


- © 2004 Canadian Medical Association or its licensors
Long waiting lists for cardiac surgery are a problem for national health care systems,1 and deaths among those waiting to be treated are a special cause for concern.2,3 Priority is usually given to patients who are at above-average risk of dying.4 The impact of such a policy can be illustrated by a simple compartment model (Fig. 1).
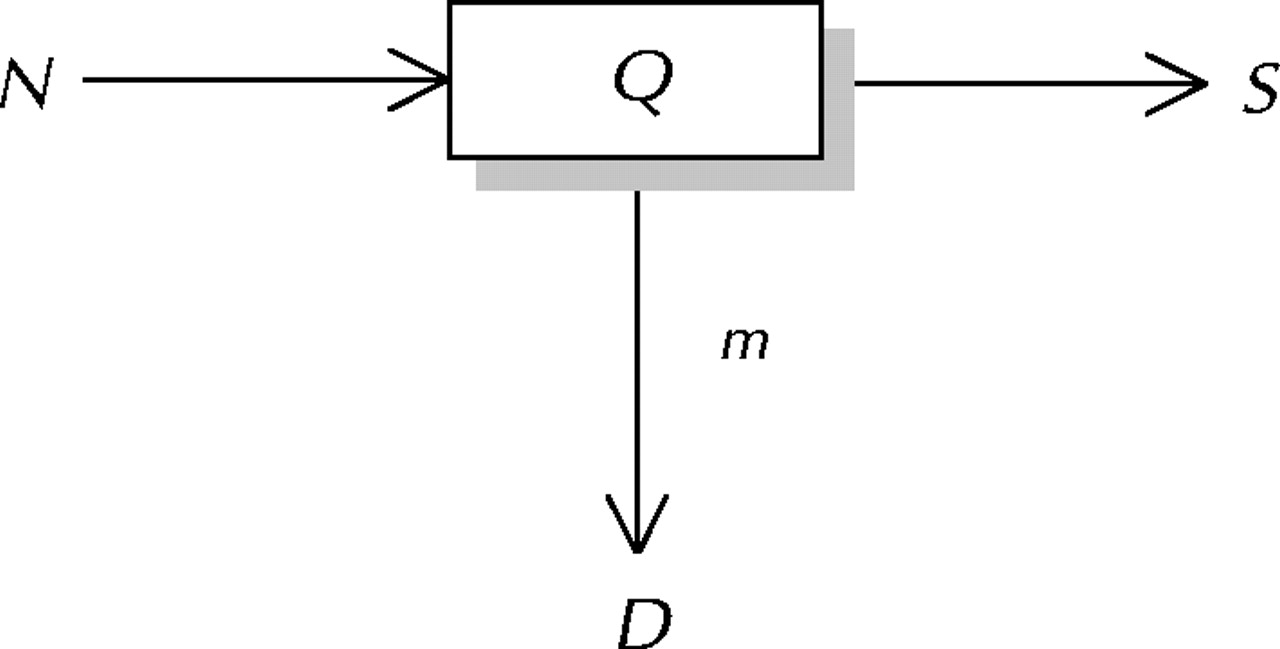
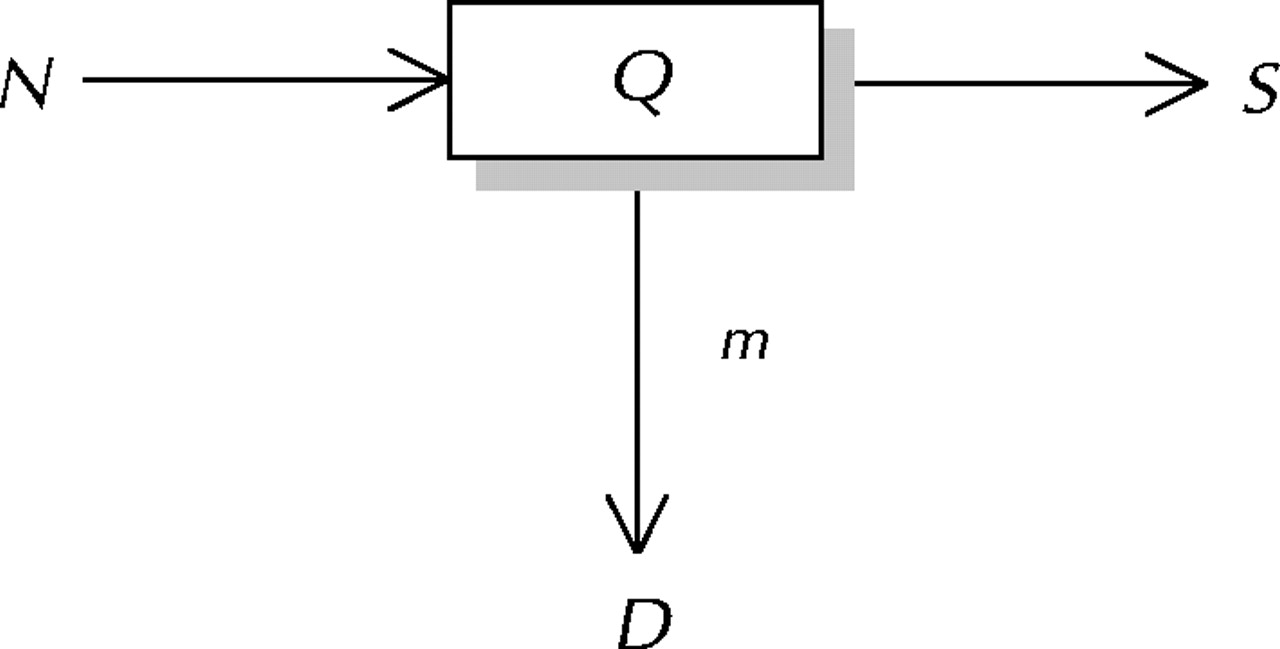
Fig. 1: A compartment model of a waiting list. N = the number of patients accepted for surgery each year, Q = the number waiting for surgery at any given time, S = the number who undergo surgery each year, m = the death rate per person-year among those waiting for surgery, D = the number of deaths each year among those awaiting surgery.
Suppose that N patients per year are added to the waiting list and S patients (some number less than N) are treated each year. If N and S are constant, and patients remain on the waiting list until they are treated or die, then a waiting list of size Q will result. Among patients on the waiting list, there will be D = mQ deaths per year, where m is the death rate per patient-year. In this steady state (where inflow = outflow) N = S + D, D = mQ, and Q = (N – S)/m. T, the average waiting time before death or surgery, is Q/N.
For example, if N = 1000 patients per year, S = 960 patients per year, and m = 0.1 deaths per patient-year, then Q = (1000 – 960)/0.1 = 400 patients, D = 0.1 х 400 = 40 deaths, and T = 400/1000 = 0.4 years or 146 days. From these calculations we can see that even a small difference between the number accepted for treatment and the number treated with available resources will result in a sizeable waiting list, since in calculating the size of the waiting list, the difference between N and S is multiplied by the reciprocal of m, a small number.
This model can be applied to any waiting list scenario that is in a steady state. Such steady states would occur in any large health care system in which the value for N – S is constant.
