


- © 2007 Canadian Medical Association
The case: A 37-year-old woman with a history of psoriasis and ulcerative proctitis presented to the hospital with blistering skin lesions on her lower legs. The patient had been in remission from presumed ulcerative colitis for 4 years and was taking mesalamine (500-mg suppository at bedtime). Two months before presentation, she had started experiencing intermittent nausea that was attributed to pregnancy. Two weeks before presentation, she underwent dilation and curettage after fetal demise at 12 weeks' gestation. The day after this operation red welts began to develop below her right patella. Within a week, several other papules had formed over both knees and anterior tibiae. These turned into blisters, 1 of which started releasing purulent fluid.
In the emergency department, naproxen therapy was started for what was considered to be a possible vasculitic process, and the patient was discharged home with outpatient follow-up. That evening, a nonproductive cough developed, which was exacerbated when she lay down and when she breathed deeply. Over the next 3 days, she experienced progressively worsening wheezing and dyspnea, to the point where she could not work and was no longer able to sleep in a supine position. She also developed pain and swelling in her hands, right elbow and left foot.
On the day she was admitted to hospital, the patient was dyspneic (oxygen saturation of 95% on room air). Her mouth revealed multiple aphthous ulcers. She was intermittently stridorous, and auscultation revealed marked bilateral inspiratory and expiratory wheezing. Abdominal examination yielded normal findings, and the patient reported normal bowel movements. Her blistering, tender, purpuric peripatellar lesions oozed yellowish fluid. Examination of her joints revealed a swollen right elbow that was restricted to 150° extension. She had erythematous swelling and tenderness in the fourth proximal interphalangeal joint of her right hand and the third distal interphalangeal and first metatarsophalangeal joints of her left hand. Treatment with nebulized salbutamol and ipratropium was started, but with minimal response.
