


Abstract
Background: Patients surviving certain types of cancer are at increased risk of a second primary cancer. We tested the hypothesis that excess risk of a second primary cancer is due mainly to excess risk of it being the same type of cancer as the first, rather than to excess risk of it being a different type.
Methods: We conducted a nationwide study using data from three dabatases for the entire Danish population (n = 7 493 705) from 1980 through 2007. For each type of cancer, we performed a nested study matching each patient with incident cancer diagnosed in that period with up to five controls who did not have the examined cancer at the time of diagnosis. We used Cox regression models to calculate individual risk estimates and meta-analysis techniques to calculate aggregated risk estimates.
Results: A total of 765 255 people had one or more diagnoses of primary cancer (total 843 118 diagnoses) during the study period. The aggregated hazard ratio (HR) for risk of any second primary cancer after any first cancer was 1.25 (95% confidence interval [CI] 1.24–1.26), with heterogeneity among cancer types. The aggregated HR for risk of a second primary cancer of the same type as the first was 2.16 (95% CI 1.98–2.34). The aggregated HR for risk of a second cancer of a different type from the first was 1.13 (95% CI 1.12–1.15). Results were similar when we excluded second primary cancers occurring within 1, 2, 5 or 10 years after the first cancer. Overall, we observed 74 significant associations among 27 types of first cancer and 27 possible types of second primary cancer.
Interpretation: Excess risk of a second primary cancer was due mainly to a 2.2-fold risk of the second cancer being the same type as the first, whereas the risk of it being a different type was only 1.1-fold. However, heterogeneity among cancer types was substantial.
See related commentary by Winget and Yasui at www.cmaj.ca/lookup/doi/10.1503/cmaj.111424
Second primary cancers are seen in 15% of cancer survivors, resulting in increased morbidity and mortality.1 Overall, patients surviving certain types of cancer are at increased risk of a second primary cancer.2–4 It is unclear, however, whether this excess risk is due mainly to excess risk of the second primary cancer being the same type as the first cancer, or to excess risk of it being a different type from the first. Clinically, this is an important question, because a clear answer may help target continued surveillance of patients with cancer for the development of second primary cancers.
Previously, the risk of second primary cancers was estimated through pair-wise examination of the risk of a specific second primary cancer following a specific first cancer5–9 and in studies of the risk of a second cancer of the same type as the first.10–13 We tested the hypothesis that excess risk of a second primary cancer is due mainly to excess risk of it being the same type of cancer as the first, rather than to excess risk of it being a different type. We studied the entire Danish population over a 28-year period using data from three national databases and calculated aggregated risk estimates across all cancer types and individual risk estimates for the different cancer types.
Methods
Study population
We reviewed data from three national databases for all people living in Denmark (about 7.5 million) from 1980 through 2007. We chose this study period because the three databases had complete data for that period. For baseline characteristics of the population, we used data from the national Danish Civil Registration System. This database records all births, immigrations, emigrations and deaths in Denmark through the civil registration number, which uniquely identifies each inhabitant of Denmark and includes information on age and sex. This database is 100% complete, that is, for practical purposes no one is lost to follow-up.
For other characteristics, we collected data from Statistics Denmark on ethnicity, highest obtained level of education and residence (size of city).
Cancer diagnoses
We identified people with incident cancer diagnosed from Jan. 1, 1980, to Dec. 31, 2007, using the national Danish Cancer Registry, which identifies 98% of all incident cancers in Denmark.14 Since 1987, all doctors in hospitals and private practices are required by law to report all diagnoses of cancer to the registry. The only cancer screening program in Denmark was for cervical cancers, from 1998 to 2007. All diagnoses in the registry are assigned based on results of histologic examination by a fully trained pathologist. The registry uses a conservative strategy to avoid misclassification of relapse of the first cancer and records only true occurrence of a second primary cancer of the same type.15
We classified diagnoses according to the International Classification of Diseases (ICD) 7th edition codes 140.0–207.0 for the period 1980–2003, and ICD 10th edition codes C00.0–C96.0 and D00.0–D09.0 for the period 2004–2007 (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110167/-/DC1).
