


The knowledge-to-action cycle represents a framework for the implementation of knowledge. 1 As discussed in the first article in this series, the action phases of this cycle were derived from a review of 31 theories of planned action. 2 Included in this cycle (Figure 1) are the processes needed to implement knowledge in health care settings. In this paper, we address the adaptation of the knowledge to the local context and assessment of barriers to and facilitators of the use of knowledge. The action cycle is a dynamic and iterative process with each phase informing the others.
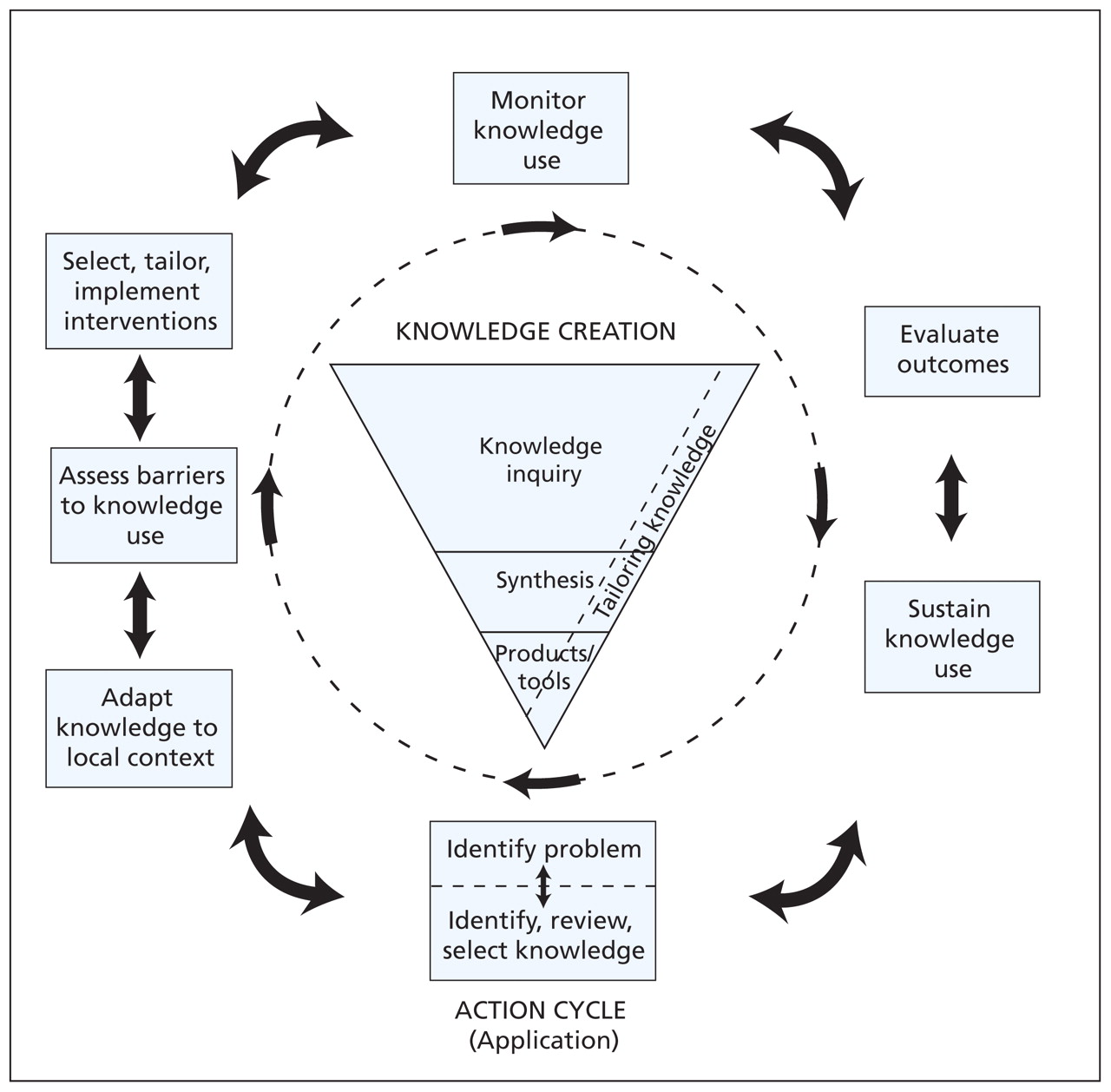
Figure 1: The knowledge-to-action cycle.
