


- © 2005 CMA Media Inc. or its licensors
A 57-year-old man noticed a painless bluish mass enlarging on top of his right foot. Fine-needle aspiration and excisional biopsy showed a high-grade giant-cell variant of malignant fibrous histiocytoma. Because he had recurrence of the tumour at the initial excision site within 2 months, the patient opted for below-knee amputation without adjuvant radiation therapy. The surgical resection margins were free of tumour cells.
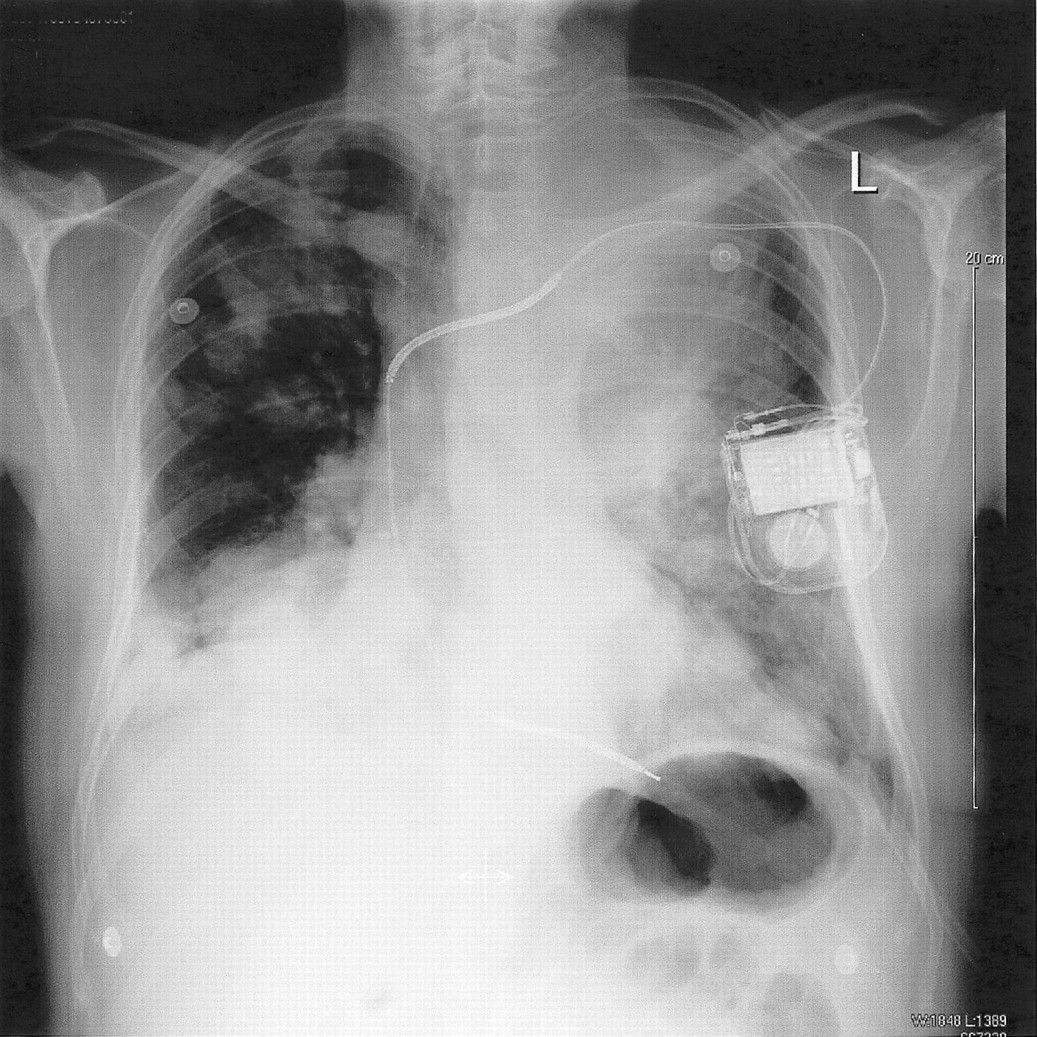
Unfortunately, the patient had increasing shortness of breath on exertion within 4 months after amputation. A chest CT showed bilateral pulmonary nodules consistent with metastases. He was admitted to hospital 5 months after the onset of shortness of breath for anthracycline-based chemotherapy. However, his left ventricular ejection fraction decreased, and therapy was switched to an ifosfamide-based regimen. Despite this, serial imaging showed enlarging nodules in the lung (Fig. 1 and Fig. 2), and hemoptysis developed 16 months after the start of chemotherapy. Along with bright red blood, the patient coughed up solid masses up to 5 cm in length (Fig. 3). Biopsy of the expectorated masses confirmed the radiologic diagnosis of metastatic malignant fibrous histiocytoma to the lung. The patient died in hospital within 2 months after the onset of hemoptysis.


Malignant fibrous histiocytoma is the most common soft-tissue sarcoma in adults,1 occurring most often in the lower extremities. The tumour contains both histiocyte and fibroblast-like cells. There are many histologic subtypes, around which there are controversies in the literature. Variants include fibrous, giant-cell, myxoid and inflammatory.2 The lung is the most common site of distant metastasis. Conservation surgery striving for negative margins along with adjuvant radiation therapy is the treatment of choice for local disease.1 Distant metastasis, larger primary tumour (> 5 cm) and high-grade tumour are all negative prognostic factors.3
Originally described by Mackenzie in 1886,4 expectoration of large fragments of lung tumour is rare.5 It has been described in cases of endobronchial primary lung cancer and metastases from renal cell and colon carcinomas, osteogenic sarcoma and malignant melanomas.5 More recently in the era of AIDS, coughing up sections of tumour has been seen in patients with Kaposi's sarcoma and lymphoma.6 Spontaneous expectoration of metastatic malignant fibrous histiocytoma is exceptionally rare.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