Statistical analysis
All analyses were performed on data for individual participants. All tests were two-sided. We calculated age-standardized incidence rates according to the World Health Organization world standard population.16 We used Wald tests and Cox regression models with delayed entry at age of diagnosis (left-truncated); Cox regression models were used to calculate hazard ratios (HRs) with 95% confidence intervals (CIs) as a measure of relative risk. We used multivariable models adjusted for age at diagnosis, date of birth, sex, ethnicity, highest obtained level of education and residence. We assessed the assumption of proportional hazards over time graphically and detected no major violations.
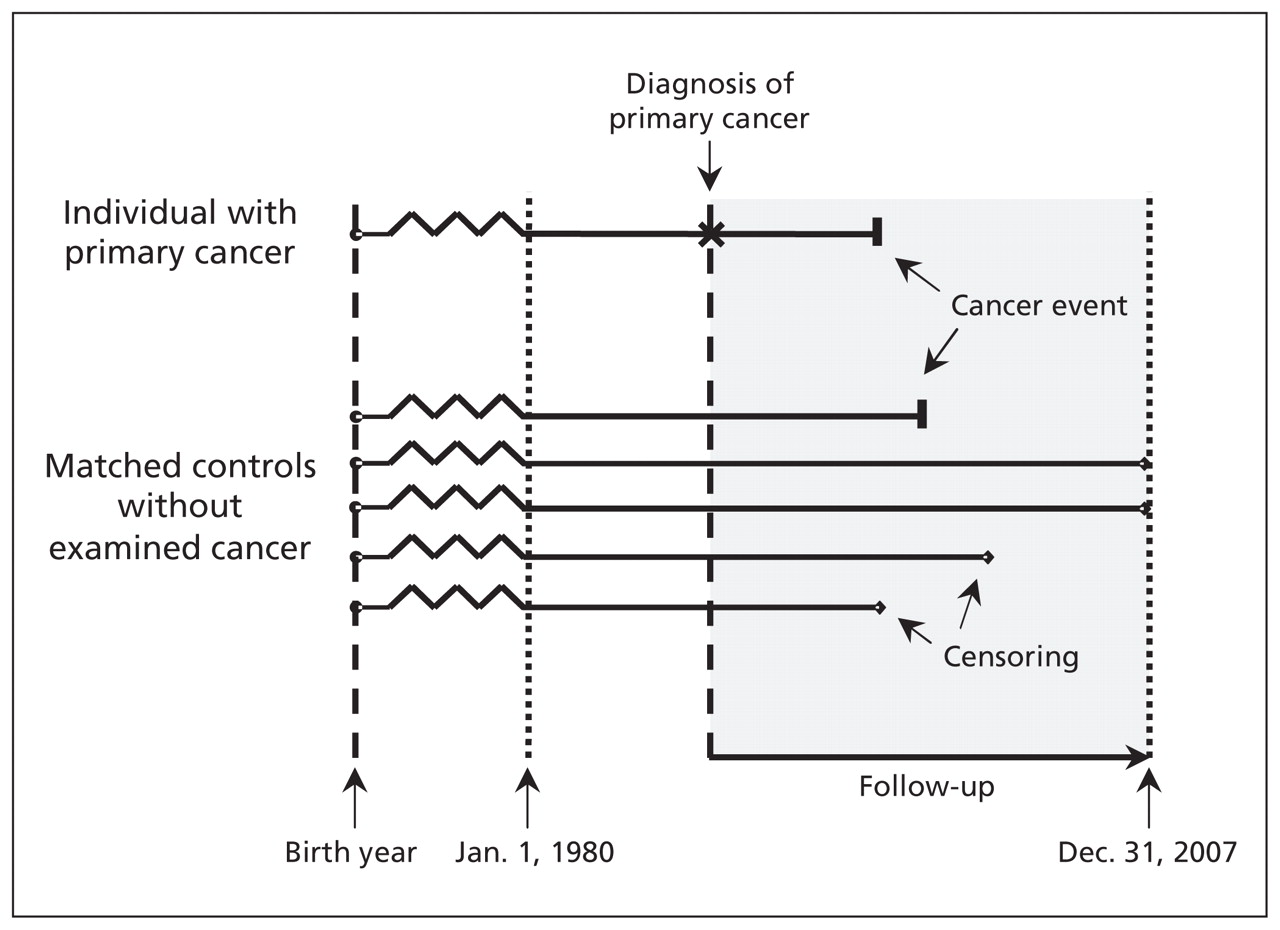
All analyses were based on nested studies, whereby each person with cancer was matched (by sex, birth year, calendar period at risk and age at diagnosis of the cancer) with up to five randomly selected controls from the general population who did not have cancer of the same type as the patient’s on the date the patient’s cancer was diagnosed (but could have had another type of cancer) (Figure 1). The randomly selected control population could therefore differ from analysis to analysis. In all analyses, there was at least one control available for each patient, and no patients were excluded from the analysis. For each matched subset, follow-up of the patient and matched controls began on the date the patient’s cancer was diagnosed and ended on the date of emigration, death, Dec. 31, 2007, or diagnosis of a primary cancer, whatever came first. Mortality was accounted for as a competing risk by censoring at date of death for individual participants (information that is 100% complete in Denmark).

