


The 2002 guidelines for the management of osteoporosis published by Osteoporosis Canada 1 identified adequate vitamin D status, in addition to calcium from diet or supplements, as essential for the prevention of osteoporosis. Since then, our knowledge of the role of vitamin D (both D2 and D3) in fractures, falls and other health outcomes has expanded. Canadian recommendations for vitamin D, which are more than 10 years old, have never been supported by adequately conducted dose-finding studies 2 and were derived primarily from early nutritional science estimates of the minimal intake necessary to prevent extreme deficiency states.
We reviewed advances in knowledge about vitamin D physiology and optimal intake requirements for adults (except in pregnancy and during lactation) to update the 2002 clinical practice guidelines. In reviewing trials of vitamin D, it is important to remember that, unlike the situation for trials of pharmacologic agents, any reported benefits of vitamin D supplementation reflect correction of a deficiency in the population under study.
Methods
We systematically searched the MEDLINE database, for the period 1996 to June 30, 2008, and the Cochrane Library using the terms “vitamin D,” “vitamin D deficiency,” “25-hydroxyvitamin D,” “meta-analysis” and “systematic review.” We identified 168 potentially relevant papers. After removal of duplicates and screening of the abstracts by two reviewers (including A.C.), 16 relevant systematic reviews remained. We included systematic reviews of randomized controlled trials and observational studies that assessed the following outcomes: fractures, falls, death or extraskeletal outcomes. We used the Assessment of Multiple Systematic Reviews instrument 3 to evaluate the methodologic quality of reviews published after the cutoff date for literature reviewed in the 2002 guideline 1 until June 30, 2008 (see Appendices 1 and 2 of the full guideline, 4 available at www.cmaj.ca/cgi/content/full/cmaj.080663/DC1). For levels of evidence and grading of the recommendations, we followed the system used in the 2002 guidelines. 1 A multidisciplinary expert panel, including the authors of this article, reviewed the identified articles. As detailed in Table 1 of the full guideline, 4 we assigned a level of evidence to each summary point (from 1 = highest to 4 = lowest), and a grade to each recommendation, according to a system that incorporated both level of evidence and expert consensus (from A = highest to D = lowest). The Guidelines Committee and the Executive Committee of Osteoporosis Canada’s Scientific Advisory Council approved the recommendations.
Table 1: Classification of vitamin D status by serum level of 25-hydroxyvitamin D (25-OH-D)*
Assessment of vitamin D
Measurement and assay
After synthesis in the skin or ingestion through the diet, vitamin D3 is stored in the liver, adipose tissue and muscle, where it has a half-life of about 60 days. It is converted into 25-hydroxyvitamin D3 in the hepatocytes. 5–7 The serum concentration of 25-hydroxyvitamin D3 is the best indicator of the nutritional and functional status of vitamin D. 2 It is imperative that clinical laboratories measuring 25-hydroxyvitamin D3 participate in external proficiency testing. 8–10 Although circulating calcitriol (1α,25-dihydroxyvitamin D3 or 1,25-dihydroxycholecalciferol) is the vitamin D hormone regulating intestinal calcium and phosphate absorption, it is not an appropriate indicator of clinical vitamin D status in most cases. 5 The classification of vitamin D status is outlined in Table 1. Vitamin D2 (ergocalciferol) follows the same metabolic pathways as vitamin D3 but may have lesser activity 7.
Monitoring of serum 25-hydroxyvitamin D
For most Canadians, the recommendations for vitamin D supplementation outlined here should result in adequate blood levels, with no need for routine testing for vitamin D deficiency. However, in cases where deficiency is suspected (e.g., intestinal malabsorption states such as celiac disease) or where deficiency could affect the person’s response to other types of therapy (e.g., in osteoporosis requiring pharmacologic therapy), vitamin D deficiency should be ruled out by measurement of serum 25-hydroxyvitamin D.