Blood tests revealed leukocytosis (leukocyte count 12.9 [normal 4.5– 10.0] × 109/L; neutrophil count 11 × 109/L), mild normocytic anemia (hemoglobin concentration 109 g/L; mean corpuscular volume 85 fL) and thrombocytosis (platelet count 833 [normal 150– 400] × 109/L). Tests of the patient's immune system revealed an elevated erythrocyte sedimentation rate of 94 mm/h, a C-reactive protein level of 103.8 mg/L, a rheumatoid factor of 26 IU/mL, normal C3 and C4 concentrations, normal serum angiotensin-converting enzyme levels, an antinuclear antibody titer of 1:160 and the presence of antineutrophil cytoplasmic antibodies with an atypical perinuclear (p-ANCA) pattern. Results of tests for antiglomerular basement membrane, anticardiolipin and antistreptolysin O antibodies were negative. Results of serologic testing for hepatitis B and C viruses, HIV and cytomegalovirus were also negative.
Table 1.
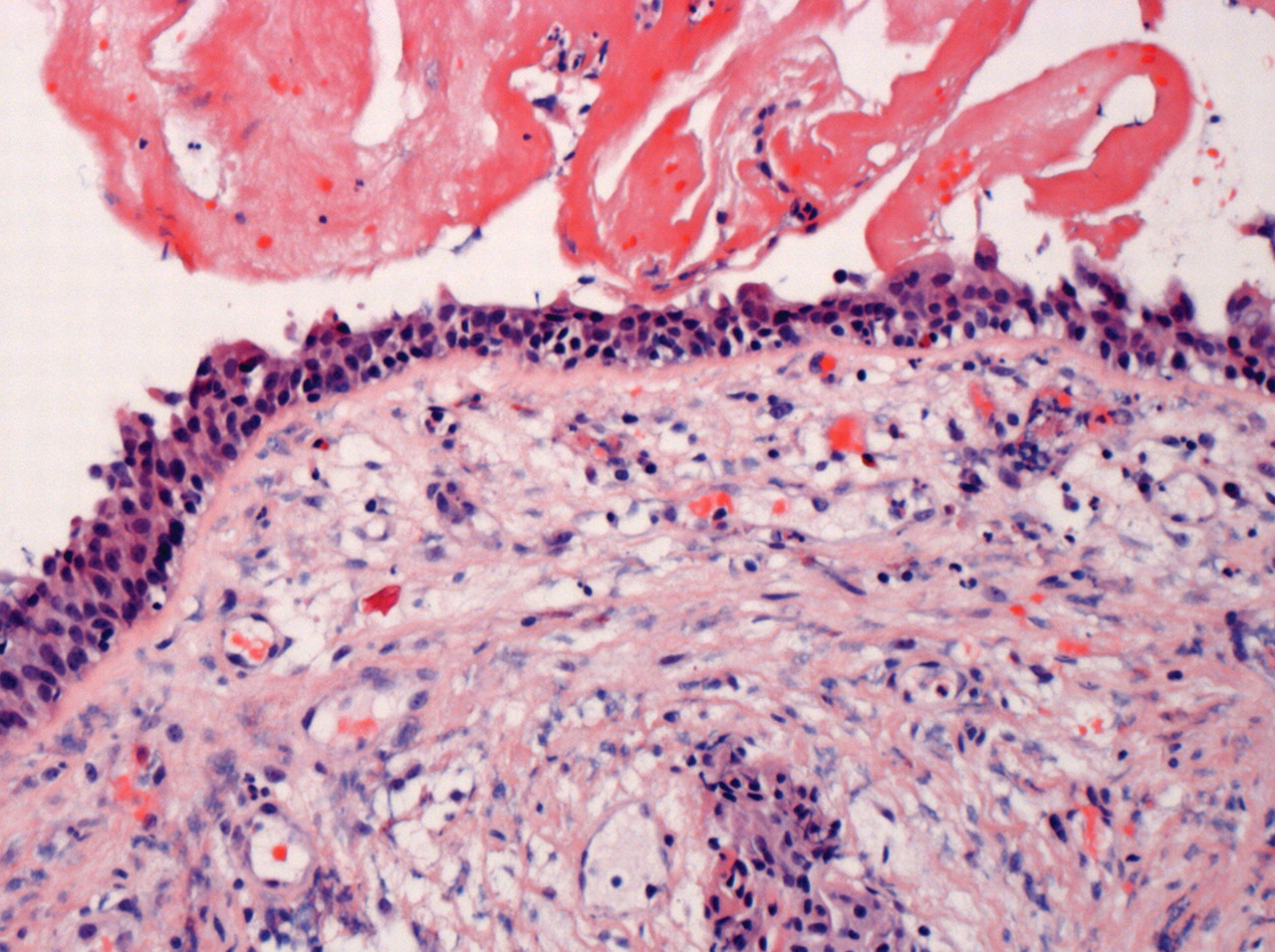
Chest radiography on the day of admission showed collapse of the left upper lobe of the lung (Figure 1). At the time, our differential diagnosis included a pulmonary process associated with pyoderma gangrenosum, sulfasalazine pneumonitis, Wegener's granulomatosis and sarcoidosis. Alternative possibilities to consider were Sweet's syndrome, tracheal tuberculosis and other infectious causes. Sulfasalazine pneumonitis seemed unlikely given the concurrent pyoderma gangrenosum and polyarthritis. Pulmonary function tests showed a ratio of forced expiratory volume in the first second to forced vital capacity of 36% (Table 1) with a biphasic flattening of the flow– volume curve (Figure 2), which indicated fixed upper-airway obstruction with no improvement after use of a bronchodilator. No upper-airway obstruction or abnormal vocal cord movement was seen on laryngoscopy. Bronchoscopy revealed edematous, glistening white nodular bronchial mucosa on an erythematous background (Figure 3, Figure 4 and Figure 5) with distal tracheal stenosis, narrowing of the left main bronchus and near total occlusion of the left upper-lobe orifice. Bronchoalveolar lavage confirmed the presence of reactive endobronchial cells but analysis yielded negative results for tuberculosis, fungi and bacteria. Biopsy of the endobronchial lesions revealed mild to moderate chronic nonspecific inflammation (Figure 6), similar to that found in a skin biopsy of the lower leg lesions, which were interpreted as pyoderma gangrenosum. Computed tomography of the thorax revealed an infiltrative process involving the trachea, left main bronchus and left upper-lobe bronchus. Several mediastinal lymph nodes and a moderate-sized pericardial effusion were visualized.

