


- © 2005 CMA Media Inc. or its licensors
Abstract
PERSISTENT LOW-GRADE INFLAMMATION, as indicated by higher circulating levels of inflammatory mediators such as C-reactive protein, interleukin-6 and tumour necrosis factor-α, is a strong risk factor for several chronic diseases. There are data indicating that decreasing energy intake and increasing physical activity may be effective therapies for reducing overall inflammation. Evidence is strong that circulating levels of inflammatory markers are elevated with total and abdominal obesity, possibly owing to a higher secretion rate of cytokines by adipose tissue in obese people. Moreover, very-low-energy dietary weight loss reduces both circulating markers of inflammation and adipose-tissue cytokine production. Data from several large population-based cohorts show an inverse association between markers of systemic inflammation and physical activity or fitness status; small-scale intervention studies support that exercise training diminishes inflammation. Dietary weight loss plus exercise is likely more effective than weight reduction alone in reducing inflammation. To date, data from randomized, controlled trails designed to definitively test the effects of weight loss or exercise training, or both, on inflammation are limited. Future studies are required to define the amount of weight loss needed for clinically meaningful reductions of inflammation; in addition, fully powered and controlled studies are necessary to clarify the effect of exercise training on chronic, systemic inflammation.
The biologic cascade of events that form the body's natural defenses against injury or infection is a vital part of the immune system. Ordinarily, this process is an acute response resulting in rapid, major increases in inflammatory mediators released into the circulation.1,2 In healthy, lean, non-elderly people, for example, blood concentrations of the acute-phase reactant C-reactive protein (CRP), which are normally less than 2 mg/L in men3 and less than 2.5 mg/ L in women,4 can increase more than 1000-fold in response to infection or trauma.2,5,6
Typically, a CRP value of 10 mg/L or more is considered indicative of clinically significant inflammation.7 However, recent evidence indicates that persistent elevations in circulating markers of inflammation, even when within the clinically normal range, are risk factors for cardiovascular disease in both middle-aged8,9,10,11,12,13 and older14,15,16,17,18,19 people. Recently, the US Centers for Disease Control and Prevention and the American Heart Association have stated that people with CRP values in the upper tertile of the adult population (> 3.0 mg/L) have a risk of cardiovascular disease that is double that of people whose CRP concentrations are less than 1.0 mg/L.20 In addition to CRP, interleukin-6 (IL-6) and tumour necrosis factor-alpha (TNF-α), along with several other acute- phase reactant proteins, cytokines and cytokine-soluble receptors, are strongly associated with increased risk for several chronic diseases, including cardiovascular disease,12,17,21,22 diabetes mellitus23,24 and disability.25,26 IL-6 and TNF-α are both stimulators of CRP release from hepatocytes.27,28 It is not yet known which of these factors might be the most robust indicator of underlying inflammation, or whether the effects of these biomarkers are additive for risk prediction.
As illustrated in Figure 1, behavioural factors are associated with chronic, low-grade states of inflammation (as measured by slightly elevated inflammatory biomarkers), and therefore with the several chronic diseases that are associated with inflammatory states. Since the risk estimates associated with elevated inflammation appear to be linear (e.g., the CRP category cut-offs for assessment of cardiovascular disease risk20 are low risk < 1.0 mg/L, medium risk 1.0–3.0 mg/L and high risk > 3.0 mg/L), behavioural interventions that produce even slight reductions in inflammation may have clinically significant benefits. A few pharmacologic interventions such as use of angiotensin- converting-enzyme inhibitors and statins decrease inflammation, as evidenced by lowered CRP concentrations in prospective clinical trials.29,30,31,32 Moreover, there are very promising data suggesting that decreasing body weight and increasing physical activity are just as effective as medication for reducing overall inflammation. The published effects of behavioural interventions involving weight loss and exercise training on inflammatory markers are reviewed here.

Fig. 1: Reported behavioural factors associated with chronic subclinical inflammation, and diseases and adverse health conditions for which inflammation is a risk factor. ↓ = decreased; BMI = body mass index.
