


Abstract
Background: Systems of stroke care delivery have been promoted as a means of improving the quality of stroke care, but little is known about their effectiveness. We assessed the effect of the Ontario Stroke System, a province-wide strategy of regionalized stroke care delivery, on stroke care and outcomes in Ontario, Canada.
Methods: We used population-based provincial administrative databases to identify all emergency department visits and hospital admissions for acute stroke and transient ischemic attack from Jan. 1, 2001, to Dec. 31, 2010. Using piecewise regression analyses, we assessed the effect of the full implementation of the Ontario Stroke System in 2005 on the proportion of patients who received care at stroke centres, and on rates of discharge to long-term care facilities and 30-day mortality after stroke.
Results: We included 243 287 visits by patients with acute stroke or transient ischemic attack. The full implementation of the Ontario Stroke System in 2005 was associated with an increase in rates of care at stroke centres (before implementation: 40.0%; after implementation: 46.5%), decreased rates of discharge to long-term care facilities (before implementation: 16.9%; after implementation: 14.8%) and decreased 30-day mortality for hemorrhagic (before implementation: 38.3%; after implementation: 34.4%) and ischemic stroke (before implementation: 16.3%; after implementation: 15.7%). The system’s implementation was also associated with marked increases in the proportion of patients who received neuroimaging, thrombolytic therapy, care in a stroke unit and antithrombotic therapy.
Interpretation: The implementation of an organized system of stroke care delivery was associated with improved processes of care and outcomes after stroke.
Stroke is a leading cause of death and disability worldwide.1,2 Guidelines recommend that eligible patients receive care in a stroke unit, undergo neuroimaging and receive thrombolytic therapy, antithrombotic agents and screening for carotid stenosis.3–6 Many of these interventions require specialized resources, including clinicians with expertise in stroke care and rapid access to brain and vascular imaging; however, wide interfacility variations exist in the availability of such resources.7–10
To address regional disparities in resources and care, organizations such as the Canadian Stroke Network and the American Stroke Association have recommended the implementation of organized systems of stroke care delivery.11,12 Such systems are designed to facilitate access to optimal stroke care across an entire region and to promote the use of evidence-based therapies.11 However, little is known about the effect of stroke systems of care on outcomes in patients with stroke.
The province of Ontario was the first large jurisdiction in Canada, and in North America, to implement an integrated regional system of stroke care delivery. A system of coordinated stroke care, known as the Ontario Stroke System, was launched in 2000 and fully implemented in 2005, resulting in a major transformation in the delivery of stroke care across the province.13 We used population-based administrative and clinical data to evaluate the effect of the system’s implementation on stroke care and outcomes.
Methods
Setting
We conducted a population-based retrospective analysis of patients discharged from hospital following either an emergency department visit or admission for acute stroke or transient ischemic attack between Jan. 1, 2001, and Dec. 31, 2010. Ontario is Canada’s most populous province, with a population of more than 12.1 million at the midpoint of the study period.14 The province has more than 140 acute care institutions, with 40% of all hospitals located in rural areas.15 Residents have universal access to hospital care and physicians’ services.
This study was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre.
Data sources and study sample
We used 2 main data sources for this study. For analyses of rates of care at stroke centres, stroke case–fatality rates, and rates of admission to a long-term or chronic care facility after stroke, we used the Canadian Institute for Health Information’s Discharge Abstract Database and National Ambulatory Care Reporting System database. These databases contain diagnostic and procedural information for all hospital admissions and emergency department visits in Ontario and have been extensively validated.16,17 We identified visits for stroke or transient ischemic attack using the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10), codes I60, I61, I63, I64, H34.1 and G45; these codes are endorsed by the Canadian Stroke Strategy and have been validated in Canadian populations.18–20 We included patients aged 18–102 years and excluded those with an invalid health card number. Carotid endarterectomy and stenting were identified using procedure codes 1JE57 and 1JE50. Comorbid conditions were summarized using the Charlson–Deyo comorbidity index scale21 and were only available for patients admitted to hospital. Date of death was identified using the Registered Persons Database.
