


Abstract
Background: Effective patient–physician communication requires the use of words that are clearly understood by both parties. We conducted this study to compile a list of words used by children and caregivers to describe “private” anatomical structures and physiological functions, to document the frequency of such usage and to examine the relation between correct word usage and caregiver's level of education.
Methods: In a large urban pediatric emergency department, a convenience sample of 156 children at least 3 years old were asked to name the body parts (penis, testes, vagina, buttocks, breasts) pointed to in 4 simple, explicit line drawings of an unclothed boy or girl, and to name the bodily functions (vomiting, defecation, urination) depicted in 3 drawings of children. Eighty-seven patients sufficiently fluent in English were included in the study. Their caregivers were asked separately what words they currently use with their child and with other adults for these body parts and functions and what words they remembered using as children.
Results: The children used a mean of 1.2 correct anatomical and physiological terms out of a possible 8 to describe the private parts and functions in the drawings. The mean number of correct words used by the caregivers was 2.3 when talking with their children, 3.6 when talking with their peers and 1.5 when they were children. There was no correlation between the caregiver's level of education and the frequency of correct word usage by their children. We identified slang words used by at least 5% of the respondents; however, some used the same slang words to refer to different body parts.
Interpretation: Given the variety of slang words used by children and their caregivers to describe private parts and functions, the meaning of the words should be clarified during history taking.
The use of words that can be clearly understood by both patient and clinician is essential to obtaining an adequate medical history1 and maintaining effective communication.2 This is especially important when communicating with children and their caregivers about “private” body parts and functions in situations with medicolegal implications, and with children and their families who often substitute personal code words for anatomically or physiologically correct terms. A list of these commonly used words would facilitate communication.3
Two previous studies compiled lists of words used by children and their caregivers; however, they did not report on the frequency of use or investigate the relation between correct word usage and education level of the caregivers.4,5 Because we could find no further relevant articles, and because we wished to assist health and legal professionals who interview and examine children and their caregivers, we undertook this study to (a) develop an inventory of terms used by children and their caregivers, from a wide range of ethnic origins, to describe “private” anatomical parts and physiological functions, (b) document the frequency of correct word usage and (c) correlate the frequency of correct word usage with the caregivers' educational backgrounds.
Methods
We selected a convenience sample of children and their caregivers presenting to the emergency department at the Hospital for Sick Children, Toronto, between January and May 1999. The hospital's emergency department serves an ethnically diverse population, with more than 50% of patients claiming a language other than English as their mother tongue. We excluded children who were less than 3 years old, those who were not accompanied by a primary caregiver (defined as the person looking after the child for most of his or her waking hours) and those who presented with an altered level of consciousness.
