


Article Figures & Tables
Figures
- Figure 1:
Flow chart for development of the study cohort (visits by adults aged 18–105 years from April 2007 to March 2009). ED = emergency department.
- Figure 2:
Median time to physician assessment among patients with a mental illness diagnosis (continuous lines) versus other patients (dashed lines) in the emergency department at 4 levels of crowding. Scores are based on the Canadian Triage and Acuity Scale guidelines. Note: MH = patient whose primary diagnosis in the emergency department was mental illness and who had a related chief complaint.
- Figure 3:
Median time from decision to admit the patient to ward transfer in patients with a mental illness diagnosis (continuous lines) versus all other emergency department patients (dashed lines), at 4 levels of crowding. *Value omitted because of a small sample size of admitted, low-acuity patients who were seen in severely crowded settings. Scores are based on the Canadian Triage and Acuity Scale guidelines. Note: MH = patient whose primary diagnosis in the emergency department was mental illness and who had a related chief complaint.
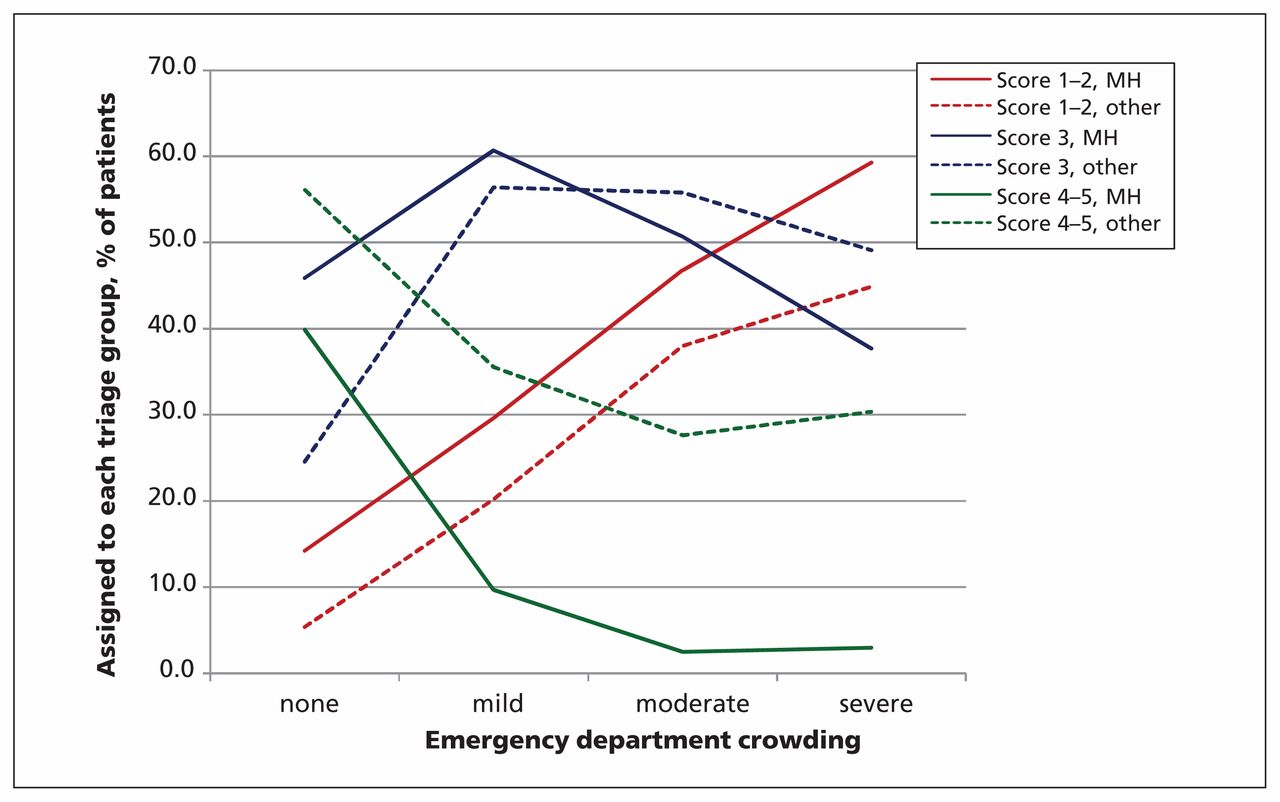
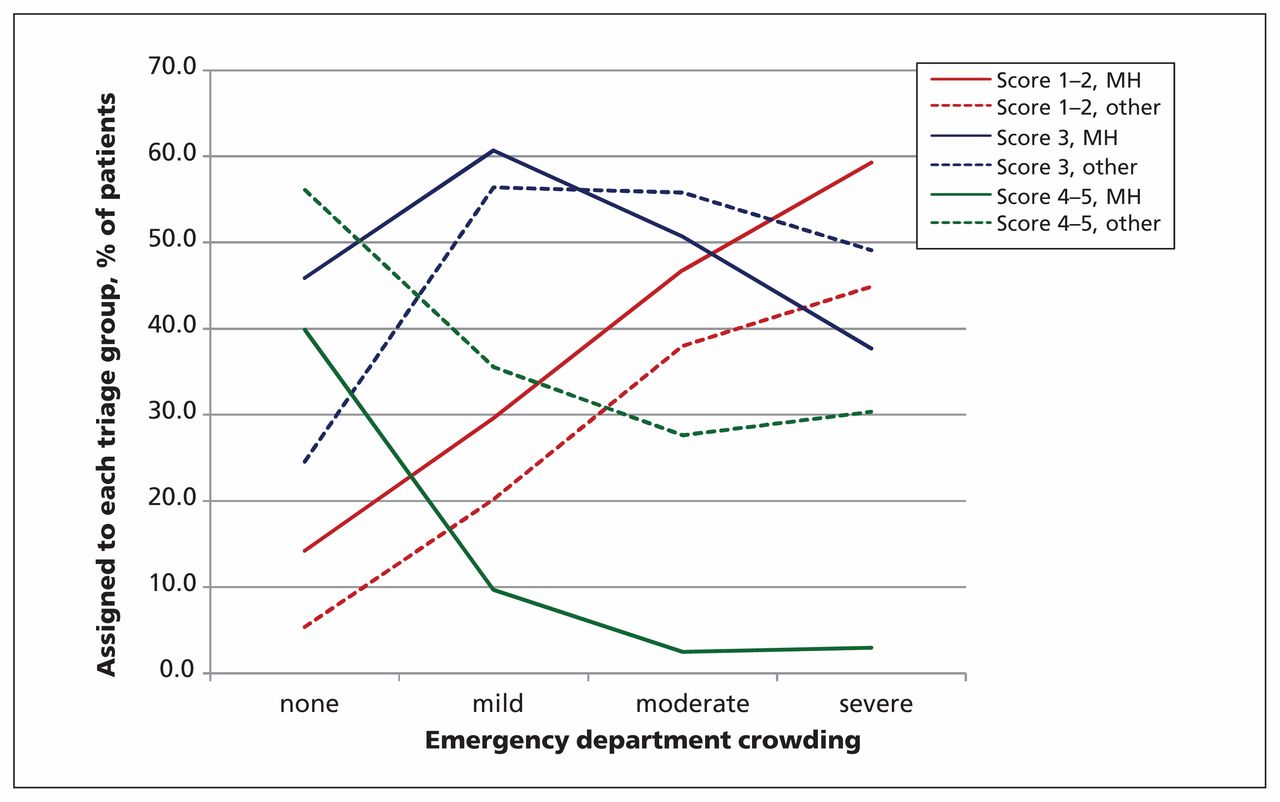
- Figure 4:
Percentage of patients assigned to each triage score at each level of emergency department crowding, by patient type. For example, during periods with no crowding, 40% (continuous green line) of patients with mental illness were assigned a low priority triage score. As crowding increased, the proportion of patients with mental illness assigned to these scores decreased to 10%, then 2.5%. For other patients, the proportion who received low priority scores also decreased as crowding increased (dashed green line), but remained above 25% of those patients. Scores are based on the Canadian Triage and Acuity Scale guidelines. Note: MH = patient whose primary diagnosis in the emergency department was mental illness and who had a related chief complaint.