Follow-up of Danish population from 1980 through 2007 for diagnoses of primary cancers. Of 7 493 705 individuals, 765 255 received a diagnosis of one or more primary cancers during the study period, for a total of 843 118 cancer diagnoses. All analyses were based on nested studies, whereby each individual with cancer was matched (by birth year, sex, calendar period at risk and age at diagnosis) with up to five controls who, up until the time of matching, did not have the examined cancer. Four outcomes were possible for both cancer patient and controls: diagnosis of a primary cancer, censoring because of death, censoring because of emigration, and end of follow-up (here illustrated for the controls).
We First examined the association between 27 types of cancers and increased risk of any second primary cancer. We used fixed-effect meta-analysis techniques for the individual HR estimates across the 27 cancer types to compute aggregated HR estimates. Because tobacco use is a common risk factor for several cancers, we also calculated aggregated HR estimates according to the relation of the first cancer to tobacco use (related, not related and relation uncertain).17 Because protocols for treating cancer in children differ from those for treating cancer in adults, we also computed aggregated HR estimates according to whether the first cancer was diagnosed in childhood (< 14 years) or later. We measured heterogeneity among cancer types using the I2 statistic.
Second, for each of the 27 types of cancer, we examined whether excess risk of a second primary cancer was due mainly to excess risk of the second cancer being the same type as the first cancer or to excess risk of it being a different type. We used fixed-effect meta-analysis techniques to compute aggregated estimates as described earlier.
Third, we performed sensitivity analyses to examine the potential influence of a relapse of the first cancer being erroneously diagnosed as a second primary cancer of the same type. We advanced the time at entry for patients and controls to 1, 2, 5 and 10 years after the diagnosis of the first cancer of the patient. We computed aggregated estimates as described earlier. In addition, we assessed associations between any of the 27 types of first cancer and any of the 27 types of second primary cancer, for 729 individual associations (minus 12 non-existent sex-specific associations). For these 717 associations, we report HRs with 95% CIs, and we indicate which HRs were significant after Bonferroni correction for multiple comparisons (i.e., p < 0.05/717 = 0.00007). Finally, using Poisson regression models, we estimated the absolute risk per 100 of a second primary cancer occurring within five years after diagnosis of the first cancer among both the patients and the controls.
Results
During the 28-year study period, the cohort included 7 493 705 people, with 143 million person-years of follow-up. A total of 765 255 individuals had one or more cancers during the study period, for a total of 843 118 diagnoses of cancer. The number of people with successive cancers and the median time between them are shown in Appendix 2. Age-standardized incidence rates and median age at diagnosis for the 27 cancer types are listed in Appendix 1. Baseline characteristics of the cohort and the 765 255 individuals with cancer are shown in Appendix 3. (The appendices are available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.110167/-/DC1).
Risk of second primary cancer
The risk of any type of second primary cancer after any type of first cancer varied from a reduced risk after prostate cancer (adjusted HR 0.80, 95% CI 0.77–0.83) to an increased risk after cancer of the larynx (adjusted HR 1.87, 95% CI 1.77–1.97) (Figure 2). The aggregated HR for risk of any second primary cancer after any first cancer was 1.25 (95% CI 1.24–1.26), with substantial heterogeneity among cancer types (I2 = 98.6%). Figure 2 also shows the aggregated HR estimates according to whether the first cancer was related to tobacco use and whether the first cancer was diagnosed in childhood or later.

