


Abstract
Background: There is no single generally accepted clinical definition of frailty. Previously developed tools to assess frailty that have been shown to be predictive of death or need for entry into an institutional facility have not gained acceptance among practising clinicians. We aimed to develop a tool that would be both predictive and easy to use.
Methods: We developed the 7-point Clinical Frailty Scale and applied it and other established tools that measure frailty to 2305 elderly patients who participated in the second stage of the Canadian Study of Health and Aging (CSHA). We followed this cohort prospectively; after 5 years, we determined the ability of the Clinical Frailty Scale to predict death or need for institutional care, and correlated the results with those obtained from other established tools.
Results: The CSHA Clinical Frailty Scale was highly correlated (r = 0.80) with the Frailty Index. Each 1-category increment of our scale significantly increased the medium-term risks of death (21.2% within about 70 mo, 95% confidence interval [CI] 12.5%–30.6%) and entry into an institution (23.9%, 95% CI 8.8%–41.2%) in multivariable models that adjusted for age, sex and education. Analyses of receiver operating characteristic curves showed that our Clinical Frailty Scale performed better than measures of cognition, function or comorbidity in assessing risk for death (area under the curve 0.77 for 18-month and 0.70 for 70-month mortality).
Interpretation: Frailty is a valid and clinically important construct that is recognizable by physicians. Clinical judgments about frailty can yield useful predictive information.
Frailty is a term widely used to denote a multidimensional syndrome of loss of reserves (energy, physical ability, cognition, health) that gives rise to vulnerability. It appears to be a valid construct, but how exactly to define it remains unclear.1,2,3,4,5,6,7,8 There are many operational definitions,1,5,9,10,11,12,13 which typically are rules-based; for example, a person may be defined as frail if 3 or more symptoms (of unintentional weight loss, feeling exhausted, weak grip strength, slow walking speed and low physical activity) are present.5 Rules-based definitions often are derived from multiple regression analyses and can be speciously precise, for example in requiring combinations of factors that might not apply to an individual case.
Summing the number of impairments is another way to define frailty.2 Despite its strong predictive validity,2,14,15 this approach is time-consuming and not widely used clinically. A third class of operational classifications, which in this report we attempt to extend, relies on clinical judgment to interpret the results of history-taking and clinical examination.16,17
The creation of so many scales to measure frailty reflects uncertainty about the term and its components. The ability to measure frailty is useful at a health care policy level as well as clinically: Information about frailty helps program planners by identifying the range of services that might be required and the anticipated need for them. Clinically, frailty stratification can help to plan interventions or to predict a patient's risk of death or need for institutional care. Because the scales are intended to stratify risk, the ability to predict adverse outcomes serves a common goal.
In the Canadian Study of Health and Aging (CSHA), we have worked with 3 approaches. First, like other groups, we developed a rules-based definition of frailty.12 Later, we developed (and still actively work with) a method of counting a patient's clinical deficits (identified by means of signs, symptoms and abnormal test results). This approach is reproducible and correlates highly with mortality,2 but in clinical use the deficit count is unwieldy. In this paper, we describe our third approach: the derivation and validation of the Clinical Frailty Scale, a measure of frailty based on clinical judgment.
Methods

The CSHA is a representative 5-year prospective cohort study. Its first stage of investigation (CSHA-1) began in 1991 with 10 263 people aged 65 years and older, recruited with the aim of describing the epidemiology of cognitive impairment and other important health issues in elderly Canadians.18,19,20 From the clinical examinations we did within this cohort, we developed the rules-based frailty definition12 and the Frailty Index, a measure of frailty obtained by counting various clinical deficits (Appendix 1). Afterward, we also developed CSHA scales for function and overall clinical frailty, with the goal of creating tools that could stratify elderly patients as to their relative degree of vulnerability (i.e., their risks of death and of entry into an institutional facility) with simple clinical descriptors. We defined the Clinical Frailty Scale using the terminology of Streiner and Norman.21 Rooted in our theoretical model of fitness and frailty7 and the importance of function (which we reported in earlier investigations),12 our Clinical Frailty Scale (Box 1) ranges from 1 (robust health) to 7 (complete functional dependence on others).