Figure 1: Chest radiograph showing collapse of left upper lobe (arrow).
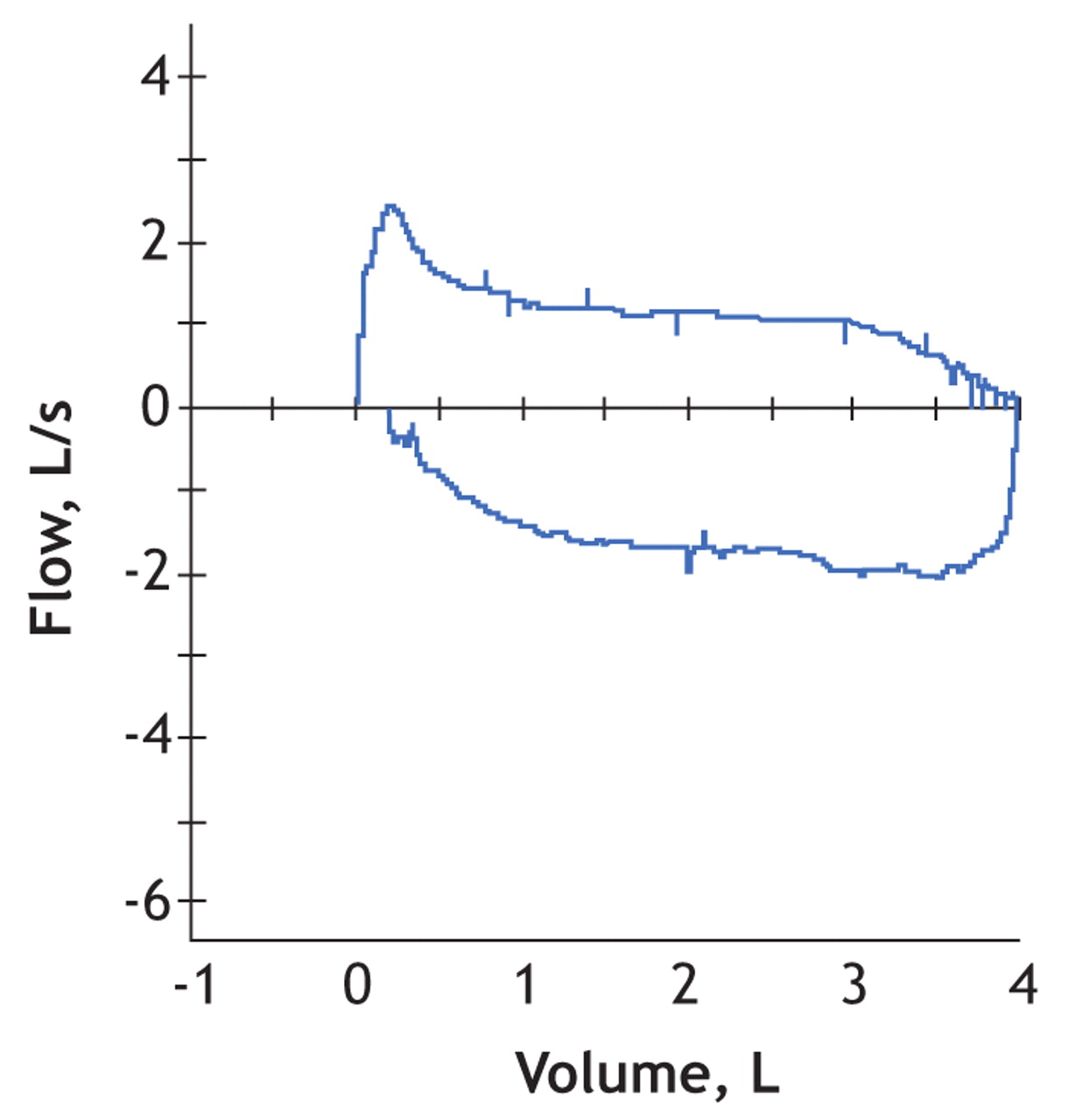
Figure 2: Flattening of flow–volume loop, indicating fixed upper-airway obstruction on admission.