The half-life of 25-hydroxyvitamin D in the body is 15–20 days. 6 With standard-dose supplementation, serum 25-hydroxyvitamin D plateaus after three to four months. 11 Therefore, to monitor a patient’s response, serum 25-hydroxyvitamin D should be measured no sooner than three months after treatment begins. After administration of high-dose oral or parenteral vitamin D replacement (e.g., 500 000 IU), the peak 25-hydroxyvitamin D level may be achieved in one month. 12
Factors associated with vitamin D deficiency
Many factors and conditions are associated with vitamin D deficiency. Some of these are causative (e.g., marked avoidance of ultraviolet radiation or malabsorption) and others are simply associated with decreased exposure to sunlight and poor nutrition (e.g., chronic illness or renal failure). 13,14
Sources of vitamin D
Exposure to the sun
The skin synthesizes vitamin D3 from 7-dehydrocholesterol in response to ultraviolet B radiation in sunlight. 15 This synthetic process depends on many factors, including latitude, altitude, time of year and day, weather, age, skin pigmentation type, clothing, activity and other aspects of the environment. Production of vitamin D in the skin falls to near zero for four to five months of the year in Canada, which raises the risk for vitamin D insufficiency or deficiency. 16–19
Food sources
The influence of the diet on vitamin D status is minimal, given the typical daily intake of 3.7–5.9 μg or 148–236 IU, 20 but it may be enough to prevent severe deficiency states, such as rickets. The few foods that naturally contain vitamin D (e.g., certain fish) are not consumed regularly. Consequently, Canadians depend on fortified dietary sources or supplements to maintain adequate vitamin D status.
Supplements
Serum 25-hydroxyvitamin D increases by 0.7–2.0 nmol/L for each 1 μg (40 IU) of vitamin D3 ingested daily. 11,21 For optimal vitamin D status, adult Canadians probably require vitamin D supplementation of 20–50 μg (800–2000 IU) daily. Doses over 50 μg (2000 IU) can be safely administered under medical supervision. 2 Treatment of severe deficiency (rickets or osteomalacia) requires higher doses, e.g., 1250 μg (50 000 IU) daily for two to four weeks, then weekly or biweekly, with monitoring of serum 25-hydroxyvitamin D at one and three months. These dosages are based on an assumption that the patient can absorb an orally administered dose. 5
Safety and toxicity of vitamin D supplementation
Excessive use of vitamin D supplements has the potential to cause progressive accumulation and toxic effects, presenting as hypercalcemia and renal damage. Canada’s “tolerable upper intake level” (the highest level of daily nutrient intake presenting no risk of adverse effects) is 50 μg (2000 IU) vitamin D for adults. 2 By definition, there is no need to monitor patients’ serum calcium or renal function unless doses above the tolerable upper level are administered. However, this level is undoubtedly too conservative and may eventually be revised upward, since toxic effects occur only with prolonged (at least several months) daily intake of more than 1000 μg (40 000 IU). 6,22
Traditional roles of vitamin D
Effect on bone mineral density