Role of adiposity and weight loss in regulating inflammation
Evidence from observational studies
The association between excess adipose tissue (measured either indirectly by body mass index [BMI] or directly by body composition assessment) and elevated CRP concentrations33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51 has been observed to hold for children,36,40,45 elderly people14,50 and people with metabolic syndrome,49 diabetes48 and heart disease.52 In fact, obesity may account for a large portion of variation in circulating CRP concentrations; in a population-based study involving healthy, middle-aged women,35 for example, BMI explained 30% of the variance in CRP concentrations. In an analysis33 of the Third National Health and Nutrition Examination Survey, the proportion of people with a CRP level above 10 mg/L (the traditional clinical level suggestive of infection) was 20% in obese women, but only 4% in women whose weight was within the normal range. Obese participants were more likely than participants of normal weight to have an elevated CRP level, by an odds ratio of 2.13 for men (95% confidence interval [CI] 1.56– 2.91) and 6.21 for women (95% CI 4.94–7.81).33 Similarly, in a study involving 1929 middle-aged men and women,49 15% of obese participants had a CRP level above 10 mg/L, compared with only 3% of normal-weight people.
Other inflammatory markers, including the cytokines IL- 6,34,53,54,55,56,57,58,59,60 TNF-α,34,58,59,61,62,63,64,65 TNF-α receptors,57,60,63,66,67,68 IL- 8,69,70 IL-1856,58,59,71 and IL-1 receptor antagonist,72,73 are elevated in obese people. Haptoglobin and serum amyloid protein A, both proteins involved in the acute-phase response to inflammation, have also been shown to circulate in higher concentrations in people with more body fat.74,75,76 The sample sizes in these studies are smaller and typically not population-based, but across these studies the data are consistent. In an interesting study63 involving identical twins discordant for obesity (the average difference in body weight between twin pairs was 18 kg), levels of TNF-α and soluble TNF-αreceptor 2 (sTNFR2) were higher in obese than in lean twins, which suggests that obesity rather than other genetic factors is a major determinant of these inflammatory markers.
Lastly, there is some evidence from observational studies involving both men and women that, in addition to total body fat, visceral (abdominal) body fat may be an independent predictor of inflammatory markers.37,38,43,44,64,77,78 In 2 studies77,78 the amount of visceral fat was a better determinant of CRP levels than other measures of obesity, including fat mass. The location of body fat, independent of total amount, is therefore an important factor affecting chronic inflammation.
Adipose tissue is known to be a secretory organ producing cytokines, acute-phase reactants and other circulating factors.79,80,81 The source of these “adipokines” is likely not the adipocyte itself, but the infiltration of inflammatory cells (macrophages) into adipose tissue.82,83 In vivo release of IL-6 and TNF-soluble receptors from subcutaneous abdominal adipose tissue has been shown to correlate with BMI and body-fat proportion.84 Moreover, TNF-α gene and protein expression in both subcutaneous and visceral adipose tissue are greater in obese than in lean people.85,86 In one in-vitro study87 TNF-α release from abdominal subcutaneous adipose tissue was 7.5-fold higher in tissue from obese (BMI 30– 40 kg /m2) than lean (BMI > 25 kg / m2) subjects.87 Ouchi and associates81 reported not only that CRP is expressed in adipose tissue, but also that CRP and adiponectin mRNA levels are highly inversely related. (Adiponectin is a protein with anti-inflammatory properties.)
Thus, both in vivo and in vitro studies confirm that adipose tissue expression and release of cytokines are elevated in people with a higher adipose mass.
Evidence from intervention studies
The hypothesis that an expanded adipose-tissue mass contributes to an elevated state of chronic inflammation is corroborated by data (summarized in Table 1) showing that weight loss reduces inflammation. Several markers of inflammation, including CRP, IL-6, IL-18, TNF-α and TNF-α receptors, are reduced after weight loss achieved through short-term intense dietary restriction,53,88,89,90,91 longer-term behavioural changes involving reduced energy intake and increased physical activity,42,43,54,58,62,92,93,94 approved medication use95 or surgical gastric bypass.57,64 Results for liposuction are contradictory: Although one such study99 resulting in a mean weight loss of 3 kg found concentrations of IL-6, IL-18, TNF-α and CRP to be reduced after a 6-month period of weight stability, another96 in which fat mass was reduced by 9.8 kg on average found IL- 6, TNF-α and CRP concentrations to be unaltered 10–12 weeks after the surgery. The effects of weight loss through liposuction for reducing inflammation thus require further investigation.