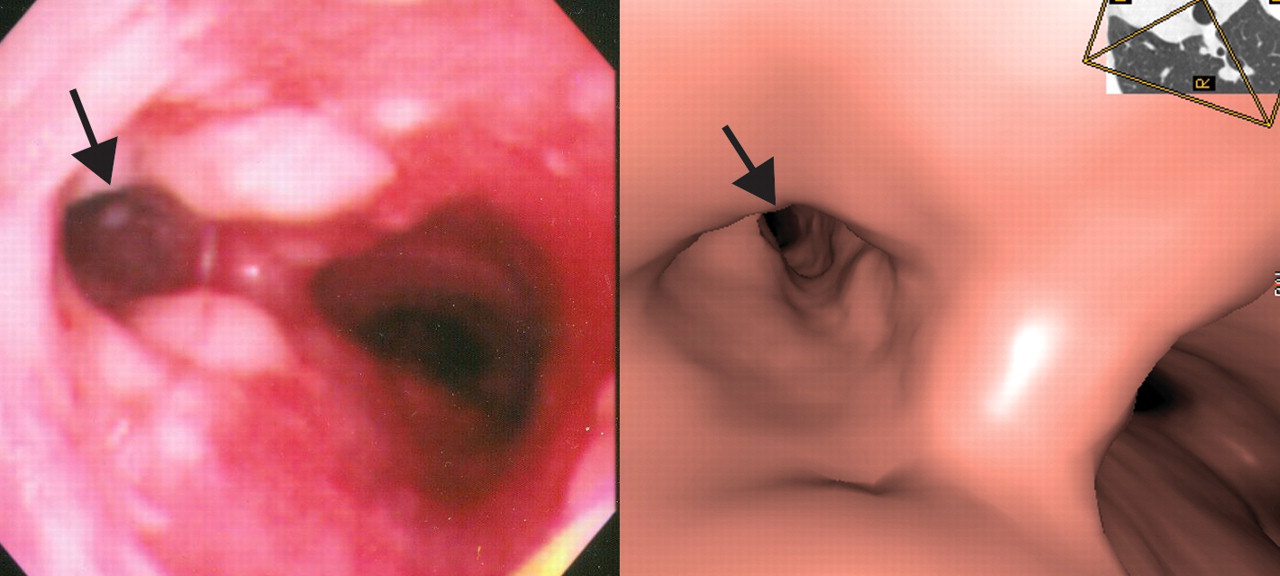
Figure 3: Distal tracheal stenosis with nodularity and ulceration on bronchoscopy (left) and virtual bronchoscopy (right).

Figure 4: View of carina showing stenosis of left main bronchus (arrows) on bronchoscopy (left) and virtual bronchoscopy (right).

Figure 5: Near-occlusion of left upper-lobe bronchus (arrows) on bronchoscopy (left) and virtual bronchoscopy (right).

Figure 6: Medium-power light micrograph of tracheal surface showing epithelium adjacent to fibrinous exudate (top) and inflammation in underlying lamina propria (hematoxylin–eosin stain, original magnification × 100).
High-dose intravenous steroid therapy was begun, and the mesalamine therapy was stopped. Because of significant improvement in the patient's respiratory symptoms, on day 2 she was switched to oral steroid therapy. However, on day 4 of steroid therapy, the patient began to pass copious amounts of bloody, loose stool. Colonoscopy demonstrated severe active colitis involving mainly the right colon and sparing the distal sigmoid colon and rectum. The endoscopic appearance was compatible with Crohn's disease, with aphthous ulcers, cobblestoning and discontinuous lesions. The pathology was consistent with chronic idiopathic inflammatory bowel disease with no granulomas or dysplasia present (Figure 7, left panel); a micrograph of the near-normal area of the colon specimen is provided for comparison (Figure 7, right panel). Prednisone was continued. After 5 weeks of steroid therapy, results of pulmonary function tests showed residual mild airflow obstruction at the level of the small airways. Over 3 months prednisone was gradually tapered, and there was complete resolution of the patient's respiratory, rheumatologic, dermatologic and gastrointestinal symptoms. Oral mesalamine therapy was then initiated. The patient remained free of symptoms until 7 months later, when she again became pregnant and diarrhea recurred at 6 weeks' gestation. The mesalamine dose was increased from 2 g/d to 3 g/d, and the diarrhea resolved.