Why adapt guidelines for local use?
Using the best evidence is a fundamental aspect of quality health care and valid guidelines for clinical practice are an important tool to inform evidence-based practices. Guidelines are derived from synthesized evidence that has been translated into specific practice-oriented recommendations. 3 The production of guidelines has been promoted and supported by governments and professional organizations as a mechanism for reducing variations in practice. Many countries have infrastructure at the national or regional level dedicated to synthesizing evidence and producing guidelines, as well as incentives designed to support practices guided by current recommendations of guidelines. 4
The goals of these initiatives differ depending on the political context and the health care system. For instance, in the United Kingdom, the National Health Service has infrastructure and incentives to deliver care guided by recommendations of guidelines. National bodies such as the National Institute for Health and Clinical Excellence 5 are dedicated to synthesizing evidence and producing guidelines for use within the National Health Service. To assess the uptake and adherence to guideline-based care, auditing functions exist across trusts (i.e., regions) in the National Health Service. Despite these efforts, evaluation of these strategies for implementation show that overall conformity of practices lags behind expectations. 6
Although high-quality guidelines may be seen as necessary, they are not sufficient to ensure evidence-based decision-making. Uptake of knowledge does not occur with simple dissemination and usually requires a substantive, proactive effort to encourage use at the point of decision-making. 7 The gap between valid recommendations of guidelines and delivery of care based on this evidence may be due to numerous barriers. For instance, clinicians may not have the requisite skills and expertise to implement a recommended action (e.g., being unfamiliar with how to initiate or titrate a new medication), or the setting may not have the mandatory equipment or its staff the time to deliver a guideline’s recommendation. 3
Although guidelines provide evidence in a more usable form for clinicians than a plethora of primary studies, an important and additional necessary step is the adaptation of the guideline to the local context of use. National and international bodies have made major efforts to improve the quality and rigour of guidelines, 8,9 but less investment has been made in understanding how guidelines can be targeted to the local context of health care. By local, we mean a continuum of contexts that could range from a single clinic to a hospital, region or nation.
Customizing a clinical practice guideline to a particular organization may improve acceptance and adherence. Active involvement of the end-users of the guideline in this process has been shown to lead to significant changes in practice. 10–13 For example, local and regional adaptations of international evidence-based practice guidelines have become mandatory for the care of patients with cancer in France. 14 For many regions and territorial jurisdictions, de novo development of guidelines is not feasible because of lack of time, expertise and resources, and thus taking advantage of existing high-quality guidelines is sensible. 15–17
Adaptation of existing high-quality guidelines for local use is an approach with the potential to reduce duplication of effort and enhance applicability. National guidelines often lack details on applicability and description of the changes in the organization of care required to apply the recommendations. 18 Adaptation of evidence may promote local uptake of evidence through a sense of ownership by the end-users who are engaged in this process. However, customizing a guideline to local conditions could weaken the integrity of the evidence base. We outline a systematic, participatory approach for evaluating and adapting available guidelines to a local context of use while maintaining the quality and validity of the guideline. Whether evidence is provided in the format of syntheses of knowledge, patient decision aids or clinical practice guidelines, end-users must consider if or how it could be adapted to the local context and the same principles can be applied to ensure these factors are considered before implementation of the evidence.
To illustrate how to adapt guidelines, we will use a recent study that was performed to improve community care of individuals living with venous ulcers of the leg. 10,13 Regional managers of home care were concerned about costs of supplies, amount of nursing time, and frequency of visiting for clients with ulcers of the leg. A regional task force was developed to review existing practice guidelines to help guide the care plan. The task force identified that many of these guidelines were from international bodies and would require adaptation to the local context.