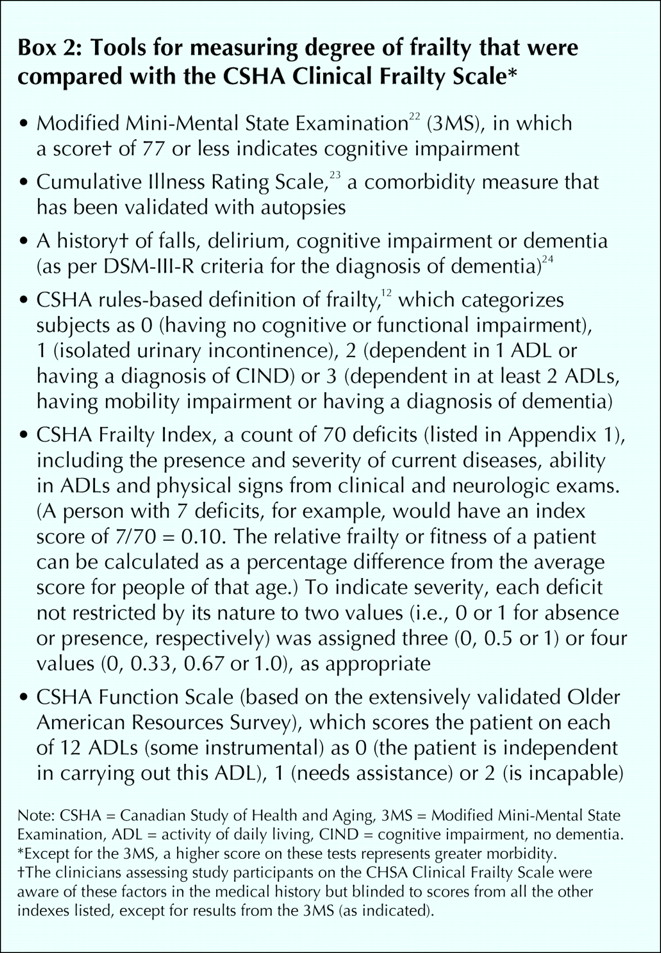
In 1996, we began CSHA-2, the second stage of the study. Of the 10 263 people in CSHA-1 who had been examined clinically and found to be without dementia, 2305 (22.5%) were examined again by one of a team of clinicians (33 family physicians, 30 internists or geriatricians, 11 neurologists and 3 psychiatrists), who then applied the Clinical Frailty Scale and the other measures in Box 2, for comparison. This reduced study population (874 men [37.9%] and 1431 women) consisted of 210 people (9.1%) who had entered institutional facilities since CSHA-1; 1326 (57.5%) who were still living at home or elsewhere in the community and whose 3MS screening results in CSHA-2 now indicated cognitive impairment (i.e., a 3MS score of 77 or less); and 769 (33.4%), also living within the community, whose 3MS scores remained at 78 or greater and who formed a comparison group.
Our objective in the present study (CSHA-3), begun in 2001, was to validate the Clinical Frailty Scale by following those patients who remained alive 5 years after CSHA-2 (1299/ 2305 [56.4%]). Follow-up vital and domicile status (living in the community or in an institution) was known for all 2305 participants who did not have dementia at the time of CSHA-2, of whom 249 had entered an institutional facility between CSHA-2 and -3.
At the end of the clinical interview in CSHA-2, the interviewing physician assigned the subject a score of 1 to 7 on the Clinical Frailty Scale. Each interview was reviewed and scored again by a multidisciplinary team that included the physician and therefore was not blinded to the initial score.
Given the increased likelihood of falls, episodes of delirium and cognitive impairment among people who are frail, we recorded that information. Physicians making the initial Clinical Frailty Scale assessment had access to diagnoses and assessments related to these variables and other measures of comorbidity, function and associated features that inform clinical judgments about the severity of frailty. They were, however, unaware of subjects' results on other frailty indexes. The subjects assessed were almost always new to the clinician involved.
To assess the construct validity of the CSHA Clinical Frailty Scale, in the analysis we compared patients' scores from the initial assessments only with their results from other established tools that indicate the degree of frailty by measuring function and comorbidity1 (see Box 2).12,23,24,25,26 When applying the CSHA Function Scale, we excluded “walking” and “transferring” because data from nursing homes were incomplete for many patients.