Table 1.
Most of the dietary weight-loss studies showed the magnitude of decrease in inflammatory markers to be linearly related to the amount of weight lost. For example, when CRP concentrations were reduced from 3.1 mg/L (standard deviation [SD] 0.7 mg/L) to 1.6 (SD 0.8) mg/L in postmenopausal women who followed a 14-month individualized weight-loss program,42 the reductions correlated with changes in body weight and fat mass. Decreases in CRP, IL-6, IL-18 and TNF-α in a group of premenopausal women after a 10% weight reduction correlated with changes in BMI but were more strongly related to changes in waist–hip ratio.43,58 Those women were healthy, without diabetes or metabolic syndrome, and their mean reduction in CRP (from 3.4 [SD 0.7] to 1.9 [SD 0.2] mg/L) mimicked the mean reported in healthy women by Tchernof and coauthors.42 In other studies, weight loss reduced CRP levels (from 5.0 [SD 0.5] to 4.3 [SD 0.5] mg/L) in women with metabolic syndrome,91 and IL-6 concentrations (2.75 [SD 1.51] to 2.3 [SD 0.91] pg/ mL) in women with insulin resistance.93
To date, only 2 randomized controlled trials56,97 have examined the effects of dietary weight loss on inflammation. Esposito and coworkers56 compared obese women enrolled in a behavioural counselling program designed to achieve a 10% weight reduction through monthly individualized advice on eating a low-energy Mediterranean-style diet and increasing physical activity with obese women in a control group who received no dietary advice. The 2-year intervention decreased BMI more in the women in the intervention group than in the control group (–5.2 v. –1.0 kg / m2) and reduced serum concentrations of CRP, IL-6 and IL-18 to a greater degree as well. In the intervention group, the average CRP value decreased from 3.2 to 2.1 mg/L, and the changes in CRP, IL-6 and IL-18 were found to relate to changes in BMI. Because exercise was included in the behavioural weight-loss intervention tested in this study,56 it is not possible to separate out the effects of the diet alone in producing these changes.
