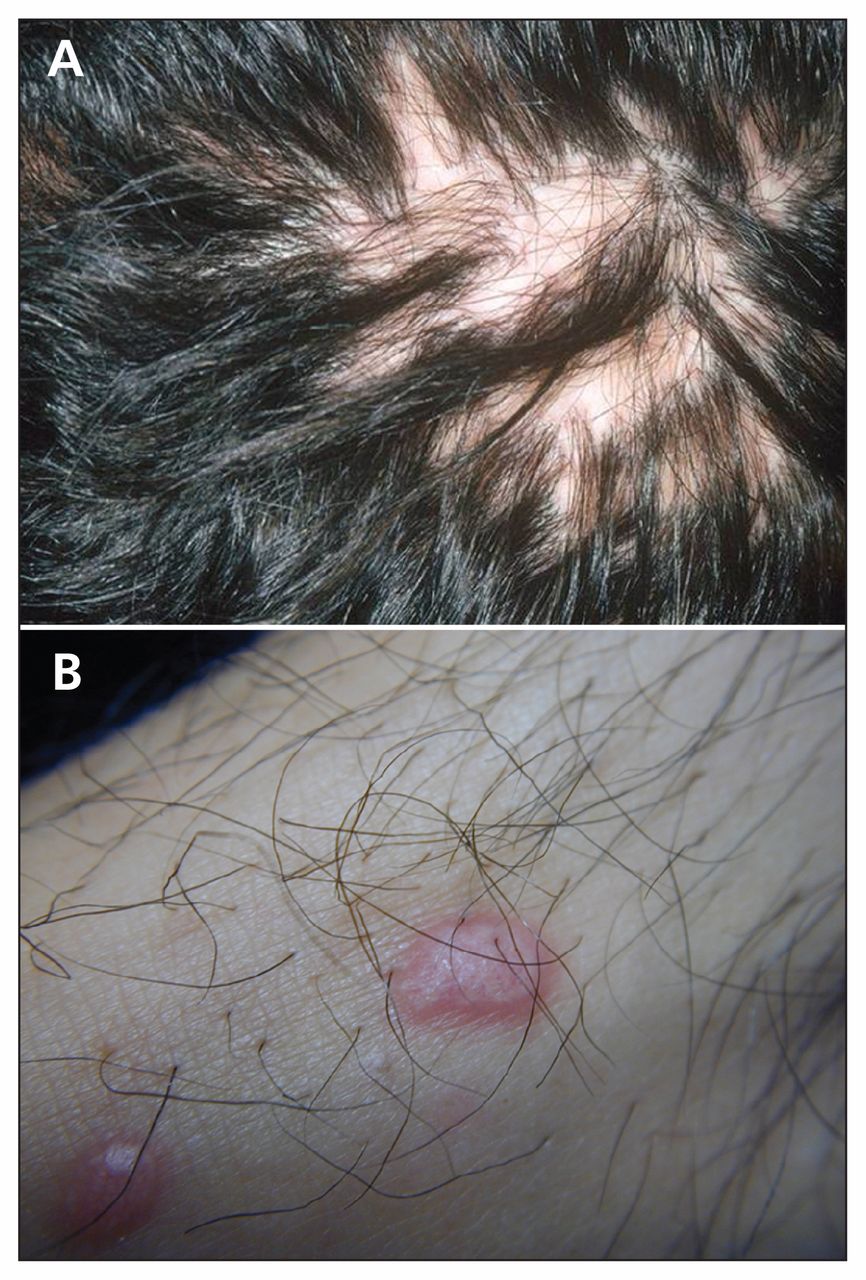
- Figure 2:
(A) Photograph of a patient’s scalp showing lichen planopilaris. Lichen planopilaris is characterized by multifocal or central patches with follicular hyperkeratosis and perifollicular erythema on the scalp. (B) Photograph of a patient’s neck showing skin changes with hair growing out of the affected area.
- Figure 3:
Photograph of a patient’s scalp showing folliculitis decalvans. Folliculitis decalvans is characterized by pustules and honey-coloured crusting at the periphery of a patch of hair loss. Patches typically present on the vertex or midfrontal scalp.


Tables
- Table 1:
Common classifications and treatment options for primary cicatricial alopecia (5), (6), (9), (11)– (25)
Type and subtype Epidemiology Clinical features Treatment Prognosis First line Second line Third line Lymphocytic Lichen planopilaris < 10% scalp involvement (localized)
Generalized
Rapidly progressing
Women Itchy, multifocal or central patches with follicular hyperkeratosis and perifollicular erythema; nonscalp areas may be affected Intralesional triamcinolone +/− topical steroids Potent topical steroids Calcineurin inhibitors If not treated, will burn out Intralesional triamcinolone +/− topical steroids Hydroxychloroquine Doxycycline, mycophenolate or cyclosporine Oral corticosteroids Oral corticosteroids Oral corticosteroids Chronic cutaneous lupus erythematosus Women, genetic, ultraviolet sensitive Single or multifocal patches with pronounced activity in the centre of the patch, ulceration, follicular plugging, atrophy and depigmentation Intralesional triamcinolone Hydroxychloroquine +/− mepacrine (quinacrine) Retinoids (e.g., isotretinoin), azathioprine, methotrexate, mycophenolate mofetil or thalidomide Systemic lupus erythematosus will develop in less than 5% of patients (higher risk in children and adolescents: 25%–30%); spontaneous remission occurs in one-third of patients Frontal fibrosing alopecia Postmenopausal women Band-like distribution around the frontal hairline; may be present in eyebrows Hydroxychloroquine Mycophenolate Antiandrogens or calcineurin inhibitors If not treated, will burn out Central centrifugal cicatricial alopecia Black women Resembles lichen planopilaris; burning, scaling and itchiness may occur Cease traumatic hair care Topical steroids Topical steroids If not treated, will burn out Brocq pseudopelade Adults Small and/or large, irregular patches of hair loss on the scalp with no detectable symptoms or inflammation; end-stage burnout Intralesional triamcinolone +/− topical steroids Hydroxychloroquine, isotretinoin or prednisone Hydroxychloroquine, isotretinoin or prednisone End-stage burnout Neutrophilic Folliculitis decalvans Adults; can occur in adolescent males but not seen in women until > age 30 yr Single patch of complete alopecia that expands circumferentially, slowly over years; typically found on hair-bearing periphery of scalp; pustules, honey- coloured crusting, tufting; nonscalp involvement is rare Rifampicin +/− clindamycin Doxycycline, ciprofloxacin or clarithromycin Fusidic acid + zinc If not treated, will burn out Dissecting cellulitis of the scalp Black adolescent and adult males Multiple fluctuant nodules found across the scalp, often interconnected by sinus tracts; may be associated with acne conglobata: discharge is common and should be cultured Oral isotretinoin Intralesional triamcinolone Oral corticosteroids If not treated, will burn out
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