The Frailty Index is a count of 70 clinical deficits from the CSHA clinical assessment (Appendix 1). Items included the presence and severity of current diseases, ability in the activities of daily living, and physical and neurological signs from the clinical examinations. Each deficit was dichotomized or trichotomized and mapped to the interval 0–1 (i.e., individual assessment items could be scored as 0, 0.33, 0.50, 0.67 or 1.0) to represent the severity or frequency of the problem (see Box 2). No variable had more than 5% missing data. Except for the Clinical Frailty Scale (which was completed on all but 8 patients), any values that were missing were imputed using the relevant mean.
We used Pearson or Spearman correlation coefficients to measure the degree of correlation (i.e., to test convergent construct validity) between the Clinical Frailty Scale and the other, established measurement tools. To assess predictive validity, an aspect of criterion validation,21 we constructed Kaplan–Meier curves per scale category. All significance tests were 2-sided; differences were assessed for significance (p ≤ 0.05) with the log–rank test. In the multivariable analyses, having first checked for proportionality, we used Cox regression analyses to estimate hazard ratios and construct 95% confidence intervals (CIs) independently for the 3MS score22 and outcomes of the CSHA Clinical Frailty Scale, and the Cumulative Illness Rating Scale,23 as well as the CSHA's Function Scale, rules-based frailty definition12,16 and Frailty Index,2 adjusting each for age, sex and years of education. Receiver operating characteristic (ROC) curves27 were calculated to estimate the areas under the curves for relevant predictor variables in relation to death and entrance into an institutional facility. An intraclass correlation coefficient was used to assess interrater reliability between the 2 Clinical Frailty Scale ratings (i.e., the initial scorings done by physicians and those done later by multidisciplinary teams during CSHA-2).
The research ethics committees of each institution approved the study, and all participants (or their designates) signed informed-consent forms. CSHA funding was chiefly (> 95%) public and from a variety of sources, as specified in the Acknowledgements. Sponsors had no role in the selection of the objectives or in the analysis, write-up or submission of this report.
Results
Table 1.
Participants with higher scores on the Clinical Frailty Scale were older and more likely to be female, cognitively impaired and incontinent; to have impaired mobility and function: and to have more comorbid illnesses than those with lower scores (Table 1). They also had higher scores according to both the Frailty Index and the rules-based frailty definition.12,16 Of note, at the highest level of frailty our participants had fewer falls, probably reflecting the greater proportion who were bedridden. The degree of correlation between the judgment-based CSHA Clinical Frailty Scale and the mathematically derived Frailty Index was high (Pearson coefficient 0.80, p < 0.01), confirming construct validity. The Clinical Frailty Scale and the Frailty Index each correlated to a similar degree with age (0.35 and 0.29, respectively); the 3MS measure of cognition (0.58, 0.59); the Cumulative Illness Rating Scale, which measures comorbidity (0.43, 0.48); the CSHA Function Score (0.78, 0.74); and the CSHA rules-based frailty definition (0.67 and 0.65, respectively). Reliability between the 2 ratings of the CSHA Clinical Frailty Scale assessments was very high (intraclass correlation coefficient 0.97, p < 0.001).
Table 2.
Hazard ratios for death and entry into an institutional facility (Table 2) in each case showed increasing risk with increasing frailty (Fig. 1, upper graph). ROC curve analyses of the CSHA Clinical Frailty Scale and the Frailty Index revealed similar areas under the curves, a performance better than that of the other measures (Table 3). The best result was achieved for near-term mortality (death within 18 months), with an area under the curve of 0.77.

Fig. 1: Kaplan–Meier curves, adjusted for age and sex, for study participants (n) over the medium term (5–6 years), according to their scores on the CSHA Clinical Frailty Scale. Some scores were grouped. Top: Probability of survival. Bottom: Probability of avoidance of institutional care.
Similarly, worse frailty was associated with an increased probability of entering an institutional facility (Fig. 1, lower graph). The Clinical Frailty Scale and the Frailty Index had comparable performances in ROC analyses, which again was better than the performance of the 3MS or Cumulative Illness Rating Scale tools (Table 3). However, the CSHA Function Scale showed significantly better performance than all other measures in assessing risk for entry into an institution.
Table 3.
