


Abstract
WE REPORT THE CASE OF A 50-year-old man who reported sudden, painless loss of vision in his left eye after starting antihypertensive therapy. Potential causes of acute painless unilateral visual loss are discussed, as is the initial management of hypertension in asymptomatic patients.
Case
A 50-year-old man came to the emergency department with a 36-hour history of painless decreased vision in his left eye. He had seen his family doctor 3 days earlier to report dizziness and had been found to have a blood pressure of 195/130 mm Hg. At that time, his doctor had prescribed fosinopril (20 mg/d) and hydrochlorothiazide (25 mg/d). On waking the next morning, the patient had noted loss of vision in his left eye, with no pain. When his vision had not improved a day later, he went to the emergency department.
The patient denied experiencing fever, headache, nausea, vomiting, scalp tenderness or jaw claudication. He had no significant medical history and was not taking any medications other than the 2 prescribed for his hypertension. His family history was negative for cardiac disease, diabetes mellitus and eye problems.
Examination showed the patient to be afebrile with a blood pressure of 161/85 mm Hg. Visual acuity was 20/20 (metric 6/6) in the right eye; with the left eye he could detect only hand movements. An afferent pupillary defect was noted in the left eye. The right eye appeared normal on fundus examination; however, a pale, edematous retina was noted in the left eye, with a characteristic cherry-red spot (Fig. 1). There was no evidence of retinal emboli in either eye. The patient had a normal complete blood cell count and a normal erythrocyte sedimentation rate (1 mm/h). An ophthalmologist was consulted. Based on the duration of the patient's visual loss, the opinion was that any therapeutic intervention would be unlikely to improve vision.

Fig. 1: Left: Normal appearance of right eye on funduscopic examination. Right: Cherry-red spot in left eye with extensive retinal edema and pallor secondary to retinal artery occlusion. The foveal region appears cherry red because the surrounding retina is edematous and appears white, thereby accentuating the normal red foveal reflex coming from the choroidal circulation. Choroidal circulation is usually unaffected in central retinal artery occlusion.
The patient was re-examined the following morning, at which time his blood pressure was 113/90 mm Hg. An angiogram showed a normal right eye and delayed arterial filling in the left eye consistent with a central retinal artery occlusion (Fig. 2). The Doppler scan showed small plaques in the left and right common carotid arteries, with a 16%–49% stenosis of the left proximal common carotid artery, but there were no significant hemodynamic abnormalities in either the carotid or vertebral circulation.
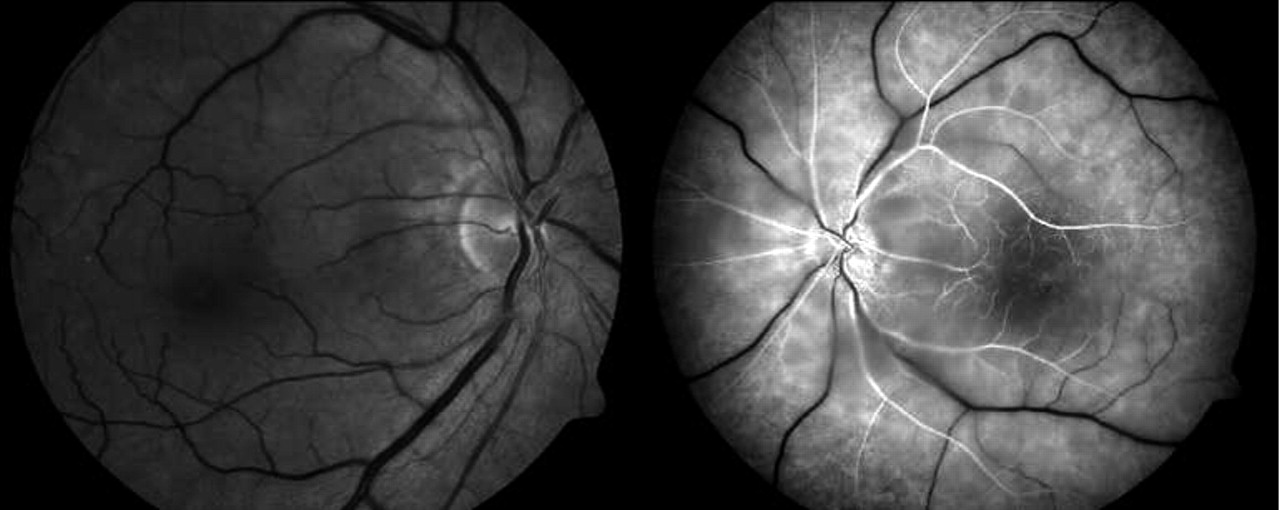
Fig. 2: Fluorescein angiograms, taken several minutes after infusion of contrast medium. Left: The vasculature of normal right eye demonstrated early filling and passage of dye. Right: The left eye showed markedly delayed passage of fluorescein, with filling of its arterial tree beginning several minutes after the infusion.