Low bone mineral density is a risk factor for osteoporotic fracture, and vitamin D deficiency is associated with low bone mineral density. 1 Observational studies have shown an association between higher serum 25-hydroxyvitamin D (range 40–90 nmol/L) and higher bone mineral density. 23–25 Randomized controlled trials have shown that vitamin D supplements significantly increase bone mineral density. 26–28
Effect on fractures
Observational studies have shown an association between low 25-hydroxyvitamin D and fractures. Clinical trials of vitamin D supplementation have been plagued by methodological issues: lack of determination of optimal dose, poor adherence, inadequate assessment of vitamin D status before or after supplementation and concurrent intervention with other osteoporosis therapies. However, it appears that 20 μg (800 IU) vitamin D3 given daily in combination with calcium reduces the risk of hip and nonvertebral fractures, especially for elderly patients living in institutions. 28–33
Effect on falls
Vitamin D may improve muscle strength and lower-extremity function, but the results of studies of fall prevention are inconsistent, because of differences in populations, doses and methods of capturing data on falls. 31,34–37 One meta-analysis suggested that vitamin D3 at a daily dose of 20 μg (800 IU) reduced the risk of falling, particularly in trials that adequately documented the ascertainment of falls. 38
Nontraditional roles of vitamin D
Calcitriol is produced locally from circulating 25-hydroxy-vitamin D in many tissues (e.g., skin, colon, prostate, breast, pancreas, heart and immune system), a process that is not regulated by serum calcium, phosphate or parathyroid hormone. 5 Many important physiologic actions of vitamin D outside the musculoskeletal system are now being explored. For example, vitamin D may have important antiproliferative and prodifferentiation properties. 5,39 Observational studies have shown a relationship between sufficient vitamin D status and lower risk of cancers. 40–42
Vitamin D may lower blood pressure by downregulating the production of renin. It may also stimulate the production and secretion of insulin and modulate immune function. 5 In epidemiologic studies, low circulating levels of vitamin D were associated with increased risk of multiple sclerosis. 43 Vitamin D–dependent processes affect macrophage lysis of Mycobacterium tuberculosis. 44 Epidemiologic studies have linked vitamin D deficiency in early life with later onset of diabetes mellitus. 45
The nontraditional actions of vitamin D have not been investigated to the same extent as its effects on mineral metabolism. There has been a paucity of intervention studies to test hypothesized benefits, and none of the studies to date used sufficient doses of vitamin D or were adequately powered. Systematic reviews or meta-analyses of the available literature are therefore unlikely to provide answers in this area. A prime example is the recently released, exhaustive report of the Agency for Healthcare Research and Quality, 33 a systematic review of the evidence for vitamin D affecting health outcomes. This review found little or weak evidence supporting the nontraditional actions of vitamin D and could make no recommendations other than that more research is needed.
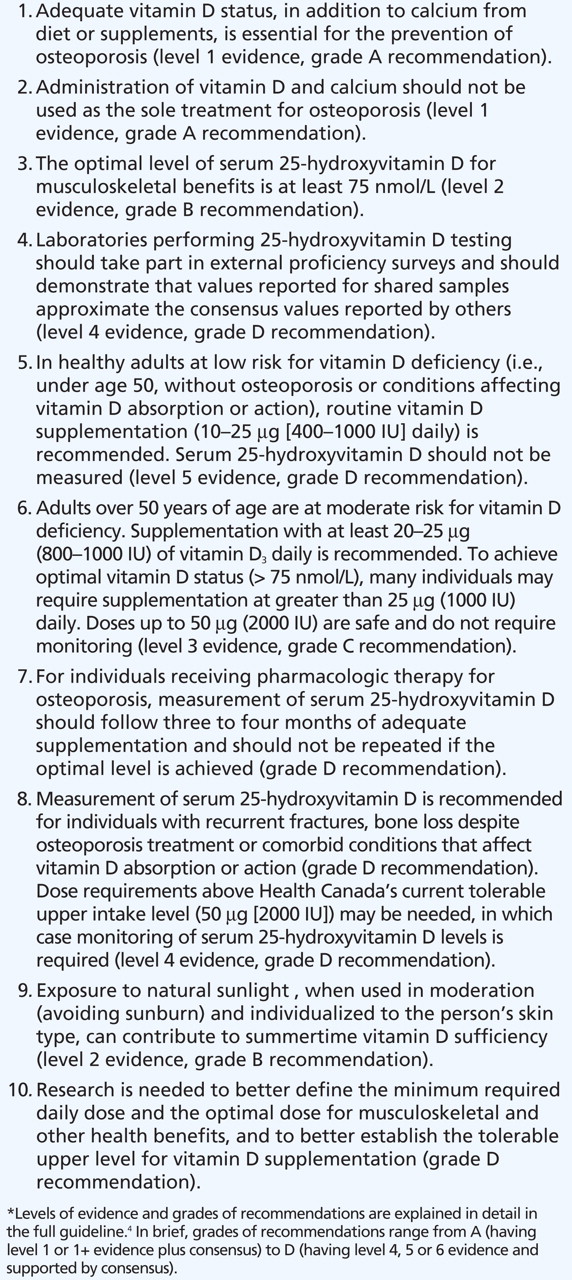
Summary statements about assessment of vitamin D levels, the safety of supplementation and the roles of vitamin D are presented in Box 1.

