


See also practice article by Leis and Gold on page 559 and at www.cmaj.ca/lookup/doi/10.1503/cmaj.111143
A 39-year-old man presented with fever (38.7°C), cough and right chest pain on inspiration. His blood pressure was 125/75 mm Hg, heart rate was 88 beats/min, respiration was 20 breaths/min and oxygen saturation on room air was 94%. Physical examination was remarkable only for crackles over the right upper lung field. Results of blood tests showed an elevated leukocyte count of 16.5 (normal 4.0–10.0) × 109/L and were otherwise normal. Urinary testing for Legionella pneumophila and Streptococcus pneumoniae antigens was negative. Chest radiography showed pneumonia in the right upper lobe (Figure 1). Because the patient was at low risk for death (class I on the Pneumonia Severity Index),1 we prescribed oral penicillin and clarithromycin, and discharged the patient home. Follow-up chest radiography one month later showed that the consolidation had resolved (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.111256/-/DC1).
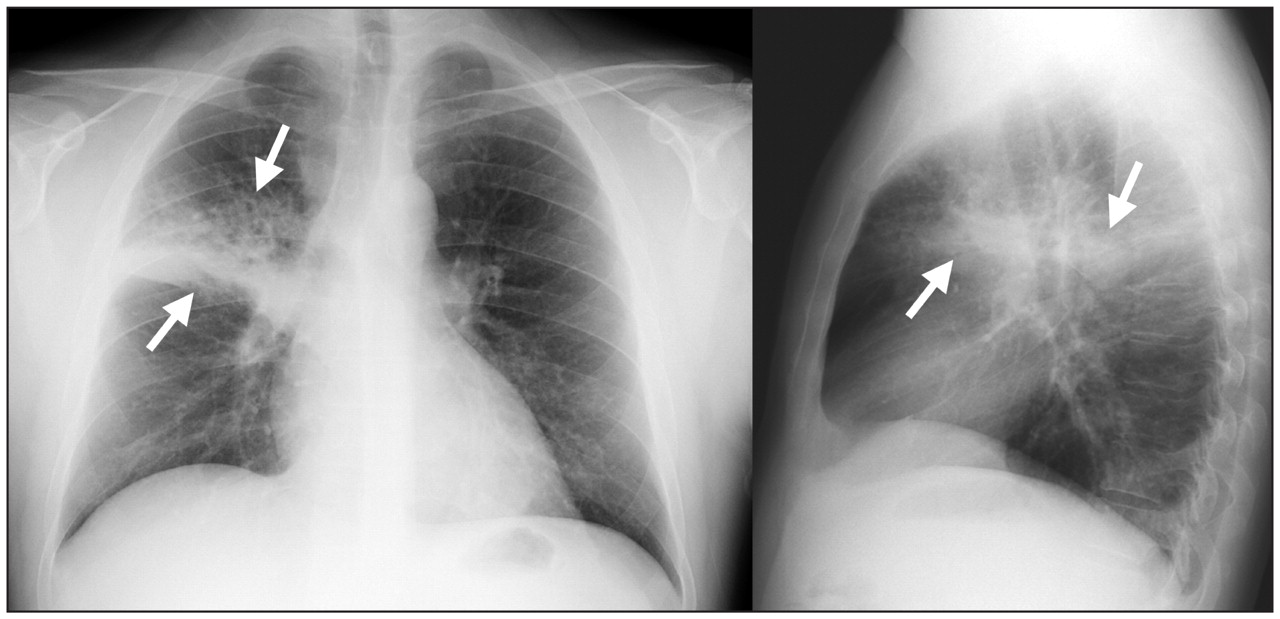
Posteroanterior and lateral radiographs of the chest of a 39-year-old man with fever, cough and pleuritic chest pain showing consolidation in the right upper lobe.
About 4 million instances of community-acquired pneumonia occur in the United States each year. It is one of the most common causes of death from infectious diseases worldwide.2 The precise diagnosis continues to be complex; at least 50% of causative pathogens remain unidentified, and all rigorous definitions of pneumonia require the finding of a pulmonary infiltrate on chest radiography.2 The initial antibiotic regimen should be chosen empirically to cover common typical and atypical pathogens. About 50% of patients with pneumonia can receive treatment outside of the hospital.2,3 The Pneumonia Severity Index is a validated prediction rule that identifies people with community-acquired pneumonia who are at low risk for death within 30 days of presentation.1 An alternative scale is the CURB-65, which takes into account confusion, urea level, respiration, blood pressure and age.4 A general rule of thumb is to admit patients with oxygen saturation under 92%.5
Helpful resources
-
The Pneumonia Severity Index calculator is available online at http://pda.ahrq.gov/clinic/psi/psicalc.asp
-
CURB-65 is available online at www.mdcalc.com/curb-65-severity-score-community-acquired-pneumonia
Footnotes
-
This article has been peer reviewed.
-
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