Risk of any second primary cancer after a first primary cancer, by type of first cancer. Hazard ratios (HRs) greater than 1.0 indicate an increased risk of a second primary cancer of any type. CI = confidence interval.
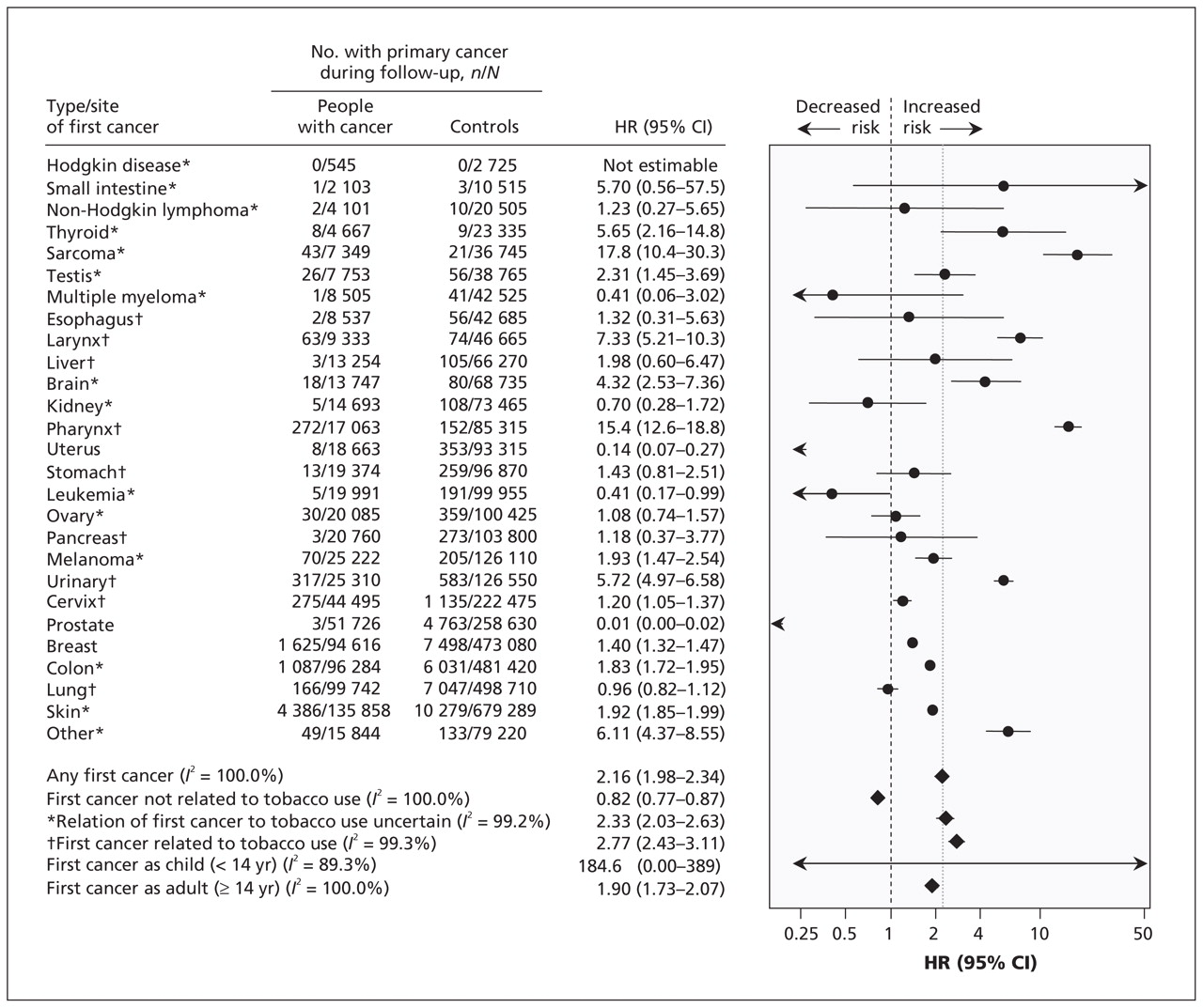
The risk of a second primary cancer of the same type as the first cancer was reduced after prostate cancer (adjusted HR 0.01, 95% CI 0.00–0.02) and was greatest after sarcoma (adjusted HR 17.8, 95% CI 10.4–30.3) (Figure 3). The aggregated HR for risk of a second cancer of the same type as the first was 2.16 (95% CI 1.98–2.34) for any first cancer, with substantial heterogeneity among cancer types (I2 = 100%).