How are guidelines adapted for local use?
Existing guidelines can be evaluated and customized to fit local circumstances through an active, systematic and participatory process. This process must preserve the integrity of the evidence-based recommendations when differences in organizational, regional or cultural circumstances may legitimately require important variations in recommendations. 8,9,14–16,19 In adapting a guideline, consideration is given to local evidence, such as specific health questions relevant to a local context of use; to specific needs, priorities, legislation, policies and resources; to scopes of practice within the local health services; and to fit within existing models of delivery in the targeted setting. Adapting the guideline to this local evidence is assumed to improve uptake of the guidelines.
Returning to our example involving care of ulcers of the leg, the task force collectively assessed the quality of individual guidelines and their recommendations. They developed a protocol that was feasible to implement locally and that was endorsed by stakeholders. The guideline was condensed to a one-page algorithm to enhance use by the clinicians, and documentation forms were created for collection of clinical data. For example, to streamline the process of assessment and facilitate application of evidence-based care, documentation forms were created to collect information about the cause of the ulcer, with venous symptoms and history on one side of the page and arterial symptoms on the other.
With the exception of a few studies such as this collaboration for care of ulcers of the leg, 10,13,17 no validated process for the adaptation of guidelines has been documented. Recently, the Canadian work 16 in this area was integrated with an international initiative known as the ADAPTE collaboration (www.adapte.org). 19 This collaboration is a group of researchers and developers, implementers and users of guidelines whose aim is to enhance the use of research-based evidence through more efficient development and implementation of practice guidelines. The ADAPTE process was developed to facilitate the creation of efficient, high-quality adapted guidelines. The process engages end-users in the guideline adaptation process to address specific health-related questions relevant to its context of use. The goal is to establish a standard of being transparent, rigorous and replicable based on the following core principles:
-
Respect of evidence-based principles in the development of guidelines, 20
-
Use of reliable and consistent methods to ensure the quality of the adapted guideline, 9,19
-
Participation of key stakeholders to foster acceptance and ownership of the adapted guideline and ultimately promote its use, 13,14
-
Consideration of context during adaptation to ensure relevance for local practice and policy, 13,21
-
Transparent reporting to promote confidence in the recommendations of the adapted guideline, 9,20
-
Use of a flexible format to accommodate specific needs and circumstances, 18,22 and
-
Respect for and acknowledgement of guideline materials used as sources.
What is the ADAPTE process?
The ADAPTE process consists of three main phases, including planning and set-up, adaptation, and development of a final product (Box 1). The set-up phase outlines the necessary tasks to be completed before the process of adaptation, including identifying necessary skills and resources, and designing the panel. The panel should include relevant end-users of the guideline, such as clinicians, managers and patients.