Figure 7: Medium-power light micrographs of colonic mucosa. Left: Mucosa from inflamed area of colon biopsy specimen, showing prominent lymphoplasmacytic infiltrate and glands containing neutrophils (crypt abscess) (hematoxylin–eosin stain, original magnification × 100). Right: Mucosa in near-normal– appearing area of colon biopsy specimen, showing sparse lymphoplasmacytic infiltrate in lamina propria and intact glands (hematoxylin–eosin stain, original magnification × 100).
This patient presented with a unique constellation of symptoms involving 4 systems: wheezing and stridor caused by tracheobronchitis, pyoderma gangrenosum skin lesions, polyarthritis and diarrhea due to exacerbation of inflammatory bowel disease. Tracheobronchial stenosis has been reported in patients with Crohn's disease,1–5 and pyoderma gangrenosum in association with tracheobronchitis has been documented in a patient without inflammatory bowel disease.6 However, this case is distinctive in that respiratory, dermatologic, rheumatologic and gastrointestinal manifestations followed a parallel clinical course. These symptoms occurred in the context of fetal loss. Active inflammatory bowel disease at the time of conception and during pregnancy has been significantly associated with fetal loss or preterm delivery. Another interesting feature of this case is that, although our patient had previously received a diagnosis of ulcerative proctitis, her current endoscopic appearance supported Crohn's disease. Pathologic investigation did not show granulomas, which are highly suggestive of Crohn's disease; however, they are present in only about 20% of biopsy specimens from patients with the disease. In recent years, the typical rectal-sparing nature of Crohn's disease has been challenged in that 10% of cases have been found to involve the rectum.
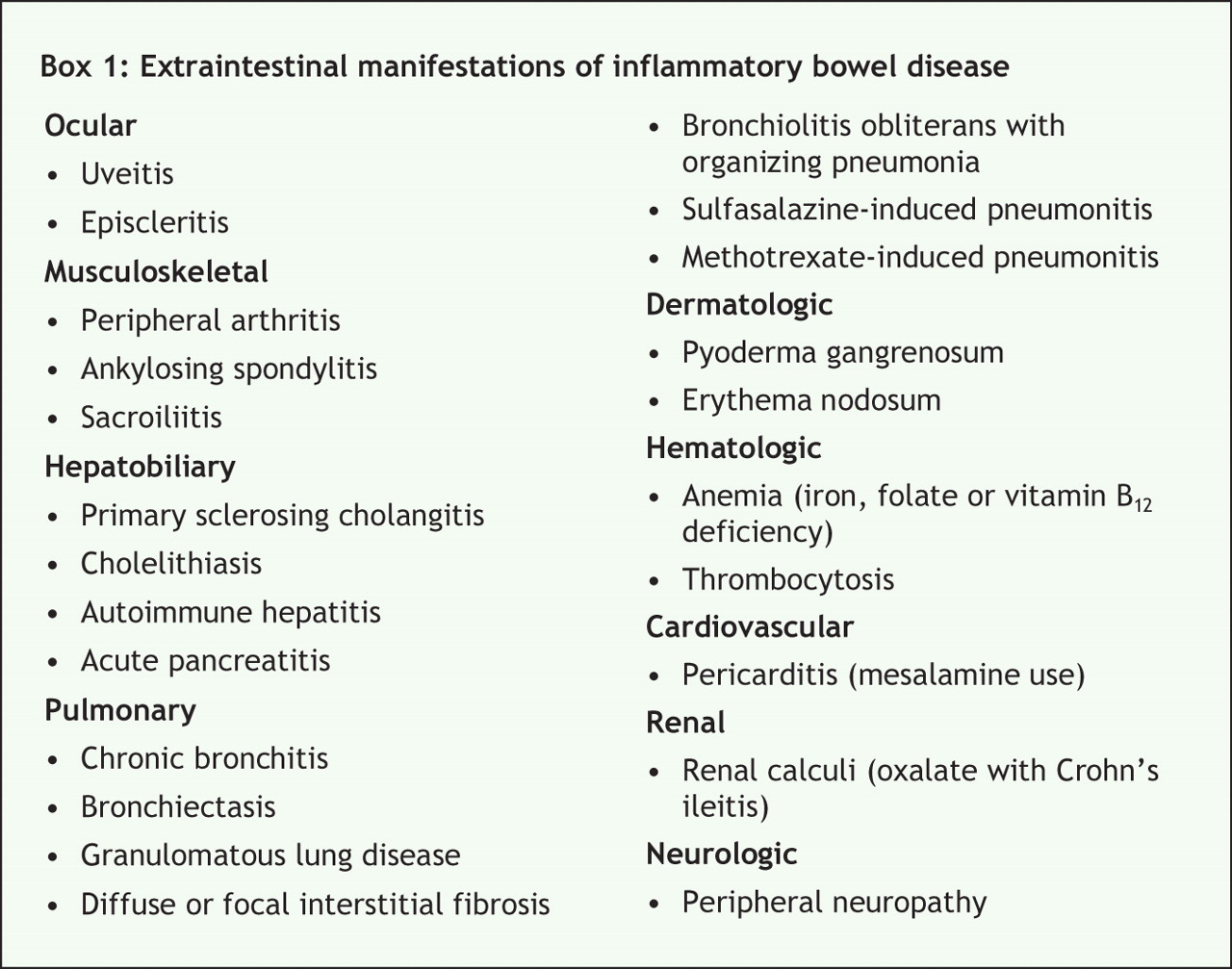
Inflammatory bowel disease has a variety of associated extraintestinal manifestations (Box 1).
Lung involvement is, for the most part, subclinical, as witnessed by abnormal pulmonary function tests in 40% of patients with inflammatory bowel disease and hyperresponsive bronchi in 45% of this population.4 The pulmonary conditions associated with inflammatory bowel disease are listed in Box 1.