Risk of a second primary cancer of the same type as the first cancer, by type of first cancer. Hazard ratios (HRs) greater than 1.0 indicate an increased risk of a second primary cancer of the same type as the first. The number of controls for each type of cancer in Figures 3 and 4 do not necessarily add up to the number of controls in Figure 2, because the controls were randomly selected for each analysis. CI = confidence interval.
The risk of a second primary cancer of a different type from the first cancer was reduced after prostate cancer (adjusted HR 0.79, 95% CI 0.77–0.82) and was greatest after cancer of the larynx (adjusted HR 1.78 (1.68–1.88) (Figure 4). The aggregated HR for risk of a second cancer of a type different from the first was 1.13 (1.12–1.15) for any first cancer, with substantial heterogeneity among cancer types (I2 = 98.4%).

Risk of a second primary cancer of a different type from the first cancer. Hazard ratios (HRs) greater than 1.0 indicate an increased risk of a second primary cancer of a different type from the first. The number of controls for each type of cancer in Figures 3 and 4 do not necessarily add up to the number of controls in Figure 2, because the controls were randomly selected for each analysis. CI = confidence interval.
Sensitivity analyses
In our sensitivity analyses of the potential influence of a relapse being erroneously diagnosed as a second primary cancer of the same type, we found that the results were similar to those of the main analyses when we excluded second primary cancers occurring within 1, 2, 5 and 10 years after the first cancer (Table 1). The aggregated HR estimates for risk of a second primary cancer of the same type as the first cancer increased slightly, from 2.16 (95% CI 1.98–2.34) without exclusion to 2.40 (95% CI 2.00–2.80) after exclusion of second cancers diagnosed within 10 years after the first cancer. The corresponding HRs for risk of a second primary cancer of a different type from the first cancer increased from 1.13 (95% CI 1.12–1.15) for any first cancer to 1.27 (95% CI 1.23–1.31).
Sensitivity analyses of duration between first and second cancer*
When we assessed the association between any of the 27 first types of cancer with any of the 27 possible types of second primary cancer, we observed 74 significant associations (p < 0.001) after Bonferroni correction for multiple comparison (Table 2). Corresponding estimates of the five-year absolute risk per 100 among patients and controls are shown in Table 3.
Relative risk of second primary cancer after first cancer in Danish population, 1980–2007*
Five-year absolute risk per 100 of second primary cancer after first cancer in Danish population, 1980–2007*
Interpretation
The principal finding of this nationwide study was that excess risk of a second primary cancer was due mainly to a 2.2-fold risk of the second cancer being the same type as the first, whereas the risk of it being a different type was only 1.1-fold.
For each of the significant associations we observed between the 27 types of first cancer and the 27 possible types of second primary cancer, three possible explanations need to be considered. First, the characteristics of the individual patient in terms of genetic and lifestyle risk factors may predispose the person to both cancer types. For example, the increased risk of a second primary cancer in the thyroid or other endocrine glands after a first thyroid cancer may be due to the known clustering of multiple endocrine neoplasia. Second, the characteristics of ascertainment (i.e., diagnostic procedures) may have been a factor. Some diagnostic or monitoring examinations for one type of cancer may influence the likelihood of detecting another type of cancer. The third possible explanation relates to the characteristics of treatment of the first cancer. Surgical removal of the whole or major parts of the affected organ would tend to reduce the risk of a second primary cancer of the same type as the first, whereas chemotherapy and radiation therapy may increase the risk of a second primary cancer of the same or different type as the first.