Because the administrative databases do not contain variables such as thrombolytic therapy and care in a stroke unit, we used the Ontario Stroke Audit database maintained by the Ontario Stroke Registry (formerly the Registry of the Canadian Stroke Network) to create a second cohort of patients with stroke, which we used for analyses of processes of care. Since 2002, the registry has conducted periodic audits on a random sample of all patients with stroke or transient ischemic attack seen at all institutions across Ontario, with patients identified using the ICD-10 codes listed above, and with detailed information collected on acute stroke management and outcomes.15 Validation by duplicate chart abstraction has shown excellent agreement for key variables including age, type of stroke, thrombolytic therapy and care in a stroke unit.15 Under provincial privacy legislation, the Ontario Stroke Registry is able to perform chart abstraction without individual patient consent. For the present study, we included all patients identified in 3 registry audits performed between Apr. 1, 2002, and Mar. 31, 2009.
Intervention
The intervention of interest was the province-wide implementation of the Ontario Stroke System (Table 1;15,20,22,23 Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.121418/-/DC1). This system was initiated and funded by the Ontario Ministry of Health and Long-Term Care in 2000, with a phased implementation that was finalized in 2005 (www.ontariostrokenetwork.ca). Under the Ontario Stroke System, the province is divided into 11 regions, each of which has a regional stroke centre (a large institution with advanced resources for delivery of stroke care comparable to the comprehensive stroke centres established in the United States24) and a program director responsible for coordinating delivery of stroke care within the region. Each region may also have a number of district (or primary) stroke centres capable of providing more basic treatment to patients with stroke. Regional transfer agreements and ambulance bypass protocols permit patients with suspected stroke to be preferentially transported to designated stroke centres. Other components of the Ontario Stroke System include secondary stroke prevention clinics, provider education and institutional audit and feedback (Table 1). Administration of thrombolytic therapy at smaller hospitals is facilitated through the Ontario Telestroke Program.22
Components of the Ontario Stroke System
Although the Ontario Stroke System was launched in 2000, we selected 2005 as the cut-point for evaluating its effect because this corresponded to the year the system was fully implemented, with finalization of regional networks, transfer agreements, infrastructure funding and transfer of responsibility for the program from the Ministry of Health and Long-Term Care to the regions.
Outcomes
The primary outcome was the proportion of patients with stroke or transient ischemic attack who received care at a regional or district stroke centre. Secondary outcomes were length of stay for patients admitted to hospital; discharge to a long-term care or chronic care facility after hospital admission for stroke; all-cause mortality at 30 days after stroke, stratified by type of stroke (ischemic or hemorrhagic); waiting times for carotid revascularization; thrombolytic therapy in patients with ischemic stroke and arrival to hospital within 2.5 hours after symptom onset; neuroimaging (computed tomography [CT] or magnetic resonance imaging [MRI] of the brain); carotid imaging (carotid Doppler ultrasonography, CT angiography, MR angiography or catheter angiography) in patients with ischemic stroke or transient ischemic attack; care in a stroke unit; dysphagia screening; and prescription of antithrombotic therapy among patients with ischemic stroke or transient ischemic attack.
Statistical analysis
We used data from the administrative databases for hospital admissions to compare outcomes in the periods before and after full implementation of the stroke system in 2005; we used the χ2 test for categorical variables and the t test for continuous variables. We next used piecewise regression analyses to determine whether there was a change in rates of outcomes after 2005 beyond what would be expected from baseline temporal trends. We divided the 10-year study period into monthly intervals and calculated rates for each outcome within each interval. In the piecewise regression model, we tested 3 parameters: β1 (equal to time in monthly intervals) to measure the slope of the outcome before the intervention; β2 (equal to the change in the outcome measure between the last time point before the intervention and the first time point after the intervention) to test whether the intervention had an immediate effect on rates of the outcome (change in level); and β3 (equal to the difference in the slope of the period before the intervention and the slope of the period after the intervention) to determine whether the slope of the outcome changed after the intervention (change in slope). We plotted residuals over time and used the Durbin–Watson statistic to ensure that autocorrelation did not exist.
