


Abstract
A YOUNG, HEALTHY MAN PRESENTED with sudden severe sensorineural hearing loss and tinnitus. The results of the workup and neuroimaging were normal, as were the auditory brain stem responses. Methylprednisolone pulse therapy was associated with significant hearing improvement within 10 days. A history of a short self-limited febrile illness preceding admission (with headache, photophobia, myalgia and fatigue), a raised serum C-reactive protein level and transient leukopenia suggested an infectious cause. Lumbar puncture revealed a mononuclear pleocytosis of the cerebrospinal fluid, with negative cultures but positive polymerase chain reaction test results for enterovirus, which was later cultured from the patient's stool. The patient's wife and baby had had a similar febrile illness without hearing loss 10 days earlier, and an outbreak of enterovirus meningitis was identified in the area, which was associated with familial clustering and echovirus serotype 4 infection. The varied causes of sudden sensorineural hearing loss, which should include enterovirus, are reviewed here.
Case
A healthy 27-year-old man was admitted to hospital in Israel in October 2001 with sudden severe bilateral hearing loss. Four days earlier, he had developed fatigue, myalgia and headache and then had a fever (38.5°C) over 1 day and had vomited once. His headache had intensified over the previous 2 days and was associated with photophobia. On the day of admission, he noted the sudden appearance of bilateral tinnitus and hearing loss. On examination, the patient was afebrile and had no signs of meningeal irritation or neurological deficits other than severe bilateral sensorineural hearing loss (SNHL).
The results of complete physical, neurological and ophthalmological examination were otherwise normal. The ECG, chest radiograph and laboratory studies were notable only for a serum C-reactive protein level of 0.36 (normally < 0.08) g/L, serum fibrinogen 4.85 (normally < 4.00) g/L and mild leukopenia (leukocytes 4.1 [normally 5.0–10.0] х 109/L), which later became normal. The initial investigation was directed mainly at varied infectious causes, hematological malignancies and autoimmune diseases. Serological tests for herpesviruses, hepatitis viruses, HIV and influenza viruses, as well as for syphilis, Lyme disease, mycoplasma, chlamydia and rickettsiae, were negative on admission and during convalescence. No autoantibodies were found.
Pure tone audiometry showed an average speech reception threshold (the mean of the thresholds at the frequencies of 0.5, 1 and 2 kHz) of 60 dB in the right ear and 65 dB in the left ear, with a 76% discrimination score, which measures ability to discriminate speech on speech audiometry. All measured frequencies, from 250 to 8000 Hz, were affected (Fig. 1). Auditory brain stem responses showed normal peak and interpeak latencies on both sides.
