


A five-year-old girl with sickle cell disease presented with a two-day history of left frontal headache and mild fever. There were no signs of toxicity, and the patient was hemodynamically stable. Her rectal temperature was 39.5°C. Marked nuchal rigidity was noted. Palpation of the dorsal vertebrae caused mild pain. There were no focal neurologic signs. The patient had been admitted to hospital several times for episodes of fever associated with pneumonia and urinary tract infections, but she had no history of vaso-occlusive crisis.
Laboratory tests showed a hemoglobin level of 51 (normal 115–135) g/L, a leukocyte count of 19.4 (normal 5.5–15.5) ×109/L, and a neutrophil count of 13.9 (normal 1.5–7.1) × 109/L. Cerebrospinal fluid obtained by lumbar puncture yielded a leukocyte count of 2.0, a erythrocyte count of 1.0 × 106 /L and normal levels of glucose and protein.
Morphine was prescribed and, despite the absence of a specific cause of the fever, treatment with intravenous ceftriaxone was started, pending results of cultures. Over the next four to six hours, a nonpainful pitting edema was seen in the left palpebral and frontoparietal regions. There was no proptosis, and the ocular movements were normal. The skin was not red or warm over the edematous zone.
What is the next step?
-
Computed tomography scan of the brain
-
Diagnostic puncture of the swollen region
-
Radiography of the sinuses
-
Doppler ultrasonography of the cervical vessels
-
Bone scintigraphy
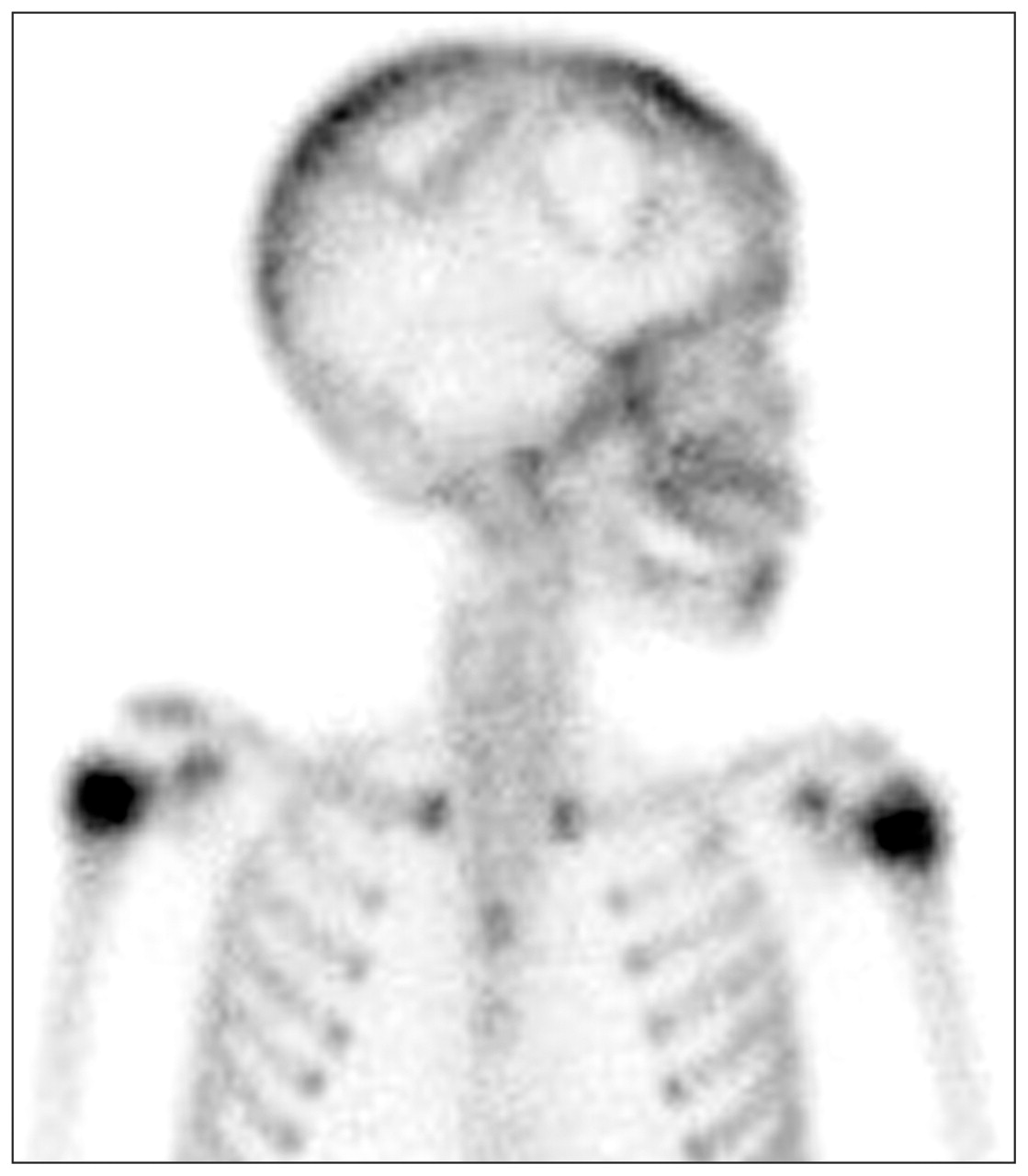
Tests (a) and (e) were performed. A computerized tomography scan of the brain showed normal parenchyma, but there was an infiltration of the subcutaneous fat of the left hemiface extending into the subcutaneous tissue of the left occipital and parietal regions (Figure 1). Bone scintigraphy of the cranial vault showed areas of decreased activity in the frontal and parietal bones compatible with infarcts (Figure 2). Bone scintigraphy of the spine showed decreased activity in the region of T5 and possibly T8.

Figure 1: Computerized tomography scan of the brain in a five-year-old girl with sickle cell disease showing infiltration of the subcutaneous fat of the left hemiface extending into the left occipital and parietal regions (arrow).

Figure 2: Bone scintigraphy of the cranial vault showing decreased activity in the frontal and parietal bones compatible with infarcts.
What is your diagnosis?
-
Cervical spine osteomyelitis
-
Peri-orbital cellulitis
-
Cerebral sinovenous thrombosis
-
Bacterial meningitis
-
Vaso-occlusive crisis of the cranial vault and dorsal spine
The diagnosis is (e), vaso-occlusive crisis of the cranial vault and dorsal spine. The child received a transfusion of packed red blood cells. Narcotics were given to control pain, and ceftriaxone was continued until the fever disappeared. Bacterial cultures of cerebrospinal fluid and blood gave negative results. The nuchal rigidity and fever resolved gradually over seven days. The swelling of the left side of the face had disappeared by the patient’s eighth day in hospital. On the ninth day, radiography of the skull showed thickening of the cranial vault related to sickle cell disease but was otherwise normal. The child was discharged from hospital 10 days after admission.