During follow-up visits with his family doctor, the patient's blood pressure was found to vary between 170/110 and 130/84 mm Hg after the addition of nifedipine. At a follow-up visit 14 months after the initial event, vision in his left eye had improved slightly, such that he was able to count fingers.
Comments
Vascular insufficiency is the most common cause of sudden painless unilateral loss of vision (Table 1).1,2,3 Retinal ischemia can result from direct occlusion of the central retinal artery by an embolism from the left atrium or carotid arteries.4,5 The resulting ischemia may be either transient (amaurosis fugax) or persistent (central retinal artery occlusion). Inflammatory conditions (e.g., giant cell arteritis) are a significant preventable cause of visual loss.6 Acute-onset visual loss resulting from systemic hypotension has been reported previously.7,8,9
Table 1.
Acute-onset visual loss requires urgent ophthalmologic consultation.10 Treatment needs to be started within 4 hours after onset for any chance of restoring normal vision.11 If treatment is delayed for more than 24 hours, significant improvement in visual acuity is highly unlikely. Therapeutic options for central retinal artery occlusion are aimed at either reducing intraocular pressure (through ocular massage, anterior chamber paracentesis or acetazolamide therapy) or attempting to dislodge or reduce the embolus (through localized thrombolysis or ocular massage).11 In our patient's case, the use of any of these therapies would have had little effect on his clinical outcome, because he had experienced visual loss for 36 hours at the time of presentation.
Chronic hypertension can induce hypertrophy of the tunica muscularis of the arterial wall, causing narrowing of the lumen and an increase in peripheral vascular resistance.12 As a result of these changes, a rapid drop in systemic blood pressure may compromise cerebral perfusion and lead to ischemia and injury in susceptible tissue, such as the retina.
In patients such as ours, who are less than 60 years old with uncomplicated hypertension, initial treatment should consist of a trial of monotherapy with a thiazide diuretic, β-blocker or angiotensin-converting-enzyme (ACE) inhibitor.13 Combination therapy should be attempted only if adequate blood pressure control is not achieved with monotherapy. The supplier's product monograph for Monopril (fosinopril) specifically warns of the danger that “patients concomitantly taking ACE inhibitors and diuretics, and especially those in whom diuretic therapy was recently instituted, may occasionally experience an excessive reduction in blood pressure after initiation of therapy.”14 During the initial studies of fosinopril in placebo-controlled heart-failure trials, 0.8% of patients were reported to have discontinued treatment as a result of first-dose hypotension.14,15
Before experiencing his visual loss, our patient had gone to his family physician because of dizziness, but he was otherwise asymptomatic. He had been prescribed combined therapy with fosinopril, at twice the recommended starting dose,14 and hydrochlorothiazide. Although his loss of vision may have resulted solely from a thromboembolic event arising from a ruptured atheromatous plaque, this seems unlikely given his age and lack of prior visual or neurological symptoms. Rather, the rapid reduction in his systemic blood pressure was likely the primary cause, and the stenosis of his proximal left common carotid artery contributed secondarily.
In summary, hypertension is a chronic medical condition to which the body responds with vascular remodelling to maintain the requisite tissue perfusion and oxygen delivery for normal physiological functioning. In the absence of manifestations of hypertensive encephalopathy (severe headache, vomiting, visual field disturbances, transient paralyses, convulsions, stupor or coma) or clinical findings suggesting pathological changes resulting from elevated blood pressure (papilledema, retinal hemorrhages and exudates), a conservative approach should be taken toward normalizing blood pressure. Sudden reduction of blood pressure through the administration of multiple antihypertensive medications may result in hypoperfusion and ischemic injury to susceptible tissues.
Footnotes
-
This article has been peer reviewed.
Contributors: Both authors contributed to the drafting of the article and its critical revision and approved the version to be published.
Competing Interests: None declared.
In this issue
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