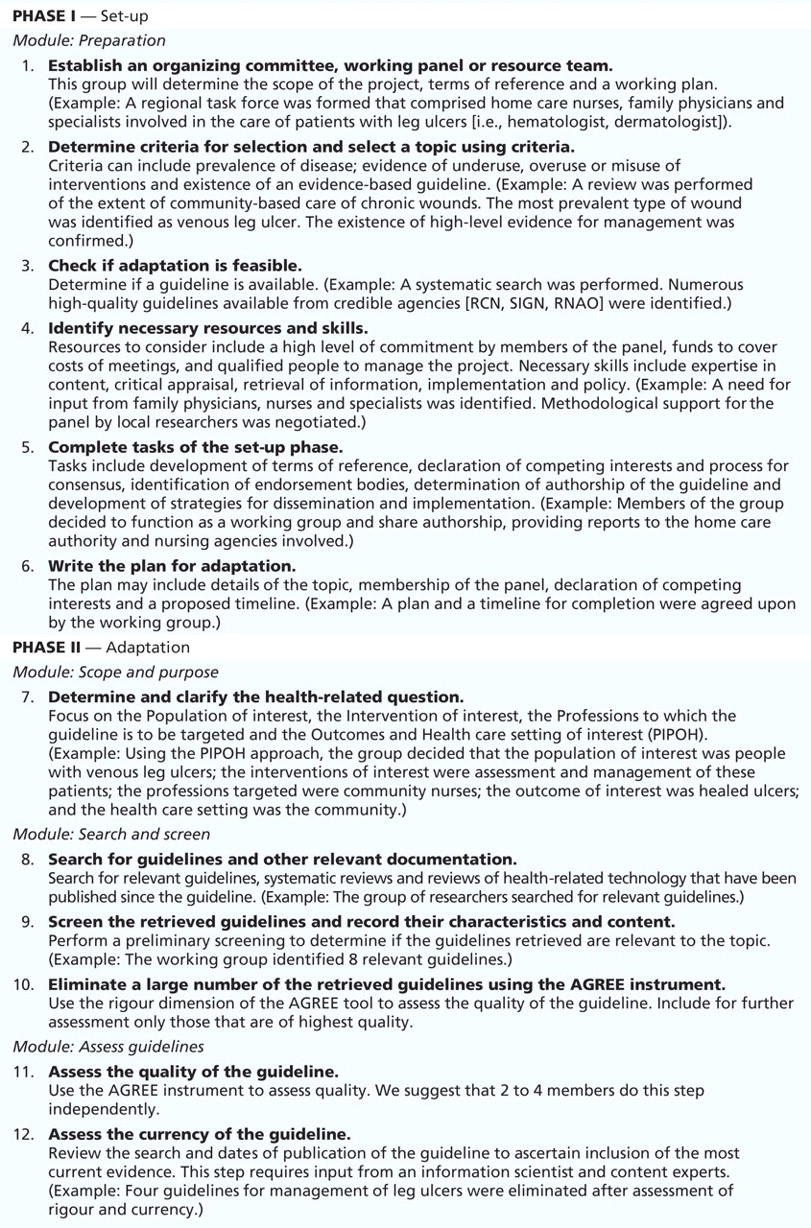
Box 1: Phases, modules and steps in the adaptation of a guideline using the ADAPTE process. A scenario of care of patients with leg ulcers is included as an example. (Part 1 of 2)

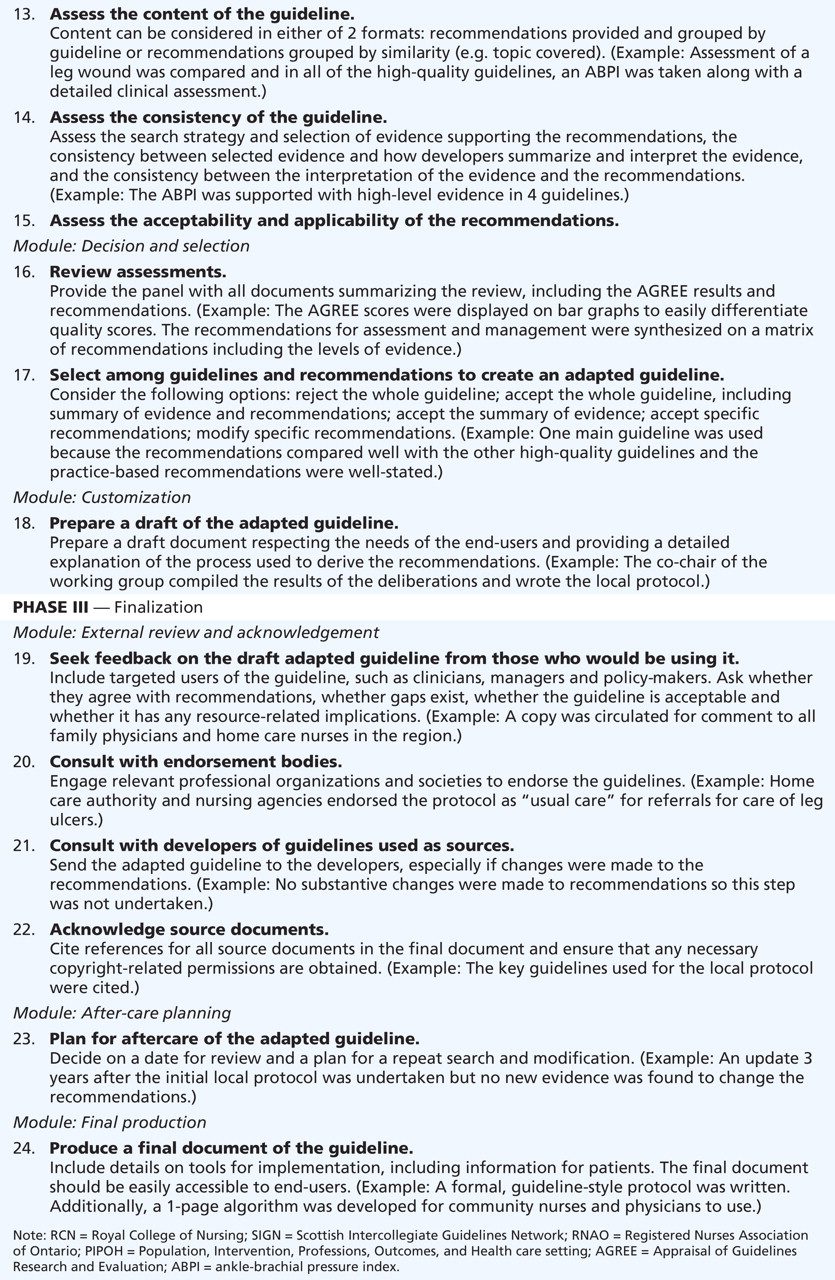
Box 1: Phases, modules and steps in the adaptation of a guideline using the ADAPTE process. A scenario of care of patients with leg ulcers is included as an example. (Part 2 of 2)
The phase of adaptation assists in moving from selection of a topic to identification of specific clinical questions; in searching for, retrieving and assessing guidelines; in decision-making around adaptation; and in preparing the draft version of the adapted guideline. Assessment of the retrieved guidelines involves evaluation of their quality (i.e., using the AGREE [Appraisal of Guidelines Research and Evaluation] instrument 9,23), currency (i.e., how up-to-date they are) and consistency (i.e., congruence of the recommendation with the underlying evidence). Assessment also consists of the examination of the acceptability (i.e., to clinicians and patients) and applicability (i.e., feasibility of applying recommendations) of the guidelines’ recommendations within the proposed context of use. This evaluation provides an explicit basis for informed and transparent decision-making around the selection and modification of guidelines used as sources. This process can result in different alternatives ranging from adopting a guideline unchanged, to translation of language and adaptation of format, to modification and updating of single recommendations, to the production of a customized guideline based on various guidelines used as sources. The finalization phase includes external review, feedback from relevant stakeholders, and consultation with the developers of source guidelines. Establishing a process for updating the adapted guideline and writing the final document are the last stages.
The ADAPTE process is supported by tools on the ADAPTE website, including a manual and toolkit. For each module, the manual provides a detailed description of the aims and tasks, the products and deliverables, and the skills and organizational requirements necessary to undertake the tasks. An example related to the adaptation of guidelines for screening for cervical cancer is provided throughout the modules. In the toolkit, 19 tools or instruments are offered to help structure the process and collect necessary information for decision-making.
For example, tool number 2 offers a comprehensive search strategy to help in identifying existing guidelines by searching websites of sources of guidelines (e.g., guideline-related clearing-houses, known developers’ sites, specialty organizations) and MEDLINE. Tool number 6 helps a group convert the topic of the guideline into a set of clear and focused key questions before the process of adaptation. Tool number 15 proposes a series of structured questions and criteria to guide the assessment of and discussion on whether a recommendation of a guideline is applicable or acceptable in the planned context of use and to identify the organizational changes that may be needed to deliver the recommendation. Steps and tools are flexible and have been designed to allow for alteration in the sequence in which they are used to fit with users’ time or restraints in resources.
