


A 36-year-old man presented to the emergency department because of gradual blurring of vision in his right eye over 20 days and progressive loss of vision in the left eye over the previous eight months. One year earlier, he had started taking sodium valproate for morning migraines with only a partial response. Visual acuity was 20/30 (66.7%) in the right eye, and he could perceive only hand motions with the left eye. He also had a left relative afferent pupillary defect. Funduscopy showed a pale left optic disk and edema of the right optic disk (Figure 1). The other results of neurologic examination were normal.
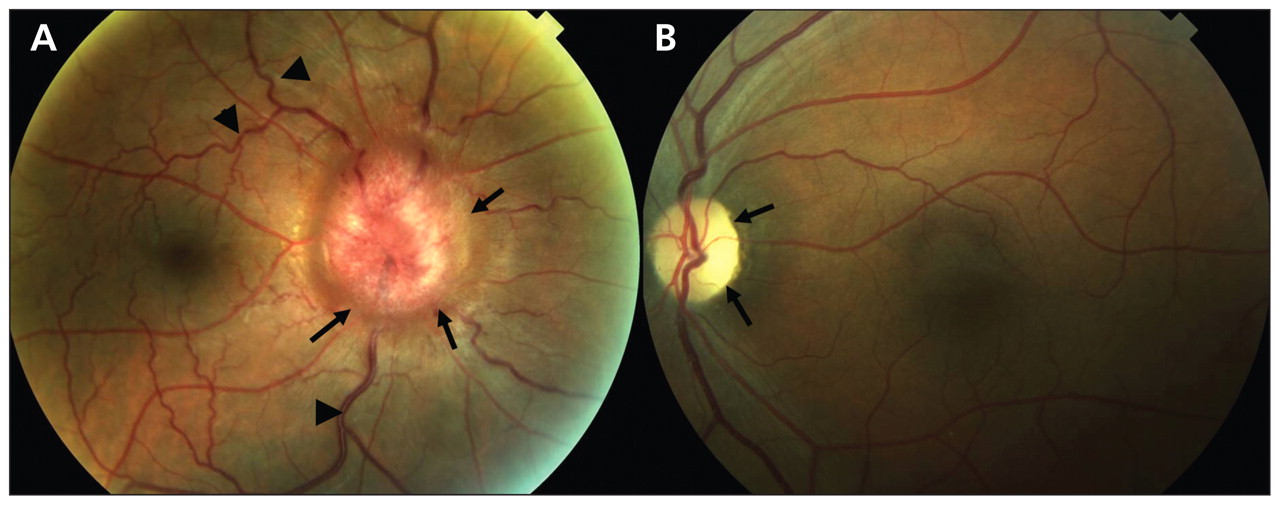
Funduscopy in a 36-year-old man with headaches and loss of vision. (A) Edema of the optic disk (arrows) in the chronic phase (“champagne cork”) is visible in the right fundus, with venous tortuosity and dilatation (arrowheads). (B) Left funduscopy shows a pale optic disk, consistent with axonal death. The lack of colour is more marked in the temporal area (arrows).
These findings suggested Foster Kennedy syndrome, in which an anterior intracranial mass directly compresses the ipsilateral optic nerve, causing atrophy, and increases intracranial pressure, which results in contralateral papilledema.1 Cranial computed tomography showed a mass arising from the left anterior clinoid process (see Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.101937/-/DC1). Systemic dexamethasone and phenytoin were started prophylactically, and the patient was admitted for surgical excision of the mass. At follow-up one year after the surgery, visual acuity in the right eye had improved to 20/20 (100%), and the patient was able to count fingers with his left eye.
Foster Kennedy syndrome is thought to be present in 1% to 2.5% of intracranial masses.2 Tumours of the frontal lobe can become quite large before they are discovered, and focal symptoms (e.g., memory loss or emotional lability) may be sparse. Although the increase in intracranial pressure correlates with the size and location of the tumour,2 related symptoms may be subtle and less prominent than pupillary changes, if the elevation of pressure is longstanding.3 Recovery of visual acuity may occur with normalization of the intracranial pressure. This case highlights that a diagnosis of migraine should be questioned when the headache is atypical, is only partially controlled by medications or is associated with other neurologic symptoms.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