Box 1: Summary statements on vitamin D*
Approach to supplementation
Recommendations for vitamin D supplementation are outlined in Box 2. Given the limitations in our knowledge of optimal intake levels, evidence of the safety and potential benefits of vitamin D supplementation support recommendations aiming for serum 25-hydroxyvitamin D levels above 75 nmol/L. For most Canadian adults, exposure to sunlight and dietary intake are insufficient to maintain this level through-out the year, and vitamin D supplementation is therefore indicated. 17–19 The clinical approach can take into account three “settings,” which are based on suspicion for vitamin D insufficiency and its complications. The three settings are low risk for vitamin D deficiency, moderate risk for deficiency and receipt of pharmacologic therapy for osteoporosis.

Box 2: Recommendations for vitamin D supplementation*
Vitamin D3 is the preferred supplementary form for humans, with vitamin D2 being available for large-dose preparations. Calcitriol and its analogues are prescription products with narrow margins of safety and are not advised for the prevention or treatment of osteoporosis. For most adults, a vitamin D3 supplement at an initial daily dose of at least 20 μg (800 IU) is appropriate. This dose is unlikely to raise the average serum 25-hydroxyvitamin D level by more than 20 nmol/L. 11,21 To achieve desirable vitamin D status (> 75 nmol/L), many individuals will require higher doses.
Because vitamin D is stored in body tissues, a larger, less frequent dose may be preferred by some patients. A weekly dose of 250 μg (10 000 IU) vitamin D3 is available by prescription in some provinces. Some practitioners prescribe vitamin D2 at a dose of 1250 μg (50 000 IU) monthly.
Knowledge gaps
There is need for research to better define the minimum required dose and optimal daily dose for musculoskeletal and other health benefits, as well as the tolerable upper intake level for vitamin D. There is also a need for randomized controlled trials to clarify the benefits and risks (if any) of vitamin D supplementation at that optimal dose. The purported benefits of vitamin D beyond musculoskeletal disorders should be confirmed in clinical trials.
-
Vitamin D is essential for the prevention of osteoporosis.
-
A serum level of 25-hydroxyvitamin D above 75 nmol/L reflects optimal vitamin D intake or synthesis to consistently improve clinical outcomes such as fracture risk; vitamin D supplementation is needed to achieve this target.
-
Recommended intake for low-risk and younger adults should be increased to 10–25 μg (400–1000 IU) daily and for high-risk and older adults, to 20–50 μg (800–2000 IU) daily, with consideration of higher doses (key change from 2002 guideline).
-
For individuals being treated with pharmacologic agents for osteoporosis, vitamin D status should be assessed by serum measurement of 25-hydroxyvitamin D after three months of vitamin D supplementation (key change from 2002 guideline).
Key points
Footnotes
-
Previously published at www.cmaj.ca
See also the complete guideline article by Hanley and colleagues at www.cmaj.ca
This article has been peer reviewed.
Competing interests: All authors were members of the Vitamin D Working Group of Osteoporosis Canada. David A. Hanley has been an investigator in clinical trials, participated in advisory boards or received speaking honoraria from the following companies: Amgen, Merck Frosst Canada, Proctor and Gamble Canada (now Warner-Chilcott), sanofi-aventis, Novartis, NPS Pharmaceuticals, Eli Lilly Canada, Pfizer, Wyeth-Ayerst, Roche, Servier, Abbott Laboratories and Nycomed. Glenville Jones serves on the scientific advisory board of the not-for-profit Vitamin D External Quality Assessment Scheme. He is also on the advisory board and has received a research grant from Cytochroma Inc. and is a member of the Genzyme speakers’ bureau. Susan J. Whiting is a member of the International Institute for Nutrition and Bone Health, an educational initiative sponsored by Yoplait. She has received current or recent funding in the form of grants and contracts from the Canadian Institutes of Health Research and the Canadian Foundation for Dietetic Research. She is a nutrition consultant to Osteoporosis Canada. She has presented talks with sponsorship from the Dairy Farmers of Canada, the International Alliance of Dietary/Food Supplement Associations, the Vitamin D Society, GlaxoSmithKline and Amway/Nutrilite. William D. Leslie has received speaker fees and unrestricted research grants from Merck Frosst Canada Ltd; unrestricted research grants from sanofi-aventis, Procter and Gamble Pharmaceuticals Canada, Novartis, Amgen Pharmaceuticals Canada and Genzyme Canada; and has served on advisory boards for Genzyme Canada, Novartis and Amgen Pharmaceuticals Canada. None declared for Ann Cranney.