In multivariable models that adjusted for age, sex and education (Fig. 1), each 1-category increment of our Clinical Frailty Scale significantly increased the medium-term risks (i.e., those within about 70 months) of death (21.2%, 95% CI 12.5%–30.6%) and entry into institutional care (23.9%, 95% CI 8.8%– 41.2%).
Interpretation
We have shown that the Clinical Frailty Scale is an effective measure of frailty and provides predictive information similar to that of other established tools about death or the need for an institution. The Clinical Frailty Scale is easy to use and may readily be administered in a clinical setting, an advantage over the tools previously developed. For example, counting deficits with the Frailty Index is easy to understand, and powerfully correlates the relation between frailty and death; on the other hand, it requires the physician to consider a list of no fewer than 70 possible disorders. The 7-category Clinical Frailty Scale showed good criterion validity, with a dose– response effect in relation to 5-year prediction of death or entry into an institutional facility and reasonable construct validity, with worse health characteristics associated with increasing frailty.
The Clinical Frailty Scale mixes items such as comorbidity, cognitive impairment and disability that some other groups separate in focusing on physical frailty.3 Although support exists for separate approaches,28 consensus does not,1,2 and there are reasons to be skeptical. The physical frailty approach rests on unspecified assumptions about an unquantitated “physiological reserve”; its predictive validity is no better than a more comprehensive account. Empirically, most elderly patients who are physically frail show some level of disability, although this aspect of the debate depends on the definitions employed29,30,31,32 and in any case would be captured by our designation of being “apparently vulnerable.”
Applying the Clinical Frailty Scale to patients requires judgment. The fabric of individual health has many strands, and it seems likely that some clinicians sometimes used factors not precisely specified in our brief set of descriptors. Some readers might be inclined to view such subjectivity poorly, but we do not see flexibility as a weakness: Different clinicians will emphasize different aspects of illness differently — as in, for example, a psychiatrist and a neurologist each validly concluding, by distinct processes, that a given patient has frontotemporal dementia. Such flexibility is widely validated in similar settings.33,34,35,36 It also appears to us to be analogous to the advanced computing techniques that we have used in recent inquiries to enhance the performance of the high-dimension Frailty Index.15,37 For instance, an artificial neural network can be used to calculate weighted scores, and can significantly improve the Frailty Index's predictive performance over an unweighted version.15
What an artificial neural network cannot do, however, is describe which factors most increase risk. This appears to us to be analogous to clinical judgments about the same phenomenon. Both clinical judgment and such advanced computational techniques can be contrasted with a rules-based frailty approach, which specifies combinations a priori but at the expense of not including the patients that most clinicians would recognize as frail.
The present inquiry showed that the predictive validity of the CSHA's Frailty Index and Clinical Frailty Scale were indistinguishable; moreover, both measures performed better in this regard than did the rules-based frailty definition. On these grounds, and given that rules-based combinations cannot fully embrace the complexity of states in which individual people can find themselves, a judgment-based system seems to be a reasonable way to measure relative fitness and frailty. For such an instrument to be used routinely, however, more information is needed about its interrater reliability, which is the subject of additional studies. Until those study results become available, the Clinical Frailty Scale can be used to provide broad guidelines for helping to advise about the best mix of care for elderly patients.
Our data must be interpreted with caution. Although CSHA was population-based, CSHA-2 clinical examinations overrepresent people with cognitive impairment and those in institutions. This probably accounts for the Clinical Frailty Scale's bimodal distribution, with peaks at 3 (“well, with treated comorbid disease”) and at 6 (“moderately frail”). On the other hand, the Clinical Frailty Scale showed a wider distribution than might be expected with a purely clinical sample, and our study was large enough to generate estimates with narrow confidence intervals. The only measure of test–retest or interrater reliability available to us was unblinded; that reliability estimate is therefore likely to be higher than would be the case in usual practice. Category 7 appeared to mix 2 groups that seem distinct: terminally ill people (who might still be independent) and those who are totally dependent on others tao carry out their activities of daily living. Although people in category 7 had a high mortality, these subgroups routinely would be distinguished clinically; future users of the scale might do well to subdivide these groups, especially in acute care settings.