Adapting a guideline or other tool of knowledge is a key component of the knowledge-to-action cycle. The adaptation process also integrates other steps of the cycle, including assessment of barriers to and facilitators of use of knowledge, which is necessary both for adapting and implementing the guideline.
Key concepts for assessment
The use of a framework is important for assessing barriers because it helps researchers and practitioners identify research questions, generate testable hypotheses, assess outcomes using valid and reliable instruments and make valid inferences from their results. A framework would ensure that researchers can elaborate theory-based interventions that have the potential for increasingly effective implementation of knowledge into clinical practice. 24 More importantly, the use of a framework also provides the foundation for the tools that help busy clinicians implement practice guidelines.
One of the more often-cited conceptual frameworks regarding barriers to use of knowledge in health care is the Clinical Practice Guidelines Framework for Improvement by Cabana and colleagues. 25 This framework was based on an extensive search of the literature for barriers to adherence by physicians to clinical practice guidelines and was organized according to knowledge, attitudes and behaviour of physicians. 26 Of 5658 potentially eligible articles, Cabana and colleagues identified 76 published studies describing at least one barrier to adherence to clinical practice guidelines. The included articles reported on a total of 293 potential barriers to adherence to guidelines by physicians. These barriers included unawareness of the existence of the guideline (n = 46), unfamiliarity with the recommendations of guidelines (n = 31), disagreement with the recommendations (n = 33), lack of self-efficacy (i.e., feeling one is unable to carry out the recommendations) (n = 19), outcome expectancy (i.e., the perception that health outcomes will be changed if the recommendations are followed) (n = 8), inability to overcome the inertia of previous practice (n = 14) and presence of external barriers to following the recommendations (n = 34). 25
Espeland and Baerheim 27 proposed a revised and extended classification of barriers based on the Clinical Practice Guide-lines Framework for Improvement. 27 They based their classification on interviews with focus groups of Norwegian general practitioners about factors affecting adherence to clinical practice guidelines for ordering diagnostic images for back pain. Newly identified barriers were lack of expectancy that adherence to guidelines will lead to the desired process of health care, emotional difficulty with adherence, improper access to actual or alternative health care services and pressure to do otherwise from health care providers and organizations. 27
More recently, the Clinical Practice Guidelines Framework for Improvement was expanded. In a study targeting the identification of barriers to and facilitators of implementing shared decision-making in clinical practice, each type of barrier was provided with a specific definition. 28 The intention was to standardize the reporting of barriers to and facilitators of use of knowledge in the context of health care. 28 Barriers were defined as factors that would limit or restrict implementation of shared decision-making in clinical practice. 29 More importantly, the Clinical Practice Guidelines Framework for Improvement was transferred into a list of potential facilitators of use of knowledge in clinical practice. 28 Facilitators were defined as factors that would promote or help implement shared decision-making in clinical practice.
Sometimes we forget that the same factor may sometimes be identified both as a barrier to and as a facilitator of use of knowledge, showing the importance of developing a more comprehensive and integrated understanding of both barriers and facilitators concurrently. 30,31 The Clinical Practice Guidelines Framework for Improvement was further extended to include the attributes of innovation as proposed by the Diffusion of Innovation theory. 32 As a result, except for the barrier known as lack of awareness (i.e., not knowing of the existence of a guideline) and the facilitator known as awareness (i.e., knowing about a guideline), the other factors initially proposed by the Clinical Practice Guidelines Framework for Improvement were potential barriers or facilitators. One new barrier, “forgetting” (i.e., inadvertently omitting to attend to something) was also identified.