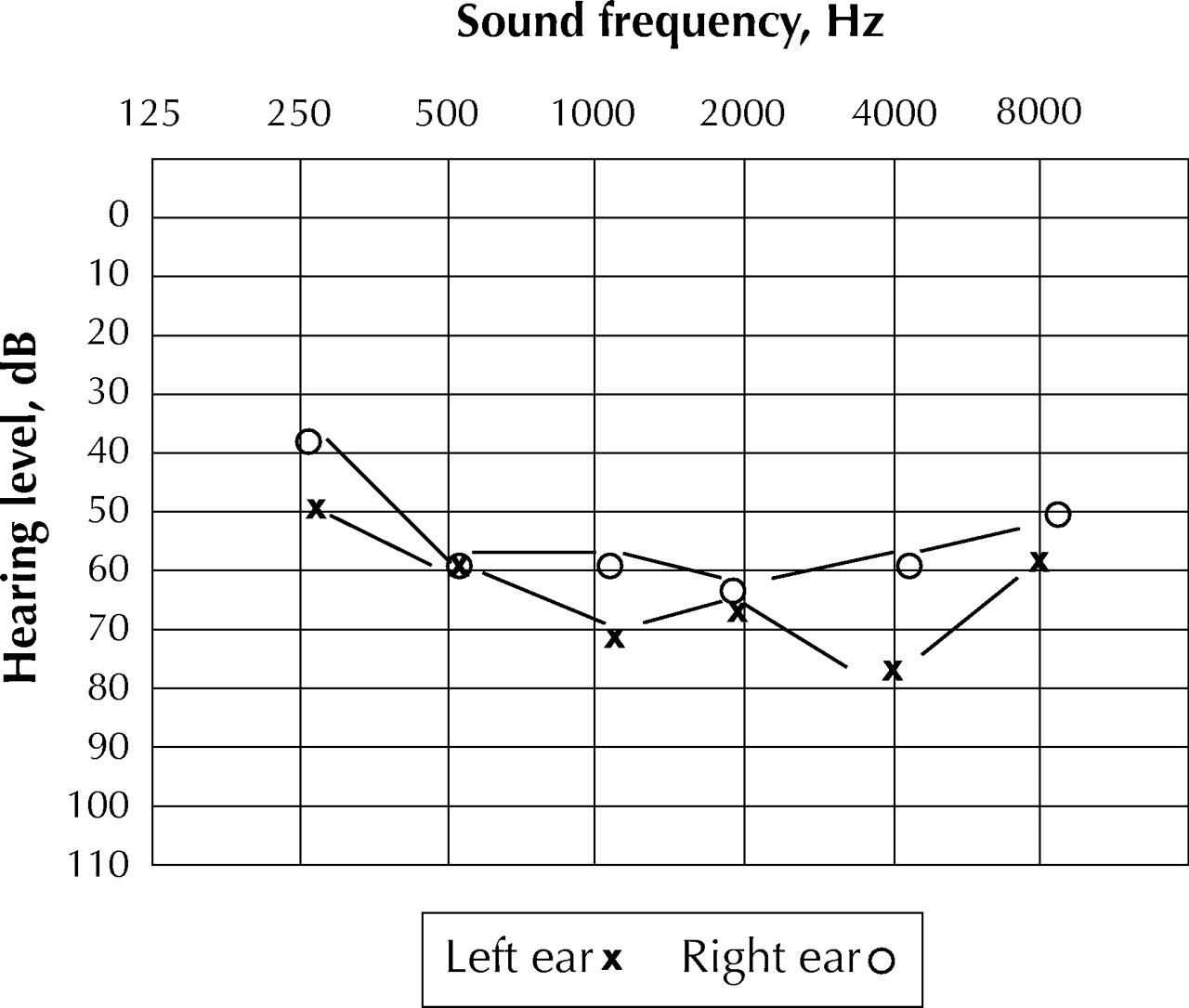
Fig. 1: Results of pure tone audiometry carried out on the patient's presentation.
The results of brain imaging (CT with contrast and MRI with gadolinium) were normal.1 A lumbar puncture was performed to look for “aseptic” meningitis and study cerebrospinal fluid (CSF) cell cytology and oligoclonal IgG.2 It revealed CSF under normal pressure, with normal protein and glucose levels and 0.11 х 109/L leukocytes (97% mononuclear cells) of normal morphology on cytological examination. The findings of microbiological stains and cultures were negative.
The patient was treated with methylprednisolone pulse therapy (1 g/d intravenously, over 3 days) followed by prednisone, 60 mg/d, which was gradually tapered off. He continued to complain of persistent tinnitus and hearing loss. On the fifth day in hospital, an objective improvement in hearing was first demonstrated, and at 10 days a dramatic improvement was found, with speech reception thresholds of 15 dB (right ear) and 25 dB (left ear) at all measured frequencies and 100% discrimination.
The patient then recalled that his wife and baby daughter had had a short self-limited illness about 10 days before his admission: both had fever, vomiting and diarrhea, which resolved spontaneously within 2–3 days. In addition, epidemiological data indicated that over the 8–10 weeks preceding admission an outbreak of enterovirus infections was documented in Israel. The patients, mostly children and young adults, were admitted to hospital with aseptic meningitis. The virus in this outbreak had been cultured and identified as an echovirus of the same serotype (echovirus type 4). On several occasions familial clustering was observed, explained by the known spread of enterovirus from person to person via the fecal–oral route.3
The patient's CSF, which had been kept frozen, was therefore re-examined: following extraction, the RNA was subjected to reverse transcription polymerase chain reaction (PCR) using enterovirus universal primers in one reaction tube, as described elsewhere.4 The sample was tested along with positive and negative buffer and CSF controls, taking special precautions to avoid contamination. The amplification product was detected on microwell plates containing an immobilized oligonucleotide probe specific for enteroviruses (Chemicon International Inc., Temecula, Calif.), using enzyme immunoassay. PCR revealed clear evidence of enterovirus infection. The virus was later cultured from the patient's stool.
Comments
We report the case of a young man who presented in the fall with self-limited aseptic meningitis and sudden severe bilateral SNHL caused by enterovirus infection. The diagnosis was established by PCR and supported by epidemiological and microbiological data.