In a retrospective analysis of stored serum samples from a randomized clinical trial,97 our earlier research team found that an 18-month diet-induced weight loss program resulted in significantly greater reductions in body weight (–5.1% v. –1.8%) and CRP, IL-6 and sTNFR1 concentrations than no weight-loss intervention in a control group of older, obese men and women with knee osteoarthritis (Fig. 2). Changes in sTNFR1, but not CRP and IL-6, correlated with changes in body weight. Although some of the participants randomly assigned to the weight-loss intervention were also randomly assigned to an exercise intervention, no interaction was found between weight loss and exercise training.97
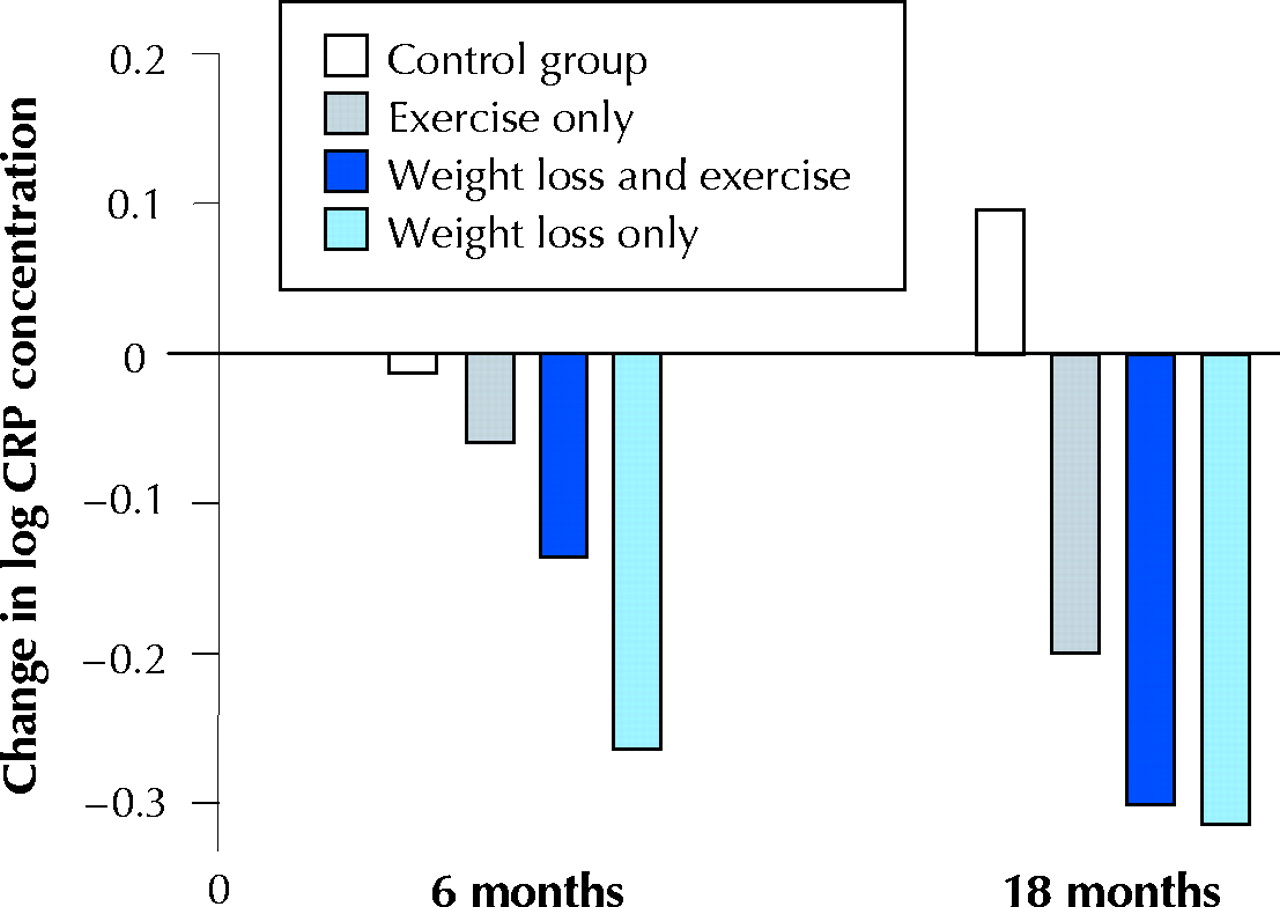
Fig. 2: Effects of 18 months of weight loss, exercise, or both upon mean CRP concentrations, adjusted for baseline BMI, baseline CRP level, sex and race. The treatment effect of dietary weight loss was significant compared with the control and exercise-only groups (p = 0.01). Modified from Nicklas et al (Am J Clin Nutr 2004;79:544-51), with permission.
In that prior study,97 the decrease in CRP concentrations in people who underwent diet-induced weight loss was 1.54 mg/L on average, or 5.8%. In other studies, CRP values decreased 26% with a 10% weight loss89 and fell 32%– 34% with a 15%–16% weight loss.42,56 These results suggest that there may be a dose–response effect between the degree of weight loss and its capacity to attenuate chronic inflammation. Unfortunately, no data are available on clinical manifestations of this decline in CRP concentrations, although a CRP reduction of about 15% after 1 year of statin use was shown to be associated with a lowered risk of coronary events.98 Longitudinal studies are needed to determine whether a reduced incidence of cardiovascular disease and diabetes is associated with the decline in CRP concentrations seen with weight loss.