This revised version of the Clinical Practice Guidelines Framework for Improvement was used in a systematic review of barriers to and facilitators of implementing shared decision-making in clinical practice. 33 The framework was applied successfully in extracting data from 41 publications covering 38 unique studies. 33 The corresponding definitions of each of the potential barriers to and facilitators of use of knowledge in the health care context are provided in Appendix 1 (available at www.cmaj.ca/cgi/content/full/cmaj.081232/DC1).
Tools for assessment
To clearly identify barriers to and facilitators of use of knowledge in health care practices, assessment of them in a valid and reliable fashion is needed. Considerable interest exists in the idea of instruments for valid and reliable assessment of barriers to and facilitators of use of knowledge that can be used by various end-users who are trying to implement knowledge. Based on the Clinical Practice Guidelines Framework for Improvement, a tool to assess barriers to adherence to guidelines for hand-specific hygiene was developed and tested on a group of 21 clinicians of infectious disease. 34 The tool uses a six-point Likert scale and has two sections: attitudinal statements about practice guidelines in general and specific statements regarding hand hygiene. The survey was administered twice, at two-week intervals. The tool known as Attitudes Regarding Practice Guidelines was found to have good reliability. 34 However, the authors concluded that their tool needed to undergo further testing and adaptation as a general measure of potential barriers to adherence to practice guidelines. 34
One of us (FL) completes regular audits of practice as part of a primary health care group. In a large, urban site for teaching family medicine (i.e., with 20 clinical teachers and 24 residents in family medicine as well as three nurses), the residents recently completed an audit of ambulatory care of patients with type 2 diabetes mellitus. One of the clinical teachers supervised a group of four residents in the completion of this audit. Residents reviewed the relevant practice guidelines and assessed their quality using the AGREE checklist. Based on this appraisal of quality, they retained the recommendations of the guidelines of the Canadian Diabetes Association. Based on these recommendations, they created a grid for extracting data on whether the recommendations were implemented. Forty patient charts were chosen randomly and the percentage of cases that followed the recommendations of guidelines was calculated.
The results of the audit were presented to the health care team for discussion. For example, results showed that a test for glycosylated hemoglobin was performed every three months, as recommended by the guidelines of the Canadian Diabetes Association (i.e., level D, consensus) in only 30% of cases. Based on the Clinical Practice Guidelines Framework for Improvement, discussion by the group revealed that barriers perceived by health care providers included lack of agreement with the recommendation because it was too rigid or artificial, factors associated with environment such as not having enough staff to carry out the recommendation, lack of agreement with the applicability of this recommendation to the population served by the practice based on the characteristics of the patient because some patients had very stable results in the past, and external factors, such as perceived inability to reconcile patient preferences with compliance to this recommendation.
This scenario shows that groups of providers in real clinical settings can take advantage of this checklist to identify barriers to carrying out recommendations in guidelines for practice. Once the barriers are made explicit, solutions can be expected to be brought forward for the benefit of patients. Without ignoring that one solution usually does not fit all, this checklist has the potential to help groups of providers reconcile their diverse perspectives because it is evidence-based, extensive and explicit.
Gaps in the implementation of evidence
Although many current research-based initiatives focus on implementing guidelines and assessing factors influencing use of knowledge in health care practices, many challenges remain that will need to be addressed by rigorous research. First, evaluation of the ADAPTE process is needed to determine its impact on the implementation of guidelines. Second, validated methods are needed to assess barriers to and facilitators of the translation of research into clinical practice. 29,35,36 Researchers and clinicians may want to consider using existing models that have been tested, such as the Clinical Practice Guidelines Framework for Improvement (i.e., in its latest version), to conduct studies on barriers to and facilitators of assessment. 25 Lastly, more will need to be done to reconcile the recommendations of practice guidelines to the sharing of care-related decisions with patients — the core concept of patient-centred care.
-
Clinical practice guidelines can be adapted to local circumstances and settings to avoid duplication of efforts and optimize use of resources.
-
The ADAPTE process is an approach to adapting guidelines to local contexts through the explicit participation of relevant decision-makers.