Tables
- Table 1:
Baseline characteristics of the study cohort (patients with a primary emergency department diagnosis of a mood [affective] disorder or psychotic disorder and a related chief complaint)
Characteristic Primary diagnosis of mental illness Other diagnosis Index visits, no. 51 381 3 551 413 Age, mean ± SD 40.0 ± 15.3 48.0 ± 19.7 Female (%) 26 252 (51.1) 1 855 625 (52.3) Arrived by ambulance (%) 8 270 (16.1) 499 071 (14.1) Time to physician assessment,* median (IQR), min 82 (41–147) 75 (36–140) Time to physician assessment, mean ± SD, min 110 ± 107 103 ± 387 Length-of-stay, median (IQR), min 266 (147–493) 171 (92–302) Admissions, no. (%) 21 089 (41.0) 362 209 (10.2) Decision to admit time, median (IQR)†, min 74 (15–215) 152 (45–605) Decision to admit time, mean ± SD, min 374 ± 1 639 531 ± 2 467 Crowding status, no (%) No crowding‡ 14 151 (28.5) 1 585 295 (48.1) Mild crowding 28 026 (56.5) 1 429 061 (42.2) Moderate crowding 6 496 (13.1) 287 056 (8.5) Severe crowding 966 (1.9) 38 848 (1.1) Note: IQR = interquartile range, SD = standard deviation.
↵* 20.8% of patients had missing or unknown values.
↵† 10.2% of patients had missing or unknown values.
↵‡ A small proportion (3.4%) of visits could not be assigned to a crowding level because of low numbers of patients in that emergency department during a specific period.
- Table 2:
Unadjusted wait times and triage scores for patients with a primary diagnosis of mental illness or another diagnosis
Primary diagnosis of mental illness
n = 51 381Other diagnosis
n = 3 551 413p value Time to physician assessment, median (IQR), min Triage category 1/2 70 (35–130) 51 (25–110) < 0.001 Triage category 3 89 (45–155) 88 (44–163) 0.5 Triage category 4/5 83 (40–150) 71 (35–130) < 0.001 Time from admission decision to ward transfer, median (IQR), min Triage category 1/2 88 (24–260) 161 (46–640) < 0.001 Triage category 3 70 (15–204) 156 (48–623) < 0.001 Triage category 4/5 55 (5–150) 100 (13–346) < 0.001 Triage score, no. (%) 1–2 14 027 (27.3) 508 765 (14.3) < 0.001 3 27 668 (53.9) 1 415 701 (39.9) < 0.001 4–5 9 686 (18.9) 1 626 947 (45.8) < 0.001 Note: IQR = interquartile range.
- Table 3:
Wait times by level of crowding in the emergency department for patients with a primary diagnosis of mental illness or another primary diagnosis
Primary diagnosis; median (IQR) Unadjusted analysis Adjusted analysis Mental illness
n = 51 381Other
n = 3 551 413Difference between patient types p value Difference between patient types (95% CI) p value Time to physician assessment,*min Not crowded 62 (32–110) 56 (30–97) 8 < 0.001 10 (8 to 11) < 0.001 Mild crowding 90 (47–156) 104 (50–179) −14 < 0.001 −14 (−12 to −15) < 0.001 Moderate crowding 110 (55–202) 143 (60–268) −33 < 0.001 −39 (−35 to −42) < 0.001 Severe crowding 96 (48–211) 146 (51–332) −50 < 0.001 −48 (−39 to −56) < 0.001 Decision to admit time† Not crowded 55 (8–144) 97 (25–287) −42 < 0.001 −5 (0 to −9) 0.002 Mild crowding 86 (24–255) 179 (58–705) −93 < 0.001 −59 (−56 to −63) < 0.001 Moderate crowding 86 (24–246) 247 (77–865) −161 < 0.001 −128 (−121 to −134) < 0.001 Severe crowding 83 (23–260) 238 (64–774) −155 < 0.001 −106 (−86 to −134) < 0.001
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