Mechanism of effect
One of the postulated mechanisms by which weight loss reduces circulating markers of inflammation is through a decrease in adipose-tissue cytokine production (Fig. 3). A handful of studies have investigated the effects of dietary weight loss on cytokine gene and protein expression in subcutaneous adipose tissue; most data indicate that local production of IL-6 and TNF-α is reduced upon weight loss. Recently, gene-expression profiling showed that pro-inflammatory genes were downregulated and anti-inflammatory genes upregulated in subcutaneous adipose tissue after 28 days on a very-low-energy diet that resulted in a 6-kg loss of fat mass.73 In another study involving obese women,53 3 weeks on a very-low-energy diet (3.9 GJ/d, 5% drop in BMI) reduced IL-6 protein content in subcutaneous abdominal adipose tissue by 22%, with a corresponding 15% decrease in circulating levels. Interestingly, moderate dietary restriction (a deficit of 2.5 GJ/d for 10 weeks, for a 7.5% weight loss) reduced IL-6 mRNA in abdominal adipose tissue by 35% and its secretion rate by 30%, but decreased circulating IL-6 levels by only 6%.100Moreover, weight loss through caloric restriction reduced TNF-α gene87,101,102 and protein expression87 in, and TNF-α release from, abdominal adipose tissue.102

Fig. 3: Schematic of possible mechanisms by which weight loss and exercise training reduce sources of inflammation that lead to chronic activation of a pro-inflammatory state. Weight loss and increased activity affect the immune system by reducing the number of mononuclear cells in the peripheral blood, which are a source of pro-inflammatory cytokines (such as interleukins IL-6, IL-1β and IL-8; tumour necrosis factor-α and its receptors TNFR1 and TNFR2; and transforming growth factor TGFβ). A reduction in adipose tissue would not only reduce the volume of adipocytes and pre-adipocytes, but also decrease the number of endothelial cells and macrophages that reside there. These cells produce many pro-inflammatory mediators such as C-reactive protein (CRP), serum amyloid protein A (SAA) and cytokines. Weight loss and exercise may also increase the expression of anti-inflammatory mediators such as IL-10 and IL-1 receptor antagonist (IL-1ra) in these cells. The resulting circulatory changes could, in turn, cause the liver to contribute by decreasing its production of fibrinogen and other pro-inflammatory mediators. Photo: Lianne Friesen and Nicholas Woolridge
The effects of weight loss on adipose-tissue expression or secretion of CRP81 are still unreported. More studies are needed to determine whether reductions in adipose-tissue production of inflammatory biomarkers is one mechanism by which weight loss reduces overall chronic inflammation.
Role of physical activity and fitness in regulation of inflammation
Evidence from observational studies
Although acute bouts of exercise are well known to increase concentrations of pro-inflammatory cytokines and acute-phase reactants,103 chronic (regular, long-term) physical training may reduce basal concentrations of inflammatory markers. Table 2 summarizes the data from cross-sectional observational studies, which show an inverse association between markers of systemic inflammation and physical activity and fitness status.50,104,105,106,107,108,109,110,111,112 Several studies of large population cohorts, including the British Regional Heart Study,106 the Third National Health and Nutrition Examination Survey,108,111 the Cardiovascular Health Study,105 the men's Health Professionals Follow-up Study,109 the Nurses' Health Study II109 and the Health, Aging and Body Composition Study (Health ABC),50 provide evidence for an inverse, independent dose–response relation between plasma CRP concentration and level of physical activity in both men and women.
Table 2.
This relation does not seem to alter with age: Of the 5888 participants in the Cardiovascular Health Study,105 those older and younger than 72 years showed similar associations; and among people 70–79 years old enrolled in Health ABC,50 trends for decreased IL-6, TNF-α and CRP concentrations were linear with increasing amounts of reported exercise. In the British Regional Heart Study,106 even moderate physical activity (i.e., some vigorous activity at least once per week) in middle-aged men was associated with a 37% reduction in the number who had a high CRP concentration (> 4.27 mg/L). The relation was similar in men with and without prior heart disease.106 A dose-response relation between CRP level and exercise was also seen at baseline in men, but not women, enrolled in the Pravastatin Inflammation/CRP Evaluation Study,112 a finding that perhaps was confounded by the fact that the women were less likely than the men to be physically active.
In all of the studies described, the relations between inflammatory markers and physical activity were independent of differential levels of obesity. Contrary reports109,113 do exist, but their results may reflect chance findings owing to their small samples.
Although CRP is the marker of chronic inflammation most frequently studied, both IL-6 and CRP concentrations have been shown in elderly men to be inversely correlated to reported amounts of moderate and strenuous exercise, even after adjustment for BMI.104,109 Similar studies have shown this to be true for recreational activity and house and yard work110,114 (although not consistently for IL-6110).