We can envisage future roles for CSHA's Frailty Index and Clinical Frailty Scale alike. The judgment-based scale might be better exploited where clinicians are available who have experience in the care of elderly people. The index approach might better serve where such access is unavailable. The index approach also appears to have some important mathematical advantages in its scaling that might lead to novel insights,2,38,39 especially into matters such as physiologic reserve, which is often invoked in relation to frailty but little measured. Given the increasingly elderly population, and the particular challenge posed by elderly people who are frail, the important questions for researchers now are how to measure frailty more precisely and how to better translate frailty measurement into clinically sensible tools and practices.
Footnotes
-
This article has been peer reviewed.
Contributors: Kenneth Rockwood designed the study, wrote the first and final drafts of the manuscript, and supervised the analyses. Xiaowei Song and Arnold Mitnitski conducted and verified all the analyses. (Arnold Mitnitski and Kenneth Rockwood previously devised and tested the Frailty Index.) Kenneth Rockwood, Chris MacKnight, David Hogan and Howard Bergman examined patients. Ian McDowell, Chris MacKnight and David Hogan commented on and revised interim drafts. All authors contributed to and approved the final published version and support the presented results.
Acknowledgements: This analysis was supported by grants from the National Health Research Development Program of Health Canada (grant no. 6603-1417-55) and the Queen Elizabeth II Research Foundation. The data reported in this article were collected as part of the Canadian Study of Health and Aging. The core study was funded by the Seniors' Independence Research Program, through the National Health Research and Development Program, project no. 6606-3954-MC (S). Additional funding was provided by Pfizer Canada Incorporated through the Medical Research Council/Pharmaceutical Manufacturers Association of Canada Health Activity Program, the National Health Research and Development Program, project no. 6603-1417-302(R). The study was coordinated through the University of Ottawa and Health Canada's Division of Aging and Seniors. Additional funds for analysis came from the Canadian Institutes for Health Research (CIHR) grant MOP 62823 and the Dalhousie University Internal Medicine Research Foundation. Kenneth Rockwood and Chris MacKnight receive CIHR support through Investigator and New Investigator awards, respectively. Kenneth Rockwood is also supported by the Dalhousie Medical Research Foundation as Kathryn Allen Weldon Professor of Alzheimer Research. Howard Bergman is Dr. Joseph Kaufman Professor of Geriatric Medicine at McGill University, and David Hogan is Brenda Strafford Foundation Chair in Geriatric Medicine at the University of Calgary.
Competing interests: None declared.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- An international factorial vignette-based survey of intubation decisions in acute hypoxemic respiratory failure
- Health-related quality of life after 12 months post discharge in patients hospitalised with COVID-19-related severe acute respiratory infection (SARI): a prospective analysis of SF-36 data and correlation with retrospective admission data on age, disease severity, and frailty
- Influence of frailty on cardiovascular events and mortality in patients with Chronic Obstructive Pulmonary Disease (COPD): Study Protocol for a multicentre European observational study
- Clinical phenotypes and outcomes associated with SARS-CoV-2 Omicron variant JN.1 in critically ill COVID-19 patients: a prospective, multicenter cohort study
- Development and external validation of a practical diagnostic support tool, 'ABC2-Screener, to predict sarcopenia among patients on maintenance haemodialysis: A multicentre cross-sectional study
- Using illness trajectories to inform person centred, advance care planning
- Evaluation of a Low-threshold Exercise And Protein supplementation intervention for Women (LEAP-W) experiencing homelessness and addiction: Protocol for a single site intervention study
- Tailoring follow-up endoscopy in patients with severe oesophagitis
- Rationale and design of the United Kingdom Heart Failure with Preserved Ejection Fraction Registry
- Association between the frailty index and readmission risk in hospitalised elderly Chinese patients: a retrospective cohort study
- Unveiling Frailty: Comprehensive and Sex-Specific Characterization in Prematurely Aging PolgA Mice
- What are the factors that determine treatment choices in patients with kidney failure: a retrospective cohort study using data linkage of routinely collected data in Wales
- Longitudinal Fragility Phenotyping Predicts Lifespan and Age-Associated Morbidity in C57BL/6 and Diversity Outbred Mice
- Epidemiology of Tracheostomized Adult Patients Admitted to Specialized Weaning Centers After Acute COVID-19