Discussion
Sickle cell disease results from the presence of abnormal β chains in hemoglobin. It is one of the most common autosomal recessive diseases, affecting millions of people in West and Central Africa, South America, Central America, India and Mediterranean countries. The gene that causes the disease is particularly prevalent in people of African origin. Approximately 8% of African-American people are heterozygous and 1 in 600 is homozygous for the gene. Although reliable data for Canada are scarce, it is estimated that 2000 to 3000 children in this country have sickle cell disease.
Acute painful episodes from vaso-occlusive crises are the most common manifestations of sickle cell disease; they occur most frequently in the lumbar spine, abdomen, femur, knees and sternum 1 but can affect any bone with active marrow. Dactylitis, often referred to as hand–foot syndrome, is often the first manifestation of vaso-occlusive crisis in children with sickle cell disease, occurring in 50% of children before two years of age. The vulnerability of the bone marrow to microvascular occlusion may be due to the anatomically confined space and hypercellularity of the marrow. Flat bones are less commonly infarcted, probably because of their many nutrient vessels. 2
Acute infarction of the skull bone (calvarial infarction) is an uncommon complication of sickle cell disease. It could involve the cranial vault, as in our patient, but also the facial bones and orbits. 3 Headache related to calvarial infarction may originate from pain-sensitive structures such as the skull, dura, periosteum and extracranial arteries. 4 Local meningeal inflammation can cause meningismus. The infarction may also be associated with pitting scalp edema. 4 In our patient, the infiltration of the subcutaneous fat over the left hemiface was found to be edema of the subcutaneous tissue caused by the infarction. Bone infarction is self-limiting, and only conservative treatment is usually required. However, infarctions at these sites may cause subperiosteal or epidural hematomas or even abscesses, 3 complications that can be life- or sight-threatening and may require urgent decompression. 3
The spine is the area most commonly involved in vaso-occlusive crisis. 5 The lumbosacral level is affected in two-thirds of patients, and the thoracic level in approximately 20%. 5 Signs of spinal vaso-occlusive crisis — mostly local tenderness and a decreased range of motion in the spine —have been reported only in small series. 5 That infarctions of the cranial vault and the thoracic spine were observed simultaneously in our patient is not surprising; in the classic description of vaso-occlusive crisis by Serjeant and colleagues, multiple sites of bone infarction occur in 79% of patients. 1 Indeed, in a patient with sickle cell disease, the presence of many sites of pain reinforces the possibility of vaso-occlusive crisis rather than a primary infectious process.
