


- © 2007 Canadian Medical Association
Case 1: A previously healthy 51-year-old man came to hospital complaining of headache of 3 weeks' duration and several days of nausea, vomiting and confusion. He had some difficulty recalling the events of the preceding 3 weeks, but the results of his general and neurologic examinations were otherwise normal. A CT scan of the brain showed bilateral, symmetric infarcts in the heads of the caudate nuclei, with hyperdensity surrounding the anterior communicating artery. The infarcts were confirmed via MRI; conventional angiography showed a 4-mm saccular aneurysm of the anterior communicating artery (Fig. 1). To treat the aneurysm, we successfully inserted detachable coils endovascularly. Afterward, the patient remained medically stable and was discharged home 2 weeks later.

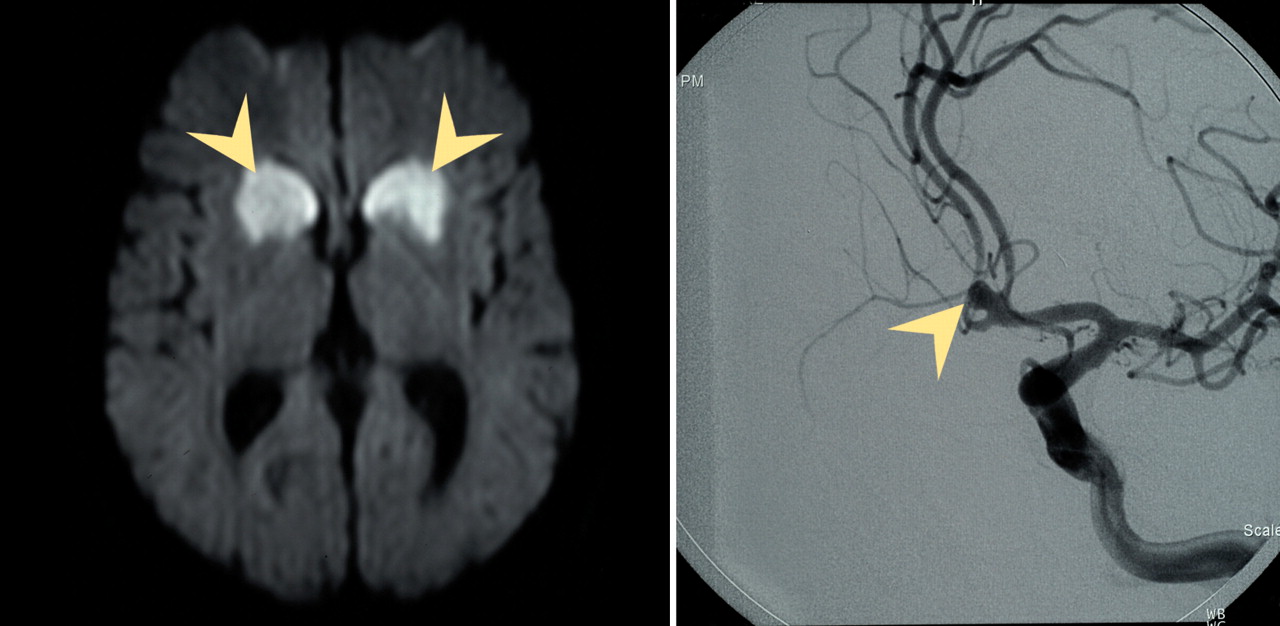
Fig. 1: Images of the brain, case 1. Left, a diffusion-weighted MRI scan showing large symmetric infarcts (arrowheads) in the heads of the caudate, the anterior limbs of the internal capsules and the basal ganglia. These are the areas fed by the recurrent arteries of Heubner. Right, an angiograph showing a large saccular aneurysm (arrowhead) in the patient's anterior communicating artery.
One month after discharge, he returned to hospital with a sudden onset of slurred speech, left-sided facial weakness and unsteady gait. Another CT scan revealed a new left thalamic hypodensity; MRI showed an acute infarct in the left thalamus and recent strokes in the pons and midbrain (Fig. 2). A cerebral angiograph showed bilateral narrowing of the M1 segments of the middle cerebral arteries. Results of transesophageal echocardiography were normal. Given the prominent headache, strokes in several vascular territories and arterial narrowing, we considered vasculitis of the central nervous system (CNS).