Suppose now that the 1000 patients accepted each year for surgery comprise 2 groups: N1 = 300 per year with mortality rate m1 = 0.24, and N2 = 700 per year with mortality rate m2 = 0.04. The degree of priority given to one or the other of these 2 groups is determined by the allocation of the total available treatments, S per year, to each group, say S1 and S2 (such that S1 + S2 = S). If complete priority is given to the high-risk group, then all 300 high-risk patients will be treated, leaving 960 – 300 = 660 treatments for the low-risk group. Conversely, if complete priority is given to the low-risk group, then all 700 low-risk patients will be treated, leaving 960 – 700 = 260 treatments for the high-risk group. If no priority is given to either group (i.e., S1/S2 = N1/N2), then S1 = 288 and S2 = 672.
Table 1 shows the effect of these 3 scenarios on the number of deaths per year, the size of the eventual waiting list and the mean waiting time for each risk group and for the patient group as a whole. Giving priority to the high-risk group yields a larger overall waiting list and a longer mean waiting time, although the total number of deaths per year is the same as under the other scenarios. The latter must be so, since N1 – S1 + N2 – S2 = N1 + N2 – (S1 + S2) = N – S, which is constant.
Table 1.
Thus, the natural clinical tendency to give priority to the group with a higher mortality rate does not yield fewer deaths among patients on the waiting list and leads to a larger overall waiting list. To reduce the size of the waiting list by giving priority to the group with lower mortality rate (see Table 1) would probably be considered cynical and unethical, but it should be noted that such a policy would not increase the overall number of deaths per year.
It can also be shown that these results hold where there are more than 2 risk groups.
This analysis is not intended to be normative or to constitute a recommendation that priorities for surgery be changed. However, there is anecdotal evidence that in Ontario “some access to specialized cardiovascular services occurs preferentially on the basis of facts other than clinical needs.”5 Although rightly considered deplorable, such behaviour would not, according to the model, increase the number of deaths on the waiting list.
𝛃 See related article page 357
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