-
Assessing barriers to and facilitators of the use of knowledge is closely linked to the adaptation and uptake of the evidence.
Key points
Articles to date in this series
-
Straus SE, Tetroe J, Graham I. Defining knowledge translation. CMAJ 2009;181:165–8.
-
Brouwers M, Stacey D, O’Connor A. Knowledge creation: synthesis, tools and products. CMAJ 2009.DOI:10.1503/cmaj.081230
-
Kitson A, Straus SE. The knowledge-to-action cycle: identifying the gaps. CMAJ 2009.DOI:10.1503/cmaj.081231
Footnotes
-
ADAPTE Group
Melissa Brouwers, George Browman, Jako Burgers, Bernard Burnand, Margaret B. Harrison, Béatrice Fervers, Ian Graham, Jean Latreille, Najoua Mlika-Cabanne, Louise Paquet, Raghu Rajan, Magali Remy-Stockinger, Anita Simon, Joan Vlayen and Louise Zitzelsberger
This article has been peer reviewed.
Competing interests: None declared.
Contributors: Margaret Harrison, Béatrice Fervers and Ian Graham, who are founding members of the ADAPTE group, were involved in the development of the methodology of the manuscript, and conceptualized and drafted the section on adaptation of guidelines. France Légaré and Ian Graham were involved in the conceptualization and drafting of the section on assessment of barriers. All of the authors critically revised the manuscript and approved the final version submitted for publication.
Funding: No external funding was received for this paper.
The book Knowledge Translation in Health Care: Moving from Evidence to Practice, edited by Sharon Straus, Jacqueline Tetroe and Ian D. Graham and published by Wiley-Blackwell in 2009, includes the topics addressed in this series.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Translation of clinical practice guidelines on lifestyle behavior in a psychiatric setting. A discourse analytical case study
- A survey of UK nurses about their care of people with malignant fungating wounds
- Organisation of care for people receiving drug-resistant tuberculosis treatment in South Africa: a mixed methods study
- Secondary analysis of a James Lind Alliance priority setting partnership to facilitate knowledge translation in degenerative cervical myelopathy (DCM): insights from AO Spine RECODE-DCM
- neuroGPT-X: Towards an Accountable Expert Opinion Tool for Vestibular Schwannoma
- Adherence to clinical practice guidelines (CPGs) for the treatment of cancers in Australia and the factors associated with adherence: a systematic review protocol
- A unique framework for the Persian clinical guidelines: addressing an evidence-based CDSS development need
- Assessment of the methodological quality of local clinical practice guidelines on the identification and management of gestational diabetes
- Could implementation of mifepristone address Canadas urban-rural abortion access disparity: a mixed-methods implementation study protocol
- Factors hindering the adherence to clinical practice guideline for diabetes mellitus in the Palestinian primary healthcare clinics: a qualitative study
- How to adapt existing evidence-based clinical practice guidelines: a case example with smoking cessation guidelines in Canada
- Facilitation roles and characteristics associated with research use by healthcare professionals: a scoping review
- National and regional asthma programmes in Europe
- Guideline harmonization and implementation plan for the BETTER trial: Building on Existing Tools to Improve Chronic Disease Prevention and Screening in Family Practice
- Emerging Issues in Pharmacological Management of Rheumatoid Arthritis: Results of a National Needs Assessment Survey Identifying Practice Variations for the Development of Canadian Rheumatology Association Clinical Practice Recommendations
- Optimizing Nutrition in Intensive Care Units: Empowering Critical Care Nurses to Be Effective Agents of Change
- A guide to the translation of the Global Initiative for Asthma (GINA) strategy into improved care
- Rigour of development does not AGREE with recommendations in practice guidelines on the use of ice for acute ankle sprains
- Vitalizing Practice Through Research and Research Through Practice: The Outcomes of a Conference to Enhance the Delivery of Care
- Guideline adaptation: an approach to enhance efficiency in guideline development and improve utilisation
More in this TOC Section
Similar Articles