- Developing a framework of concerns from people living with frailty, for the Measure Yourself Concerns and Wellbeing (MYCaW) person-centred outcome measure
- Study protocol for a national observational cohort investigating frailty, delirium and multimorbidity in older surgical patients: the third Sprint National Anaesthesia Project (SNAP 3)
- Prevalence, risks and outcomes of frailty in People Experiencing Homelessness: a protocol for secondary analysis of Health Needs Audit data
- Association between frailty assessed by the Clinical Frailty Scale 2.0 and outcomes of acute stroke in older patients
- Protocol for the Tallaght University Hospital Institute for Memory and Cognition-Biobank for Research in Ageing and Neurodegeneration
- Derivation of the Falls Decision Rule to exclude intracranial bleeding without head CT in older adults who have fallen
- Using the Primary care Academic CollaboraTive to explore the characteristics and healthcare use of older housebound patients in England: protocol for a retrospective observational study and clinician survey (the CHiP study)
- GP assessment of unmet need in a complex multimorbid population using a data-driven and clinical triage system: a prospective cohort study
- Comparison of frailty instruments in acute coronary syndrome patients
- Prehospital early warning scores for adults with suspected sepsis: retrospective diagnostic cohort study
- Protocol of the Berlin Long-term Observation of Vascular Events (BeLOVE): a prospective cohort study with deep phenotyping and long-term follow up of cardiovascular high-risk patients
- Feasibility of frailty screening among patients with advanced heart failure
- Prevalence of frailty among elderly patients with hip fracture in China: protocol for a systematic review and meta-analysis
- Low body mass index patients have worse outcomes after mechanical thrombectomy
- Silver Trauma Review Clinic: a novel model of care to manage non-operative injuries in older patients
- The Healthy Brain Initiative (HBI): A prospective cohort study protocol
- Peri-Operative Wearables in Elder Recover after Surgery (POWERS) study: a protocol for a multicentre, prospective cohort study to evaluate perioperative activity with postoperative disability in older adults after non-cardiac surgery
- Contact patterns of older adults with and without frailty in the Netherlands during the COVID-19 pandemic
- Temporal Muscle Thickness Correlates with Sarcopenia in Parkinsons Disease
- Study protocol for the 'preventing functional decline in acutely hospitalised older patients (PREV_FUNC) study: effects of two multicomponent exercise programmes on physical function - a three-armed randomised controlled trial
- European Respiratory Society statement on frailty in adults with chronic lung disease
- Clinical Frailty Scale as a predictor of adverse outcomes following aortic valve replacement: a systematic review and meta-analysis
- Effects of ageing and frailty on circulating monocyte and dendritic cell subsets
- Prevalence of swallow, communication, voice and cognitive compromise following hospitalisation for COVID-19: the PHOSP-COVID analysis
- PREhabilitation of CAndidates for REnal Transplantation (PreCareTx) study: protocol for a hybrid type I, mixed method, randomised controlled trial
- The impact of frailty on the outcomes of COVID-19 patients with persistent critical illness: A population-based cohort study
- Effect of prehabilitation-related DIETary protein intake on Quality of Recovery after elective cardiac surgery (DIETQoR) study: protocol of a randomised controlled trial
- Approche de traitement des adultes ages atteints dinsuffisance renale chronique
- Protocol paper for SMART OPS: Shared decision-making Multidisciplinary Approach - a Randomised controlled Trial in the Older adult Population considering Surgery
- Impact of Frailty Upon Surgical Decision-Making for Left-Sided Colon Cancer
- Cross-cultural adaptation and its impact on research in emergency care
- Using home monitoring technology to study the effects of traumatic brain injury on older multimorbid adults: protocol for a feasibility study
- Impact of the COVID-19 pandemic on people in need of care or support: protocol for a SARS-CoV-2 registry
- Contact patterns of frail and non-frail elderly persons in the Netherlands during the COVID-19 pandemic
- Clinical frailty and polypharmacy in older emergency critical care patients: a single-centre retrospective case series
- An approach to treating older adults with chronic kidney disease
- Clinical features and outcomes of hospitalised patients with COVID-19 and Parkinsonian disorders: a multicentre UK-based study
- Impact of Frailty Upon Surgical Decision-Making for Left-Sided Colon Cancer
- Development and validation of a hospital frailty risk measure using Canadian clinical administrative data
- Cross-cultural adaptation and its impact on research in emergency care
- Frail2Fit study protocol: a feasibility and acceptability study of a virtual multimodal intervention delivered by volunteers to improve functional outcomes in older adults with frailty after discharge from hospital