Diagnostic testing
Radiologic techniques may be helpful in patients for whom the diagnosis is in question or when it seems necessary to exclude infectious processes. A bone scan may show the three-stage process that occurs in infarction. 6 Variability of the scan images depends on the interval between the onset of symptoms and the time of the scan. 6 Stage 1 (about 48 hours after onset of symptoms), shows decreased tracer activity in the area of the infarction; stage 2 (about 1 week after onset) shows normal uptake; and stage 3 (2–4 weeks after onset) shows increased uptake. A bone marrow scan or magnetic resonance imaging may be more sensitive in identifying bone infarction, 6 but in most instances a bone scan is sufficient.
Differential diagnosis
The two prominent clinical manifestations in our patient were marked nuchal rigidity and facial edema.
In a child with fever, nuchal rigidity is of concern, and meningitis must be ruled out. However, stiffness of the neck is not necessarily the result of meningeal infection, as was the case in our patient. Some extrameningeal infections (e.g., tonsillopharyngitis, cervical adenitis, retropharyngeal abscess and cervical spine osteomyelitis) may also cause neck stiffness (Box 1). In a child with fever, sickle cell disease, neck stiffness and normal cerebrospinal fluid, these infections must be excluded promptly. Indeed, children with sickle cell disease, mostly those under five years of age, are at higher risk of bacterial infection, which is one of the major causes of illness and death in this population. 7 All patients with fever and sickle cell disease require rapid triage, urgent blood cultures, and analysis of cerebrospinal fluid and other cultures as required (Box 2). 8

Box 1: Differential diagnosis of nuchal rigidity in children with sickle cell anemia*

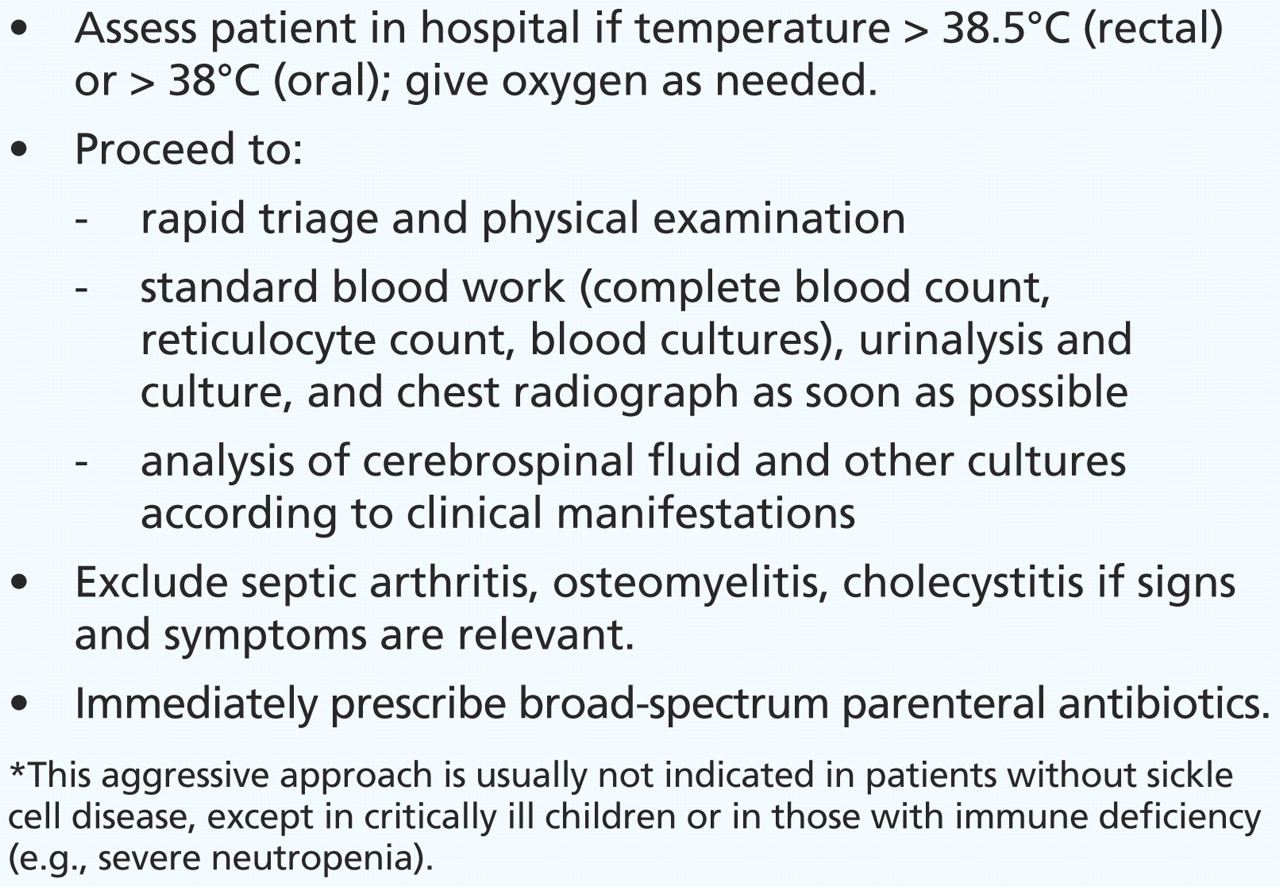
Box 2: Management of acute febrile illness in a child with sickle cell disease*
In our patient, physical examination showed no evidence of tonsillopharyngitis or cervical adenitis. She was not complaining of sore throat or difficulty in swallowing, which suggested that a retro- or parapharyngeal infection was unlikely. Cervical spine osteomyelitis could not explain the facial edema, and the bone scan images did not support this diagnosis.