The lack of detail in the available registry data prohibited us from determining which mechanisms played a role in the individual associations between first and second primary cancers. Nonetheless, the striking contrast between the 2.2-fold increased risk of a second primary cancer being the same type as the first and the 1.1-fold increased risk of it being different from the first cancer suggests that characteristics of the individual patient were involved. Thus, the risk of a second primary cancer seems to be specific to cancer type and is probably driven by the patient’s genetic and lifestyle risk factors.
The contrast between the risk of a second primary cancer being the same as the first and the risk of it being different from the first was higher in the group of tobacco-related cancers than in the group of cancers not related to tobacco use or whose relation to tobacco use was uncertain. This observation suggests that, even though risk factors display a pleiotropic association at the population level with increased risk of multiple cancer types, the increased risk at the individual level may still be specific to cancer type.
Our findings from the sensitivity analyses underline that codiagnosis of a second primary cancer probably does not influence our main findings. Second, because the risk of a second primary cancer of the same type as the first changed only slightly after we excluded all primary cancers diagnosed up to 10 years after the first cancer, short-term malignant progression of dysplastic cells in anatomic proximity of the first cancer seems less likely as the only explanation for the observed 2.2-fold risk of a second cancer of the same type as the first. Rather, we speculate that in general, risk factors acting over the long term seem to be type specific in the individual patient. However, other explanations are also plausible: effects of treatment and an increase (or decrease) in diagnostic surveillance could change observed risk of cancer in the same organ as opposed to other organs.
Limitations
One limitation of our study is the possible misclassification of cancer diagnoses. However, classification errors likely did not have a major effect on our findings because all diagnoses of cancer from the national Danish Cancer Registry are assigned based on histologic examination by a fully trained pathologist. Misclassification of relapse of the first cancer as a second primary cancer was also a possible source of bias; however, observed associations did not change significantly even after we excluded second cancers diagnosed up to 10 years after the first cancer. If anything, the national Danish Cancer Registry underreports second primary cancers of the same type as the first cancer.15 Another limitation concerns the availability and completeness of the diagnostic information; however, the Danish Cancer Registry captures 98% of all cancer diagnoses in Denmark.14,18
The broad-stroke nature of the aggregated HR estimates of all cancer types combined disregards the substantial heterogeneity in risk across individual types of cancer, as illustrated by the high I2 values. The interplay of risk factors differs for individual types of cancer; therefore, the aggregated risk estimates may have limited clinical relevance. However, in Table 2 we provide all of the associations between the 27 individual first cancers and the 27 individual second primary cancers without Bonferroni correction for multiple comparison.
Conclusion
In this nationwide study, the excess risk of a second primary cancer was due mainly to a 2.2-fold risk of the second primary cancer being the same type as the first, whereas the risk of it being a different type was only 1.1-fold. Future studies of individual pairs of first and second primary cancers should clarify whether the association is due to shared genetic or lifestyle risk factors, codiagnosis of a primary cancer in close anatomic proximity to the first cancer, treatment of the first cancer, or the timing of diagnosis of the first cancer (in childhood v. adulthood). Our present findings may assist clinicians in designing surveillance programs for their patients who have cancer, for example by focusing on second primary cancers with the highest five-year absolute risks.
Footnotes
Competing interests: Stig Bojesen has received research grants from the Danish Cancer Society. No competing interests declared by Sune Nielsen or Børge Nordestgaard.
This article has been peer reviewed.
Contributors: All of the authors designed the study. Sune Nielsen obtained the necessary permissions to use the data from the individual registries, processed and organized the data for analysis, and performed the statistical analyses. All of the authors analyzed and interpreted the data. Sune Nielsen drafted the manuscript, and Børge Nordesgaard and Stig Bojesen critically revised it for important intellectual content. All of the authors approved the final version submitted for publication.
Funding: The study was funded by the Herlev Hospital, Copenhagen University Hospital.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Validating risk prediction models for multiple primaries and competing cancer outcomes in families with Li-Fraumeni syndrome using clinically ascertained data at a single institute
- Estimating the Risk for Secondary Cancer After Targeted {alpha}-Therapy with 211At Intraperitoneal Radioimmunotherapy
- Second Malignant Neoplasms in Patients With Cowden Syndrome With Underlying Germline PTEN Mutations
- Variation in risk of second primary cancer
More in this TOC Section
Similar Articles
Collections