All of the studies mentioned relied on self-report to assess physical activity status. In a subsample of 722 men from the Aerobics Center Longitudinal Study, Church and collaborators107 reported that plasma CRP is also inversely related, in a dose–response manner, to cardiorespiratory fitness measured directly on a treadmill. The odds ratio of men in the lowest quintile of fitness for having a high CRP concentration (> 1.84 mg/L) was 3.2 (95% CI 1.8–5.8), compared with men having higher fitness levels. Study investigators measured adiposity directly from the sum of skinfolds. Additional adjustments for body fat percentage and waist circumference did not alter the relation between CRP and cardiorespiratory fitness.107
Overall, data from observational studies show that the greater the volume of physical activity, the lower the risk of elevated levels of chronic inflammatory markers. Primarily, the relation between inflammation and physical activity is independent of obesity as measured by BMI. But since BMI is not a direct measure of body fat, the question remains, after adjustment for differences in total and abdominal adiposity, as to whether inflammation is associated with physical activity.
Evidence from intervention studies
Although no data from prospective randomized controlled trials exist to date to definitely conclude that long-term regular exercise training reduces chronic inflammation, several uncontrolled studies of exercise do show an effect on specific inflammatory markers. For instance, in patients with chronic heart failure, 12 weeks of aerobic exercise reduced TNF-α concentrations,115 6 weeks of cycle ergometry reduced sTNFR2 concentrations,116 and 16 weeks of combined aerobic and resistance exercise training decreased levels of both TNF receptors (but not TNF-α itself).117 In addition, exercise training for patients with intermittent claudication reduced CRP after 3 months.118 CRP decreased after 9 months of training for a marathon in 10 of 12 male runners.119 In overweight women, aerobic exercise training for 5 months decreased serum concentrations of TNF-α, sTNFR1 and sTNFR2,120 and cycle ergometry for 12 weeks reduced TNF-α and sTNFR2 (but not sTNFR1) concentrations.121 Moreover, levels of acute-phase reactants CRP and serum amyloid protein A (but not IL-6) decreased significantly in 20 postmenopausal women who completed a 14-day diet and aerobic exercise intervention as inpatients.122 The magnitude of the CRP decrease (45%) in these women was not significantly related to the magnitude of weight loss (4%). In another study,123 resistance exercise training decreased TNF-α (both mRNA and protein levels) in skeletal muscle of frail, elderly subjects, which suggests that resistance training is also a potential treatment for chronic inflammation.
All of these studies had a small number of participants, were conducted in populations with elevated inflammatory markers (i.e., patients with congestive heart failure or obesity) and had relatively short durations. One of the larger studies124 to date, which incorporated a control group but did not randomly assign participants to groups, demonstrated that a phase II cardiac rehabilitation and exercise training program reduced median CRP concentrations by 41% (mean change from 5.9 [SD 7.7] mg/L to 3.8 [SD 5.8] mg/L; median change from 3.4 to 2.0 mg/L) in 235 patients with coronary artery disease, but CRP concentrations did not change in 42 who did not exercise (Fig. 4). Exercise training seemed to be more effective in those with the highest CRP concentrations; for example, the proportion of patients with a CRP value above 15 mg/L decreased from 9% to 1%. Stratification of the data according to use of statin therapy did not alter the results. Changes in CRP concentrations were unassociated with changes in body weight or percent body fat, which provided compelling evidence that the exercise training effect was independent of body fat loss.124 Another earlier research team of ours125 also found evidence for an independent effect of exercise training in postmenopausal women who underwent 6 months of dietary weight loss alone or in combination with aerobic exercise training. In this study, decreases in IL-6, sIL-6R and sTNFR1 differed significantly between the groups, with changes in sIL-6R and sTNFR1 concentrations inversely related to changes in aerobic fitness.125 Another interesting study126 was conducted specifically to determine the effects of a 6-month supervised, individualized aerobic exercise training program on the production of cytokines by mononuclear cells in men and women at high risk of ischemic heart disease. In the 43 people who completed the program, overall production of atherogenic cytokines (interferon γ, TNF-α and IL-1α) decreased by 58%, and the production of atheroprotective cytokines (IL-10, IL-4 and transforming growth factor TGFβ1) increased 36%. (Their mean CRP level was 35% lower after exercise training, but the difference was not statistically significant.126)

Fig. 4: Median changes in high-sensitivity (HS) C-reactive protein concentrations in patients with coronary heart disease after 19 weeks of follow-up (standard deviation 3 weeks) in cardiac rehabilitation compared with control patients with coronary artery disease. Reprinted with permission from Milani et al (J Am Coll Cardiol 2004;43:1056–61).