Written informed consent was obtained from the caregivers and oral consent from the children. Ethical approval for the study was obtained from the hospital's Research Ethics Board.
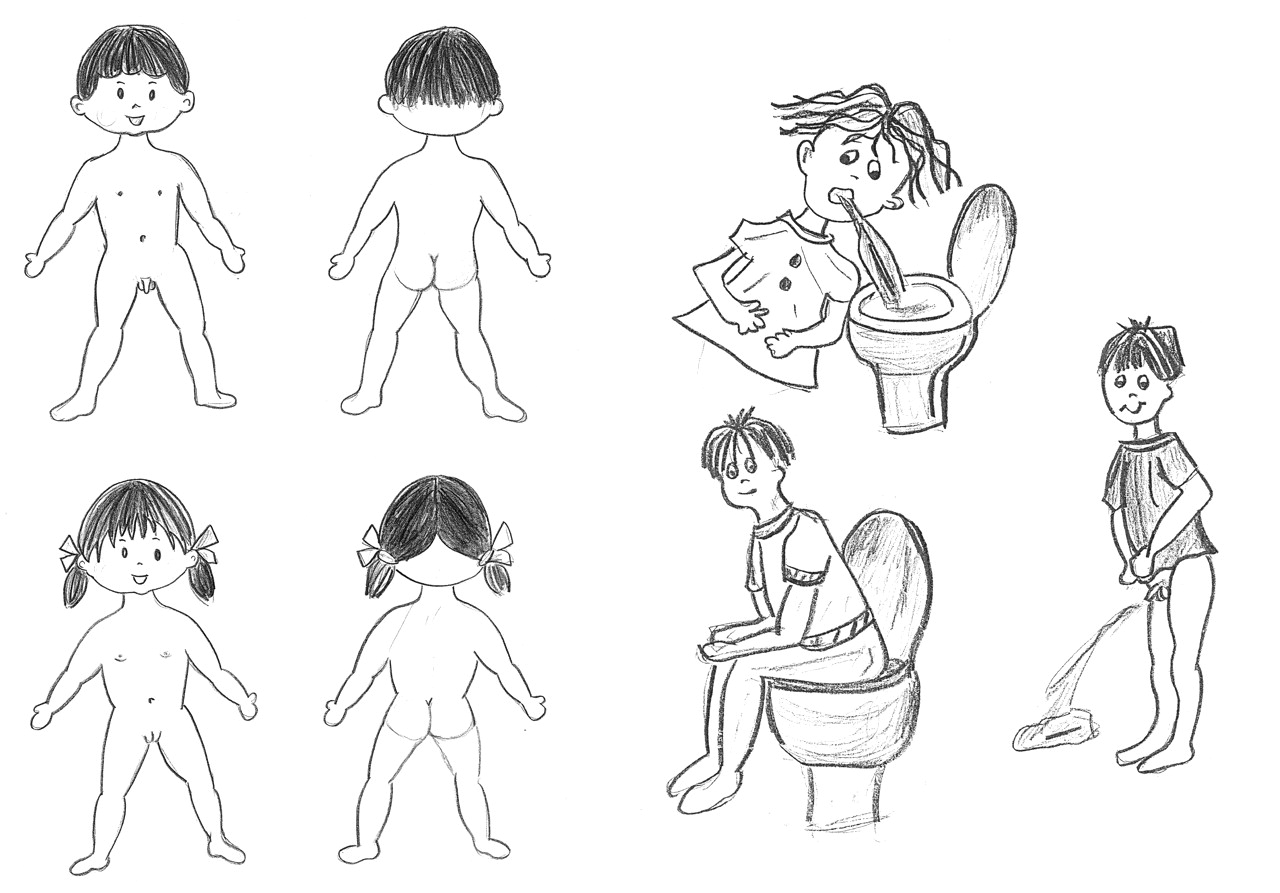
A trained interviewer conducted a structured interview with the children and their primary caregivers using a questionnaire based on 7 drawings, each depicting either an anatomical part (penis, testes, buttocks, vagina, breasts) or a physiological function (vomiting, defecation, urination) (Fig. 1). These items were chosen because the terms are frequently used clinically and are important to clinical practice. Each child was shown the drawings, which were of children close to their own age, and was asked “What is this?” or “What is this boy or girl doing?” Afterward the caregiver was asked what words he or she used with the child and with other adults as well as what words he or she remembered using as a child. Thus, a total of 4 words could be given for each of the 8 body parts and functions for each child–caregiver pair. Responses were recorded verbatim. The interviewer also recorded the level of education of the caregiver in each family who had the greatest number of years of education as well as the ages of the child and primary caregiver.

Fig. 1: The seven drawings used for questioning children and their caregivers about words they use to describe the anatomical parts and physiological functions depicted in the drawings. The complete list of words appears in Appendix 1. (It is acknowledged that the drawing of the girl shows her introitus or pudenda and does not actually anatomically represent the vagina.) Photo: Dr. Vida Farhangi
For our analysis, we classified the children into 3 age groups (3.0–4.9 years, 5.0–9.9 years and 10 years and older) and the caregivers' education levels into 4 groups (high school incomplete [less than 12.0 years of education], high school complete [12.0–13.5 years], college or undergraduate university education [13.6–17.5 years] and graduate education [more than 17.5 years]).
We used descriptive statistics to summarize demographic characteristics. We classified responses as anatomically correct or incorrect and calculated the number of correct terms. Spearman's correlation was used to compare the frequency of correct word usage between children and caregivers; the 𝛘2 test was used to determine whether the education level of the caregivers was associated with the number of correct words. Exploratory analyses were used to investigate the influence of the child's and caregiver's age and sex on the number of correct words used. A p value of less than 0.05 was considered significant.
Results
A total of 171 families participated in the study. None of the families approached refused to participate, and all but one completed the study questionnaire (one family withdrew from the study because the father cited embarrassment in articulating the words). We subsequently excluded 83 families from the statistical analysis because the child was less than 3 years old (considered unable to express himself or herself adequately) (n = 14) or because English was rarely or never spoken at home (n = 69). Thus, 87 families were included in the final statistical analysis. However, the words used by all of the children are included in Appendix 1.
The mean age of the 87 children included in the analysis was 6.0 (standard deviation 2.6; range 3–14) years; 31 were 3.0–4.9 years old, 48 were 5.0–9.9 years old, and 8 were 10 years or older. Forty-five (52%) of the children were girls. The mean age of the primary caregivers was 36.0 years; 96% were women. In 90% of the cases the primary caregiver was the parent.