Fig. 2: Diffusion-weighted images of lacunar infarcts (arrowheads) in the right crus of the midbrain (left panel), left thalamus (centre panel) and left pons (right panel).
Results of cerebrospinal fluid (CSF) analysis showed a predominant lymphocytic pleocytosis (leukocytes 244 × 109/L, 71% lymph), low glucose (2.0 mmol/L) and markedly elevated protein levels (1.55 g/L). Results of a Venereal Disease Research Laboratory test of CSF were positive. Further serum testing provided a positive response to a rapid plasmin reagin test at a 1:64 dilution, confirmed by a Treponema pallidum hemagglutination assay and fluorescent treponemal antibody–absorption staining.
The patient was treated for meningovascular syphilis with penicillin G delivered intravenously at a dosage of 4 million units every 4 hours for 2 weeks.
On further examination of the patient's medical history, he did remember a painless penile ulcer that appeared about 1 year earlier. He denied any symptoms of systemic syphilis.
Case 2: A 54-year-old man arrived with a worsening headache of 2 weeks' duration and unsteady gait. Four months before, he had had an episode of complete right facial weakness and gait ataxia, which improved. Two months before presentation, he had experienced an infarct to his posterior cerebral artery distribution. This caused right hemisensory loss and right inferior visual-field loss associated with a severe headache that persisted for weeks.
A neurologic exam found right inferior quadrantanopsia, residual from his recent stroke. His motor and cerebellar results were normal; reflexes were easily elicited. He displayed impaired vibration sense and joint position sense bilaterally at the toes, his gait was broad-based and he exhibited Romberg's sign.
Given the prominent headache with stroke and new signs and symptoms of posterior column proprioceptive loss, we considered a diagnosis of syphilis.
Results of a rapid plasmin reagin test of serum were positive to a 1:16 dilution. Confirmatory tests also returned positive results, including a Venereal Disease Research Laboratory test of CSF, a serum T. pallidum hemagglutination assay and fluorescent treponemal antibody–absorption staining. CSF fluid analysis revealed a predominant lymphocytic pleocytosis (55 cells, 98% lymphocytes), with elevated protein (0.70 g/L) concentration, a normal glucose level and positive results of a Venereal Disease Research Laboratory test to a 1:4 dilution.
Gadolinium MRI scans of the brain and spine showed only the previous stroke in the left posterior cerebral artery. A conventional angiograph appeared normal, with no evidence of arterial narrowing. He was treated with penicillin G for 2 weeks (4 million units every 4 h, delivered intravenously).
On further questioning, the patient reported unprotected heterosexual encounters 10 years earlier, followed by the appearance of 2 painless penile ulcers. These resolved with antibiotic treatment.
Syphilis, a chronic multisystem infection by Treponema pallidum, can be spread venereally or vertically. The disease passes through a series of frequently overlapping stages.1 The incidence of infectious syphilis has recently increased in Canada from 0.6 cases per 100 000 population (174 patients) in the year 2000, to 3.5 per 100 000 (1127 patients) in 2004.2 Neurosyphilis occurs with CNS invasion, typically in secondary and later stages of syphilis. Incidence data for neurosyphilis, unfortunately, are unavailable.
In the pre-antibiotic era, symptomatic neurosyphilis developed in about one-third of patients; parenchymal forms involving the brain and spinal cord (syphilitic encephalitis, tabes dorsalis) were seen the most often. With the advent of penicillin therapy, the typical clinical presentation has shifted away from chronic forms of neurosyphilis, which involve CNS parenchyma, to earlier forms that involve CNS meninges and blood vessels (e.g., syphilitic meningitis, meningovascular syphilis with associated ischemic stroke).3 Persistent and prominent headache in a patient can alert the clinician to early neurosyphilis. Unfortunately, the nonspecific nature of headache and a lack of other obvious signs can leave patients vulnerable to undiagnosed deterioration, particularly in cases of syphilitic vasculitis.
The most common form of syphilitic vasculitis, Heubner's arteritis, is a crescentic endarteritis obliterans affecting large-and medium-sized arteries.4 It is characterized by fibrous and inflammatory changes in the adventitia, along with thinning of the media and fibroblastic proliferation of the intima, leading to progressive stenosis. Vascular occlusion results in ischemia and subsequent infarction.
Aneurysms of the aorta are known to occur in syphilis, but a cerebral aneurysm secondary to syphilitic vasculopathy has been reported only once, in a patient with an aneurysm of the posterior communicating artery.5 We were unable to locate another report of an anterior communicating artery aneurysm associated with meningovascular syphilis; in fact, the aneurysm may have been an incidental finding.
The increasing incidence of syphilis should alert clinicians to consider CNS complications of syphilis. The combination of prominent and persistent headaches and stroke may suggest meningovascular syphilis even in the absence of meningism.
Physicians who manage stroke patients should be aware of early systemic features of syphilis, such as previous chancre, regional lymphadenopathy, alopecia, uveitis, retinitis and rash. They should inquire into risk factors for and history of sexually transmitted infections. Nontreponemal syphilis screening tests such as the rapid plasmin reagin test should be reincorporated into the diagnostic workup of any young patient with stroke and all patients with stroke who have the historical or clinical features outlined.
Syphilis has been described as “the great imitator.” Its recurrence within Canada will challenge clinicians to reeducate themselves about the varied manifestations of this timeless disease.
Footnotes
-
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