- Association Between Frailty and Antiseizure Medication Tolerability in Older Adults With Epilepsy
- The Silver Trauma Review Clinic: A novel model of care to manage non-operative injuries in older patients
- The Hospital to Home study (H2H): smartwatch technology-enabled rehabilitation following hip fracture in older adults, a feasibility non-randomised trial
- Association between frailty, chronic conditions and socioeconomic status in community-dwelling older adults attending primary care: a cross-sectional study using practice-based research network data
- Configurations and outcomes of acute hospital care for frail and older patients with moderate to major trauma: a systematic review
- Study protocol for neuromuscular stimulation for rehabilitation after general and vascular surgery: a pilot randomised clinical study
- Registry for Evaluating Healthy Life Expectancy and Long-Term Outcomes after Catheter Ablation of Atrial Fibrillation in the Very Elderly (REHEALTH AF) study: rationale and design of a prospective, multicentre, observational, comparative study
- Multimodal prehabilitation for major surgery in elderly patients to lower complications: protocol of a randomised, prospective, multicentre, multidisciplinary trial (PREHABIL Trial)
- Approche de la nephropathie chronique chez les personnes agees
- Approach to chronic kidney disease in the elderly
- Treatment decision-making and care among older adults with kidney failure: protocol for a multicentre, prospective observational cohort study with nested substudies and linked qualitative research (the Elderly Advanced CKD Programme)
- Frailty assessment in the management of cardiovascular disease
- How is COVID-19 changing the ways doctors make end-of-life decisions?
- Short Graphic Values History Tool for decision making during serious illness
- Aetiological and prognostic roles of frailty, multimorbidity and socioeconomic characteristics in the development of SARS-CoV-2 health outcomes: protocol for systematic reviews of population-based studies
- The Forgotten Hip Fracture: Outcomes Of Lower Limb Periprosthetic Fractures
- Investigating the association between IL-6 antagonist therapy and blood coagulation in critically ill patients with COVID-19: a protocol for a prospective, observational, multicentre study
- Association between Goals of Care Designation orders and health care resource use among seriously ill older adults in acute care: a multicentre prospective cohort study
- Emergency care for older people living with frailty: patient and carer perspectives
- Effect of a patient education video and prehabilitation on the quality of preoperative person-centred coordinated care experience: protocol for a randomised controlled trial
- MiCare study, an evaluation of structured, multidisciplinary and personalised post-ICU care on physical and psychological functioning, and quality of life of former ICU patients: a study protocol of a stepped-wedge cluster randomised controlled trial
- Development and validation of a dynamic 48-hour in-hospital mortality risk stratification for COVID-19 in a UK teaching hospital: a retrospective cohort study
- Effect of age, sex, and morbidity count on trial attrition: meta-analysis of individual participant level data from phase 3/4 industry funded clinical trials
- Clinical frailty and performance scale translation in palliative care: scoping review
- PREPARE trial: a protocol for a multicentre randomised trial of frailty-focused preoperative exercise to decrease postoperative complication rates and disability scores
- Development and assessment of an educational intervention to improve the recognition of frailty on an acute care respiratory ward
- Use of a Self-Care and Educational Mobile App to Improve Outcomes of Patients with Acute Decompensated Heart Failure during the COVID-19 Pandemic
- Evaluating instruments for assessing healthspan: a multi-center cross-sectional study on health-related quality of life (HRQL) and frailty in the companion dog
- Safety, feasibility and initial efficacy of an app-facilitated telerehabilitation (AFTER) programme for COVID-19 survivors: a pilot randomised study
- Characteristics, treatment and delirium incidence of older adults hospitalized with COVID-19: a multicentre retrospective cohort study
- The association of typical and atypical symptoms on in-hospital mortality of older adults with COVID-19: a multicentre cohort study
- Multispecialty multidisciplinary input into comorbidities along with treatment optimisation in heart failure reduces hospitalisation and clinic attendance
- Duration of External Neck Stabilisation (DENS) following odontoid fracture in older or frail adults: protocol for a randomised controlled trial of collar versus no collar
- Frailty on the acute medical take
- FARGO-360: a multi-disciplinary survey of practice and perspectives on provision of care for patients with frailty presenting with gynecological cancers in the UK and Ireland
More in this TOC Section
Similar Articles
Collections