Local trauma to the orbits, the facial bones or the skull is a major cause of facial edema (Box 3); in almost all instances, the traumatic nature of the lesions is obvious. There was no history of trauma in our patient. The child was an unlikely candidate for periorbital or orbital cellulitis; she presented with hemiface edema, predominantly on the scalp and not in the periorbital region, and the results of ocular examination were normal. Acute sinusitis can cause periorbital edema, but not edema in the parietal region, as in our patient. Hemiface edema is not a usual clinical manifestation of cerebral sinovenous thrombosis. Angioneurotic edema is usually bilateral and symmetric, and typically involves sites other than the face: the arms, legs, hands, tongue, larynx, genitalia and trunk.
Box 3: Differential diagnosis of facial edema in children with sickle cell anemia*
In our patient, the diagnosis was infarction of the cranial vault associated with vaso-occlusive crisis. Bone infarction of the cranial vault is a specific manifestation of sickle cell disease and may lead to an uncommon clinical presentation characterized by fever, neck stiffness and hemiface edema. In retrospect, the fact that our patient showed no signs of toxicity and was hemodynamically stable, despite the fever and nuchal rigidity, could have been an element in favour of a vaso-occlusive crisis. Nonetheless, it is important for clinicians to remember that vaso-occlusive crisis of the cranial vault is very uncommon. It is always a priority to exclude meningitis or other serious extrameningeal infections in a child with fever and nuchal rigidity.
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: None declared.
CMAJ invites submissions to “What is your call?” Clinical details (including images) are presented on the first page along with a multiple-choice question about the diagnosis. The answer and a brief discussion of the condition follow on the second page. We specifically invite submissions illustrating common or important radiographic and electrocardiographic diagnoses of appeal to a general audience. We allow up to five references and require authors to obtain consent from the patient for publication of his or her story (form available at www.cmaj.ca/authors/checklist.shtml). Submit manuscripts online at http://mc.manuscriptcentral.com/cmaj.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