Contributors: All authors, as well as the other members of the Vitamin D Working Group (listed in the Acknowledgments section), participated in the conception and design of the vitamin D guideline project. David A. Hanley oversaw the writing project, recruited committee members, and edited and revised all section submissions. Ann Cranney wrote the Methods section and the section entitled “Traditional roles of vitamin D” and was one of the reviewers of the abstracts identified in the literature search. Glenville Jones wrote the section entitled “Assessment of vitamin D,” Susan J. Whiting wrote the section entitled “Sources of vitamin D” and William D. Leslie wrote the section entitled “Nontraditional roles of vitamin D.” All authors contributed to the review and revision of the entire manuscript, and all authors approved the final version submitted for publication.
Funding: Osteoporosis Canada received a grant from the Ontario Ministry of Health and Long-Term Care to develop these guidelines as a part of a larger project to develop guidelines for the investigation and management of osteoporosis.
Endorsements: Canadian Society of Clinical Chemists, Canadian Association of Nuclear Medicine, Canadian Geriatrics Society, Canadian Orthopaedic Association, Canadian Society of Endocrinology and Metabolism, Dietitians of Canada, Ontario Association of Radiologists, Society of Obstetricians and Gynaecologists of Canada, Canadian Rheumatology Association, Canadian Pharmacists Association and Ontario College of Family Physicians.
Acknowledgements: The other members of the Vitamin D Working Group of Osteoporosis Canada, who made important contributions to this document, were Drs. David E. C. Cole, Stephanie A. Atkinson, Robert G. Josse, Sidney Feldman, Gregory A. Kline and Cheryl Rosen. The document was reviewed and approved by the Guidelines Committee of the Scientific Advisory Council of Osteoporosis Canada (chaired by William D. Leslie ): Angela Cheung, Kerry Siminoski, Alexandra Papaioannou, Sophie Jamal, Anthony Hodsman and Jacques Brown. The assistance of Loretta Hillier in condensing the original version of the manuscript and collating the references was much appreciated.
This article is a summary of a full review and guideline of vitamin D in adult health and disease (available online at www.cmaj.ca) prepared by a committe of authors chosen by the Guidelines Committee of the Scientific Advisory Council of Osteoporosis Canada. The guideline is an update of the vitamin D section of the complete osteoporosis clinical practice guidelines of Osteoporosis Canada, published in 2002.
REFERENCES
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Vitamin D deficiency or supplementation and the risk of human herpesvirus infections or reactivation: a systematic review protocol
- Vitamin D status among adults (18-65 years old) attending primary healthcare centres in Qatar: a cross-sectional analysis of the Electronic Medical Records for the year 2017
- Use of vitamin D drops leading to kidney failure in a 54-year-old man
- Prescribing and testing by primary care providers to assess adherence to the Choosing Wisely Canada recommendations: a retrospective cohort study
- The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases
- Vitamin D status of refugees arriving in Canada: Findings from the Calgary Refugee Health Program
- Preventing fractures in postmenopausal women: how to assess risk
- Vitamin D and Cardiovascular Disease: Time for Large Randomized Trials
- 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary
- Should I prescribe sunlight instead of vitamin D?
- Vitamin D for mental health and cognition
- A step in the right direction
More in this TOC Section
Similar Articles
Collections