We standardized rates of hospital admissions and emergency department visits by age and sex, using the 2001 Ontario population as the standard population. We calculated mortality only for patients admitted to hospital, and rates were stratified by type of stroke and adjusted for age, sex and Charlson–Deyo comorbidity index score by use of logistic regression models and indirect standardization. We adjusted rates of discharge to long-term care facilities by age, sex, stroke type and Charlson–Deyo comorbidity index score. We calculated waiting times for carotid revascularization from the date of hospital admission for stroke to the date of surgery.
For rates of thrombolytic therapy, neuroimaging, carotid imaging, care in a stroke unit, dysphagia screening and use of antithrombotic therapy, we used the registry cohort and performed tests for trends over time using a survey logistic regression model. We did not perform piecewise regression analyses because of discontinuous data and insufficient data points. We performed secondary analyses with stratification by hospital type (stroke centre v. nonstroke centre).
Results
During the 10-year study period, there were 243 287 emergency department visits and 163 198 hospital admissions for acute stroke or transient ischemic attack. Overall, 49% of the study patients were men, and the median age was 75 years. Patient characteristics were similar in the periods before and after 2005 (Table 2).
Baseline characteristics of patients with stroke or transient ischemic attack, before (Jan. 1, 2001–Mar. 31, 2005) and after (Apr. 1, 2005–Dec. 31, 2010) full implementation of the Ontario Stroke System
The proportion of patients who received care at either a regional or district stroke centre increased from 40.0% before 2005 to 46.5% in the period after full implementation of the stroke care delivery system (Table 3; p < 0.001). Rates of discharge to long-term care facilities declined from 16.9% to 14.8%, 30-day mortality after hemorrhagic stroke decreased from 38.3% to 34.4% and 