Table 1 shows the words used, and their frequency of use, by at least 5% of the English-speaking children and their caregivers. The children used a mean of 1.2 correct words out of 8 possible terms to describe the private body parts and functions in the 7 drawings. The mean number of correct words used by the caregivers was 2.3 when talking with their children, 3.6 when talking with their peers and 1.5 when they were children. The caregivers were often unable to provide the word they had used as a child. None of the differences in rates of correct word usage between these 4 groups of data was statistically significant. Some children used “pee” to mean vagina, penis, testes and urination, and “bum” to mean testes, vagina and breast.
Table 1.
Table 2 shows the mean number of correct words used by children according to education level of their caregivers. We did not find a relation between the level of education and the number of correct words (𝛘2 = 19.5, p = 0.55). Graphical review of these data confirmed the lack of relation between these 2 factors; however, there was a weak threshold effect, in that children whose caregivers had not completed high school used fewer correct words (mean 0.67). Although there was no correlation between sex and correct word usage, child's age was strongly correlated (Spearman's rho = 0.216, p = 0.047), with older children using more correct words than younger children.
Table 2.
Interpretation
Strict adherence to the use of correct terminology could severely limit clear communication with children. Table 1 and Appendix 1 can be used to suggest the range of possible meanings of terms used by families. Appendix 1 provides a lexicon of terms that can be used when standard anatomical terms prove ineffective; many of the terms used by children whose mother tongue was not English may actually represent anatomically and physiologically correct terminology in another language. Although caregivers who have completed more years of education may be expected to use fewer incorrect words than caregivers with less education, we did not find this to be the case in our study. Caregivers were more likely to use correct words and irreverent words with their peers than with their children. Three words used by caregivers with their peers — “arse,” “tits” and “shit” — were not used by them with their children, which suggests that these words should be avoided in communicating with children.
Our findings supplement those of MacDonald and coauthors,4 who compiled a list of words used by a predominantly male group of children for only 4 private subjects and did not report the frequency of use or investigate the relation between word usage and caregivers' educational background. Several words in their study were similar to those used by our population: “bum” and “bottom” to mean buttocks or anus, and “balls” to mean testes. The only other word used in both studies was “privates” (by caregivers in our study and by children in their study). This lack of similarity may reflect differences in populations, since the other study was performed in the United Kingdom, but it may also indicate a shift in use of alternative slang words over time, since the other study was performed in 1985.
Our data also supplement those from Fraley and coauthors,5 who reported words for genitalia used by parents with their children (1–4 years of age). They correlated the level of parental education with sex education but not with correct word usage, as we have done.
The fact that many caregivers did not recall the words they used as children and that most of the children in the study had at least 1 word for each body part and function (Table 1) may reflect a more conservative approach to correct naming of body parts and functions in previous generations. It could also mean that the caregivers forgot the words they had used. Today's parents may be more willing to use the correct words for intimate and private physiological and anatomical terms. Although the primary caregivers in our study were encouraged to be forthcoming in mentioning words they used, they may have been constrained by “politeness” to give the interviewer untrue responses. Generalizability of our results may be limited by our use of a cohort sample and the relatively small number of children over 10 years old. However, Toronto, where we conducted the study, is one of the most cosmopolitan cities in the world and has the greatest density of recent immigrants in Canada.6 Thus, we believe our study population is representative of populations in many major North American cities.
In order to establish a child's general developmental level and ability before an interview or examination, an attempt should be made to determine the child's ability to name obvious body parts such as the hands, feet and nose. The meaning of words used by children and their parents in relation to private body parts and functions should be clarified before clinical decisions are made on the basis of the information. Thereafter, the use of a few additional slang terms could enhance communication with children and caregivers. Future studies need to investigate nuances of communication required for the wide range of ethnic, language and religious groups that often constitute the majority of patients in large health care facilities. Furthermore, major pediatric centres should consider compiling lists of slang words commonly used by their populations to facilitate accurate communication between health care providers and their patients.
Appendix 1
Appendix 1.
Footnotes
-
Contributors: Dennis Scolnik was responsible for the study conception, the collection and analysis of data, and the writing and editing of the manuscript. Victoria Atkinson participated in the ethics approval process and was responsible for gathering data along with Maha Hadi and Jon Caulfeild. Nancy Young was responsible for the data analysis. All of the authors approved the final version.
Acknowledgement: This paper was prepared with the able assistance of Diana Cristea, Senior Secretary, Division of Emergency Services, Hospital for Sick Children.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