Case reports of patients with Crohn's disease who have tracheobronchitis have described cough, dyspnea on exertion or acute respiratory failure as the presenting respiratory features. Our patient experienced progressively worse wheezing and dyspnea at rest over 3 days, to the point of becoming stridorous.
Tracheobronchitis, as occurred in our patient, has been reported in patients with active inflammatory bowel disease1 and may predate the onset of diarrhea (Box 2). The mucosal inflammation with whitish granular lesions is thought to be the equivalent of Crohn's-specific inflammation of the gastrointestinal tract because of its cobblestone appearance.4 Common pathogenic antigens may trigger activation of T cells and macrophages, which may account for the simultaneous bronchial and colonic mucosal inflammation.4 Inhaled or oral steroids (or both) have been successful in treating this condition, possibly by suppressing Th1-type cytokines (tumour necrosis factor α, interferon gamma).
Given our patient's multisystemic inflammation, we believed that intravenous steroid therapy followed by oral steroid therapy was merited.
Infliximab, as a tumour necrosis factor α antagonist, has been successful in treating extraintestinal manifestations that parallel intestinal inflammation, such as pyoderma gangrenosum, erythema nodosum, peripheral arthritis and episcleritis.5 In retrospect, such a therapeutic approach may have been useful in this case as well.
In conclusion, when patients with inflammatory bowel disease present with persistent respiratory symptoms, it is important to consider the possibility of tracheobronchitis. Severe airway stenosis secondary to tracheobronchitis has necessitated interventional pulmonology techniques such as dilatation and ablation of stenosed areas.2 If left untreated, this condition can progress to acute respiratory failure.1 Thus, early detection of tracheobronchitis associated with inflammatory bowel disease and efficacious treatment with steroids are essential. If the patient's presentation encompasses the spectrum of symptoms seen in our patient, the diagnosis becomes even more obvious.
Footnotes
-
This article has been peer reviewed.
Acknowledgements: We thank Drs. Georges Ghattas and Thomas Maniatis for their contributions to this case. We also thank Dr. Stewart Gottfried for the bronchoscopy images, Dr. René Michel for the pathology slides and Dr. Lawrence Stein for the virtual bronchoscopy images.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