30-day mortality after ischemic stroke decreased from 16.3% to 15.7% after implementation of the Ontario Stroke System (Table 3; p < 0.01 for all comparisons). The median length of stay decreased from 7 to 6 days (p < 0.001), and the median time from stroke presentation to carotid revascularization decreased from 50 to 22 days (p < 0.001) after 2005 (Table 3).
Outcomes of patients with stroke or transient ischemic attack, before (Jan. 1, 2001–Mar. 31, 2005) and after (Apr. 1, 2005–Dec. 31, 2010) full implementation of the Ontario Stroke System
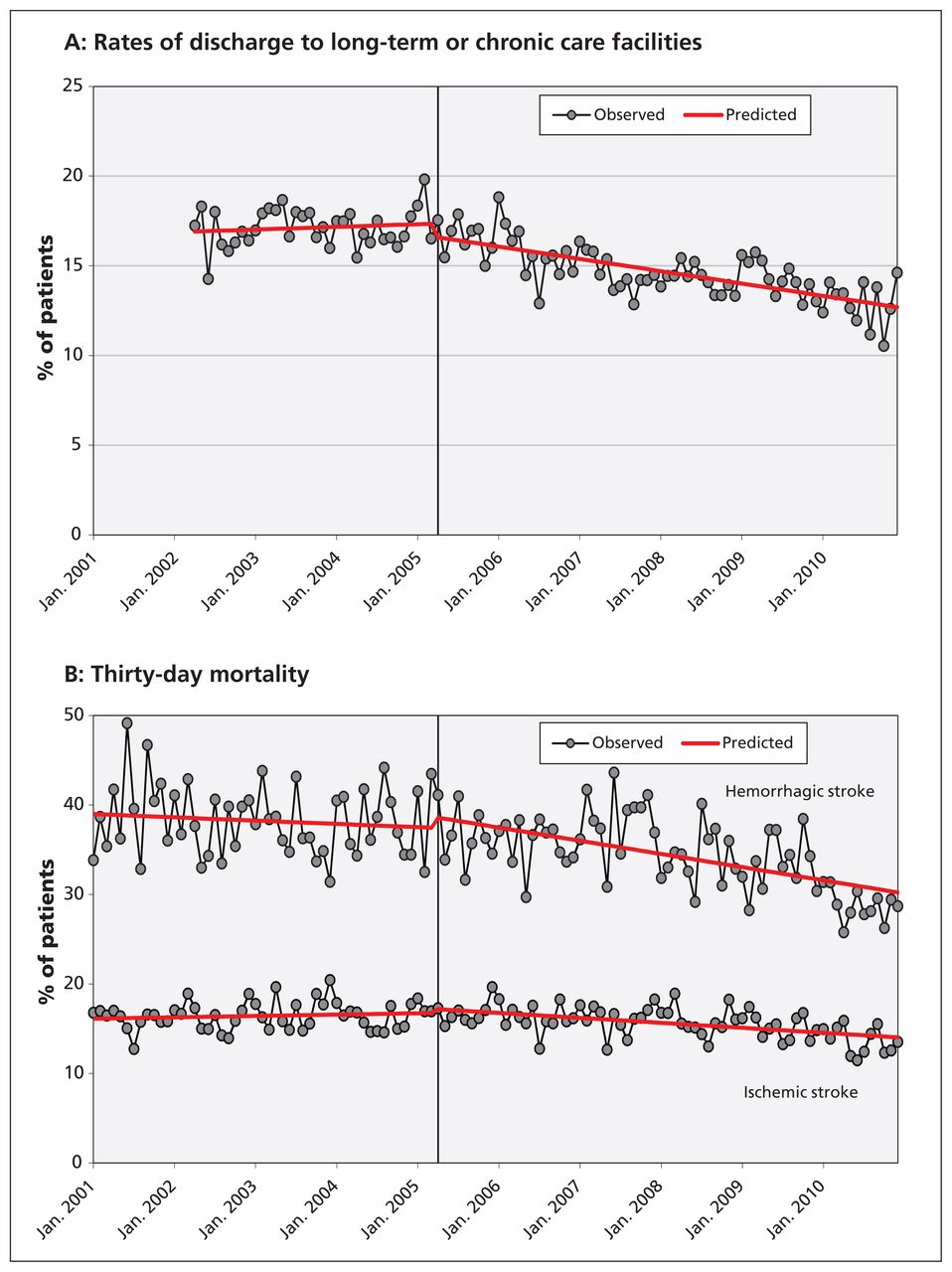
The piecewise regression analyses showed a gradual increase in rates of care at stroke centres between 2001 and 2005, followed by a significant upward shift in rates in 2005 (p < 0.01 for the change in level). This was not associated with an immediate shift in the risk of discharge to a long-term care facility after stroke or the risk of death, but rather it was associated with a decrease in the slope of these outcomes after 2005 (Figure 1; p < 0.05 for the change in slope for all outcomes).

(A) Rates of discharge to long-term or chronic care facilities after admission to hospital for stroke or transient ischemic attack from Apr. 1, 2002, to Dec. 31, 2010, adjusted for age, sex, stroke type and Charlson–Deyo comorbidity index score (p = 0.1 for a shift in rates after the intervention and p < 0.001 for a decrease in the slope after the intervention, using piecewise regression analyses). (B) Thirty-day mortality for patients admitted to hospital with hemorrhagic or ischemic stroke from Jan. 1, 2001, to Dec. 31, 2010, adjusted for age, sex and Charlson–Deyo comorbidity index score. Hemorrhagic stroke: p = 0.4 for a shift in rates after the intervention and p = 0.02 for a decrease in the slope after the intervention, using piecewise regression analyses. Ischemic stroke: p = 0.4 for a shift in rates after the intervention and p < 0.001 for a decrease in the slope after the intervention, using piecewise regression analyses.