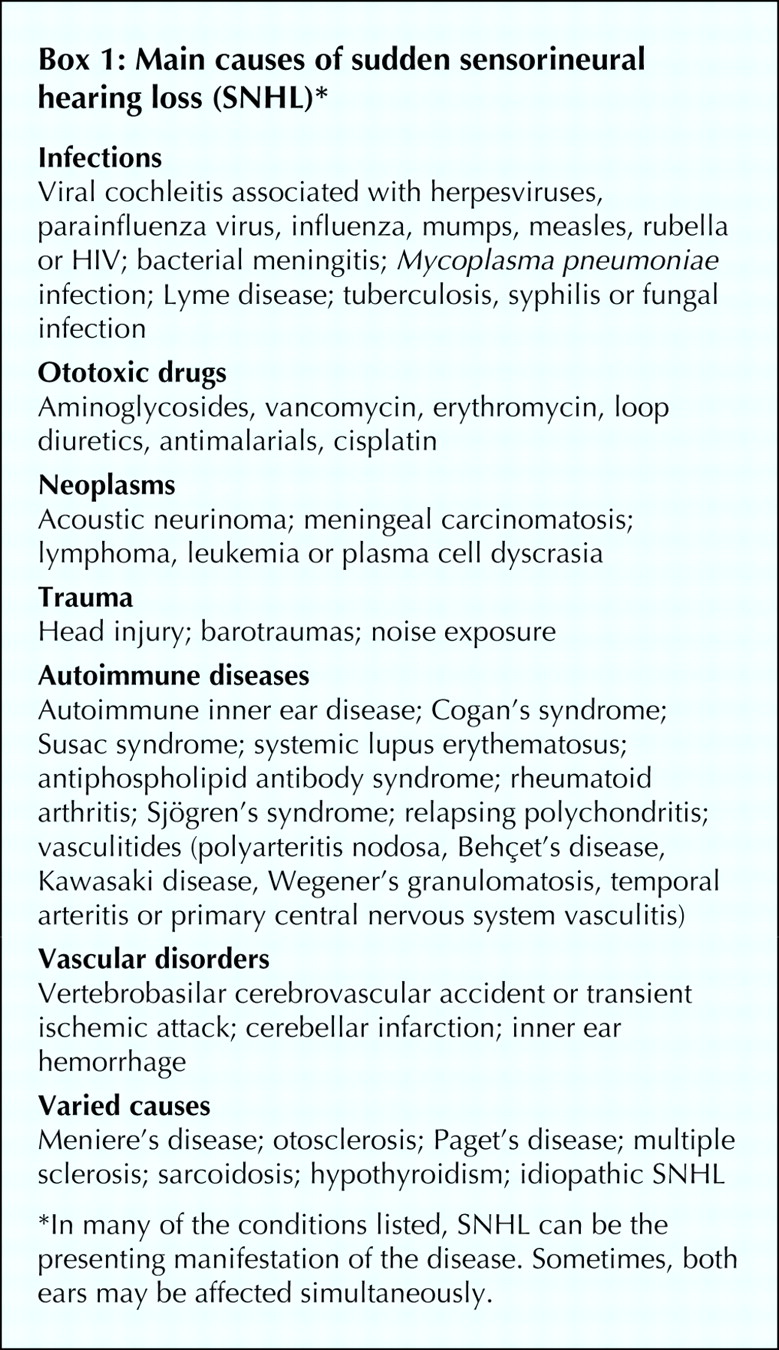
Sudden SNHL is defined as hearing loss of 30 dB or more over at least 3 contiguous audiometric frequencies occurring within hours to less than 3 days.5,6 This is often an alarming experience for the patient, particularly when both ears are affected simultaneously, which is an uncommon occurrence. For the clinician, it constitutes a considerable diagnostic challenge, because it may be caused by many diverse conditions, which may be difficult to recognize, especially when sudden SNHL is the presenting manifestation (Box 1).5,6,7,8,9,10,11,12 Enteroviruses have not been previously associated with SNHL.
{kind=link}
{kind=link}
Many cases of SNHL elude definitive diagnosis.13 Nevertheless, patients can often be offered specific therapy, provided a timely diagnosis can be made.5,14 Enterovirus infections are quite common, especially in the summer and fall, but often remain undetected.3 Our findings suggest that the availability of the highly sensitive PCR test for enterovirus allows better understanding of the full scope of enterovirus-associated neurological manifestations. The possibility that enterovirus infections may be associated not only with aseptic meningitis but also with viral cochleitis and sudden SNHL should be recognized. It may even account for some hitherto “idiopathic” cases of SNHL. The recent development of pleconaril, which may be used as specific therapy for enterovirus infections,14,15 highlights the importance of early diagnosis of enteroviruses as the cause of otherwise idiopathic sudden hearing loss.
Footnotes
-
This article has been peer reviewed.
Contributors: Drs. Schattner, Halperin and Zimhony diagnosed the case and treated the patient. Dr. Wolf performed the PCR testing and monitored the enterovirus outbreak. Dr. Schattner drafted the article, and all authors participated in its preparation and revision.
Competing interests: None declared.
References
In this issue
Article tools






Related Articles
Cited By...
More in this TOC Section
Research
Similar Articles
Collections