Only a few randomized controlled trials have been published that report the effects of an exercise intervention on inflammatory markers, and the data are conflicting. During a 6-year trial involving 140 middle-aged Finnish men,127 CRP concentrations remained consistantly lower in the aerobic exercise group than in the control group, but the trend was not statistically significant (p > 0.20). In the weight loss and exercise trial97 already described, our team also did not find an 18-month combined resistive and aerobic exercise training program to have a statistically significant effect on inflammatory biomarkers, although mean CRP values at follow-up visits tended to be lower in the intervention group than in the control group at both 6 and 18 months. Smaller studies118,128 of shorter duration also hint that exercise training reduces inflammation compared with no exercise. In men with metabolic syndrome, 3 months of aerobic exercise decreased concentrations of monocyte chemoattractant protein-1 by 33% and IL-8 by 13%.128 Although CRP levels in patients with intermittent claudication were significantly reduced after 3 months of a 12-month exercise training program compared with levels in control subjects,118 CRP concentrations increased to baseline levels at the 6- and 12-month follow-up visits, perhaps because exercise in this study was unsupervised after the first 3 months. Interestingly, Gielen and associates129 reported that exercise training did not reduce serum inflammatory markers in male patients with congestive heart failure but did reduce TNF-α, IL-6 and IL-1β gene expression in local skeletal muscle, relative to a control group. This suggests that exercise may elicit local anti-inflammatory effects that may or may not be evident in the systemic circulation.129
Additional data derived from randomized controlled studies are needed to provide definitive evidence that exercise training should be used as a treatment for chronic inflammation.
Summary
Persistent low-grade inflammation is emerging as an important contributor to the pathophysiology of several chronic diseases. Given the widespread deleterious health effects of an augmented inflammatory state, identification of therapies that reduce inflammation is critical. Yet, to date, there is little definitive evidence for therapies that can be used effectively to treat elevated markers of inflammation that are within the clinically normal range. As reviewed here, there are promising data suggesting that decreasing energy intake and increasing physical activity could be effective for reducing overall inflammation. But at present, data from randomized controlled trials conducted to determine the effects of weight loss or exercise training, or both, on inflammation are lacking. The mechanisms by which weight loss and increased physical activity reduce inflammation have yet to be elucidated.
Although weight loss is likely to emerge as an effective treatment for reducing inflammation, the magnitude of the effect and the weight loss needed to produce clinically meaningful results require delineation. On the other hand, the effects of exercise training in the absence of weight loss are unclear. Large-scale prospective studies are needed to definitively determine whether aerobic or resistive exercise training, or both, are effective in reducing inflammation.
Footnotes
-
This article has been peer reviewed.
Contributors: All of the authors made substantial contributions to the writing of the paper, including comprehensive review of the literature, interpretation of findings and drafting of the text and figures.
Acknowledgements: This work was supported in part by the Wake Forest University Claude D. Pepper Older Americans Independence Center (National Institute on Aging [NIA] grant P30-AG-021332) and NIA grant R01-AG/DK-20583.
Competing interests: None declared.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- The role of gp130 receptor cytokines in the regulation of metabolic homeostasis
- Effect of Exercise on Markers of Inflammation in Breast Cancer Survivors: The Yale Exercise and Survivorship Study
- Inflammatory Markers and Risk of Type 2 Diabetes: A systematic review and meta-analysis
- Inflammatory Marker Changes in a Yearlong Randomized Exercise Intervention Trial among Postmenopausal Women
- A 1-Year Lifestyle Intervention for Weight Loss in Individuals With Type 2 Diabetes Reduces High C-Reactive Protein Levels and Identifies Metabolic Predictors of Change: From the Look AHEAD (Action for Health in Diabetes) study
- Sex-specific effect of body weight gain on systemic inflammation in subjects with COPD: results from the SAPALDIA cohort study 2
- Physical Activity and Postmenopausal Breast Cancer: Proposed Biologic Mechanisms and Areas for Future Research
- Modulation of C-Reactive Protein, Tumor Necrosis Factor-{alpha}, and Adiponectin by Diet, Exercise, and Weight Loss
- C-Reactive Protein as a Predictor of Incident Ischemic Stroke Among Patients With Preexisting Cardiovascular Disease
- Health benefits of physical activity: the evidence.
- Other advantages to aerobic exercise
More in this TOC Section
Similar Articles
Collections