Between 2002 and 2009, there were significant increases in rates of thrombolytic therapy (from 10% to 27%), neuroimaging (from 77% to 93%), carotid imaging (from 44% to 68%), care in a stroke unit (from 3% to 24%), dysphagia screening (from 47% to 57%), antithrombotic therapy (from 80% to 94%) and referrals to stroke prevention clinics (from 14% to 57%) (Table 4; p < 0.001 for all comparisons). Although improvements in care across the study period were seen at all hospital types, increases in care in a stroke unit and rates of thrombolytic therapy were greater at district and regional stroke centres, with little or no change at nondesignated centres (Table 4).
Care of patients with stroke or transient ischemic attack, from Apr. 1, 2002, to Mar. 31, 2009
Interpretation
We found that implementation of a provincial system of stroke care delivery was associated with increased rates of care at specialized stroke centres, improved processes of acute stroke care delivery and decreased rates of admission to a long-term care facility and death after stroke beyond what would be expected based on underlying temporal trends.
Stroke systems of care are designed to coordinate and optimize delivery of care across the continuum of stroke, from primary prevention to rehabilitation and reintegration.11,12,20,26 The American Stroke Association has provided detailed recommendations for the establishment of such systems, with key elements including collaboration among providers, the use of telemedicine to facilitate patient care in remote institutions and the identification of performance measures to evaluate the effectiveness of the system.11,27 In the area of acute care, the system of stroke care delivery should include the designation of comprehensive stroke centres and the development of regional strategies to ensure that all eligible patients receive interventions such as thrombolytic therapy and care in a stroke unit. The Ontario Stroke System includes all of these components.
Although a randomized controlled trial would be the most methodologically rigorous means of evaluating the effectiveness of a stroke system of care, this was not feasible in Ontario because of the complexity of the intervention and the desire to rapidly implement the system of care across the entire province. Instead, we used piecewise regression analyses to study the effect of the implementation of the system on outcomes among patients with stroke. Such analyses are a more robust experimental design than simple before-and-after comparisons because they allow the effect of the intervention to be distinguished from underlying temporal trends in outcomes and permit the assessment of both immediate and delayed changes in outcomes.28,29 Although a true causal relation between implementation of the Ontario Stroke System and improved patient outcomes cannot be established definitively on the basis of our study, the likelihood of a causal association is strengthened by the lack of major temporal confounders and by the concomitant improvements observed in processes of care, including those (i.e., care at a stroke centre, care in a stroke unit, thrombolytic therapy, medications for secondary stroke prevention) that have been previously shown to be associated with reduced death or disability from stroke.30–34
Although we observed an increase in the proportion of patients seen at designated stroke centres over the study period, the absolute magnitude of the increase was modest, with more than half of the population receiving care at nondesignated centres even 5 years following the full implementation of the stroke system. This is presumably a consequence of the system being designed primarily to facilitate the transfer or bypass of only those patients most likely to be candidates for thrombolytic therapy or neurosurgical interventions. Therefore, although the implementation of the system was associated with only about 1600 additional people receiving care at a stroke centre each year, this was accompanied by marked increases in rates of thrombolytic therapy and care in a stroke unit. The observed decreases in stroke-related mortality and admissions to long-term care facilities were relatively small. However, when applied to the population with stroke in Ontario, these decreases would be expected to result in about 200 fewer stroke-related deaths and 300 fewer patients requiring long-term or chronic care each year.
Despite the province-wide scope of the Ontario Stroke System, previous audits have shown persistent regional variations in care, and it is likely that access to care remains particularly challenging for patients in remote or rural areas.23 Although an ideal system might see all patients receiving care at specialized stroke centres, this may be difficult to achieve in large, geographically diverse jurisdictions such as Ontario. Such a system could also have unintended negative consequences, such as increased patient volumes at stroke centres and the need for transfer and assessment of patients who are later determined to have not had a stroke. Increased use of telemedicine may serve as a feasible alternative to ensure delivery of high-quality stroke care across an entire region, including remote areas. Between 2002 and 2012, the Ontario Telestroke Program provided neurologist consultation to about 3000 patients with stroke, 30% of whom received thrombolytic therapy.22
Limitations
Some limitations of our study merit emphasis. Although we studied the effect of the full implementation of the Ontario Stroke System in 2005, a phased introduction of the system occurred between 2000 and 2005, and thus our analyses almost certainly underestimate the overall effect of the stroke system on care and outcomes. Our study focused on hospital-based processes of care and outcomes, and we do not have information on longer-term outcomes such as functional status, quality of life or after-stroke care.
Although the piecewise regression analyses helped to distinguish the effect of the system from underlying temporal trends in care, they did not account for the potential effects of concurrent interventions. For example, the publication in 2004 of data suggesting that carotid endarterectomy is most effective if performed within 2 weeks of acute stroke35 likely contributed to the decline in waiting times for carotid revascularization before and after 2005. However, it is unlikely that all of the observed improvements in other outcomes could be fully explained by alternative interventions.
In our outcome analyses, we adjusted for key prognostic variables, including age, type of stroke and comorbid illness, but we were unable to adjust for stroke severity because this variable was not captured in our administrative data sources.
We did not evaluate the individual components of the Ontario Stroke System, and this study does not provide information on the relative effectiveness of the various interventions within the system. However, previous observational studies suggest that the establishment of stroke centres and the use of prehospital protocols may lead to improved processes of stroke care delivery.36,37
We did not perform a cost-effectiveness analysis; however, many of the individual components of the stroke system have been shown to be cost-effective.38–42
Finally, stroke care in Ontario is delivered within the context of Canada’s universal health care system, and our results and outcomes may not be easily replicated in countries without a single-payer system.
Conclusion
This study assessed the effect of the implementation of a system of stroke care delivery on important outcomes, including death and admission to a long-term or chronic care facility after stroke. Our findings provide strong support for the ongoing development and implementation of regional systems of organized stroke care delivery. Future research should focus on identifying the specific components of such systems that are most likely to account for improvements in outcomes.
Footnotes
Competing interests: Frank Silver has received payments for board membership, lectures or travel expenses from Boehringer Ingelheim Canada, Bristol-Myers Squibb, Sanofi Canada and Bayer Canada. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Moira Kapral was responsible for the conception of the study, and Jiming Fang performed the statistical analyses. All of the authors contributed to the study design, analysis plan and interpretation of results. Moira Kapral drafted the manuscript, which all of the authors revised. All of the authors gave final approval of the version submitted for publication.
Funding: The Ontario Stroke Registry is funded by the Canadian Stroke Network and the Ontario Ministry of Health and Long-Term Care. The Institute for Clinical Evaluative Sciences is supported by an operating grant from the Ontario Ministry of Health and Long-Term Care. The results and conclusions are those of the authors and should not be attributed to any supporting or sponsoring agencies. The funding agencies had no involvement in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review or approval of the manuscript.
Moira Kapral holds a Career Investigator Award from the Heart and Stroke Foundation of Canada. Frank Silver is supported by the Canadian Stroke Network. Jack Tu holds a Canada Research Chair in Health Services Research and a Career Investigator Award from the Heart and Stroke Foundation of Ontario.
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Inappropriate use of clinical practices in Canada: a systematic review
- Temporal Trends in Case Fatality, Discharge Destination, and Admission to Long-term Care After Acute Stroke
- Advances in Stroke 2017
- In-Patient Code Stroke: A Quality Improvement Strategy to Overcome Knowledge-to-Action Gaps in Response Time
- Long-term morbidity and mortality in patients without early complications after stroke or transient ischemic attack
- Risk of fractures after stroke: Results from the Ontario Stroke Registry
- Association between hospitalization and care after transient ischemic attack or minor stroke
- Integrated systems of stroke care and reduction in 30-day mortality: A retrospective analysis
- Does the Volume of Ischemic Stroke Admissions Relate to Clinical Outcomes in the Ontario Stroke System?
- Advances in Stroke: Health Policy/Outcomes Research 2013
More in this TOC Section
Similar Articles

