


Abstract
Background: Congestive heart failure (CHF) is a common disease requiring admission to hospital among elderly people and is associated with a high mortality rate. The objective of this study was to examine trends in CHF mortality and admissions to hospital in Montreal between 1990 and 1997 for individuals aged 65 years or more.
Methods: We obtained information about deaths from the Quebec Death Certificate Registry database and information about admissions to hospital from the Québec Med-Écho database. Patients with a primary diagnosis that was classified as ICD-9 code 428 were considered cases of CHF.
Results: Although age-adjusted rates of mortality from CHF did not change significantly between 1990 and 1997, the annual rate of admission to hospital for CHF increased from 92 per 10 000 population in 1990/91 to 124 per 10 000 population in 1997/98 (p < 0.01). Deaths due to CHF, expressed as a proportion of all cardiovascular deaths, increased among women from 5.6% in 1990 to 6.2% in 1997 (p = 0.01). The rate of readmission for all causes following a first admission for CHF during that year rose over the study period from 16.6% to 22.0% within one month (p < 0.001) and from 46.7% to 49.4% within 6 months (p = 0.03). Conversely, mean annual length of stay per admission decreased from 16.4 days in 1990/91 to 12.2 days in 1997/98.
Interpretation: The increase in rates of admission to hospital for CHF and the stable rates of CHF mortality suggest that the management of CHF and its antecedents has improved in recent years.
The mortality rate for individuals with congestive heart failure (CHF) remains high,1,2,3,4,5 however, rates of survival are improving in some countries.2,6 The increasing use of effective treatments to reduce death and complications due to ischemic heart disease, which is a major cause of CHF, may have resulted in an increasing number of people alive with CHF.7,8 These treatments include phramacological therapy, such as ASA and β-blockers, thrombolytic therapy, angioplasty and coronary artery bypass surgery. The aging of the population and its effects on the incidence and prevalence of heart failure suggest that this problem will become more pronounced in the future. Advances in heart failure management may reduce morbidity and improve survival,9 however, CHF remains a frequent cause for admission to hospital among elderly people.10,11,12 The objective of this study was to describe trends in the mortality rate and in admissions to hospital for individuals aged 65 years or more with CHF, living in Montreal.
Methods
This investigation was limited to residents of Montreal between 1990 and 1997 who were aged 65 years or more. Mortality data were obtained from the Quebec Death Certificate Registry database, whereas information about admissions to hospital was obtained from the Québec Med-Écho database. The former reports deaths per calendar year (January 1 to December 31), and the latter provides information about hospital discharges per hospital financial year (April 1 to March 31). All individuals with a primary diagnosis classified as ICD-9 code 428 were included as cases of CHF.13
CHF mortality rates, by sex and age group (65–74, 75–84, ≥ 85 years), were calculated by dividing the number of patients who died from CHF by the population alive during that year. Furthermore, age-standardized mortality rates were calculated for all those aged 65 years and more. The standard population used for the age standardization was the population of Montreal in 1996. The observed annual rates of CHF for the groups aged 65–74 years, 75–84 years, and 85 years and more were applied to this standard population in order to calculate the yearly age-standardized rates. The proportion of CHF deaths among total cardiovascular disease (CVD) deaths was calculated. The CVD category comprised ICD-9 codes 390–459. The mean annual number of CHF admissions per patient was calculated as the number of CHF admissions divided by the number of individuals admitted for CHF in that year. Annual rates of admission to hospital were calculated by dividing the number of admissions to hospital by the annual population aged 65 years and over. Rates of admission to hospital were also age-standardized. Readmission rates were calculated as the number of patients admitted within one or 6 months after the date of discharge following their first admission for CHF during that year. The Montreal population for each year of the study period was obtained from the Quebec Ministry of Health and Social Services.14 The 𝛘2 test for linear trend in proportions was used to evaluate the statistical significance of trends observed through time.
Results
Mortality
The number of people aged 65 years and more living in Montreal during the study period ranged between 249 899 and 269 354, whereas the number of deaths from CHF ranged between 239 and 300 per year. Men had higher mortality rates than women for all years except 1993 and 1996. The crude rate of death from CHF for women increased from 9.9 per 10 000 population in 1990 to 10.3 per 10 000 population in 1997 (p = 0.02). When standardized for age, the observed increase in mortality among women no longer reached statistical significance (Fig. 1).
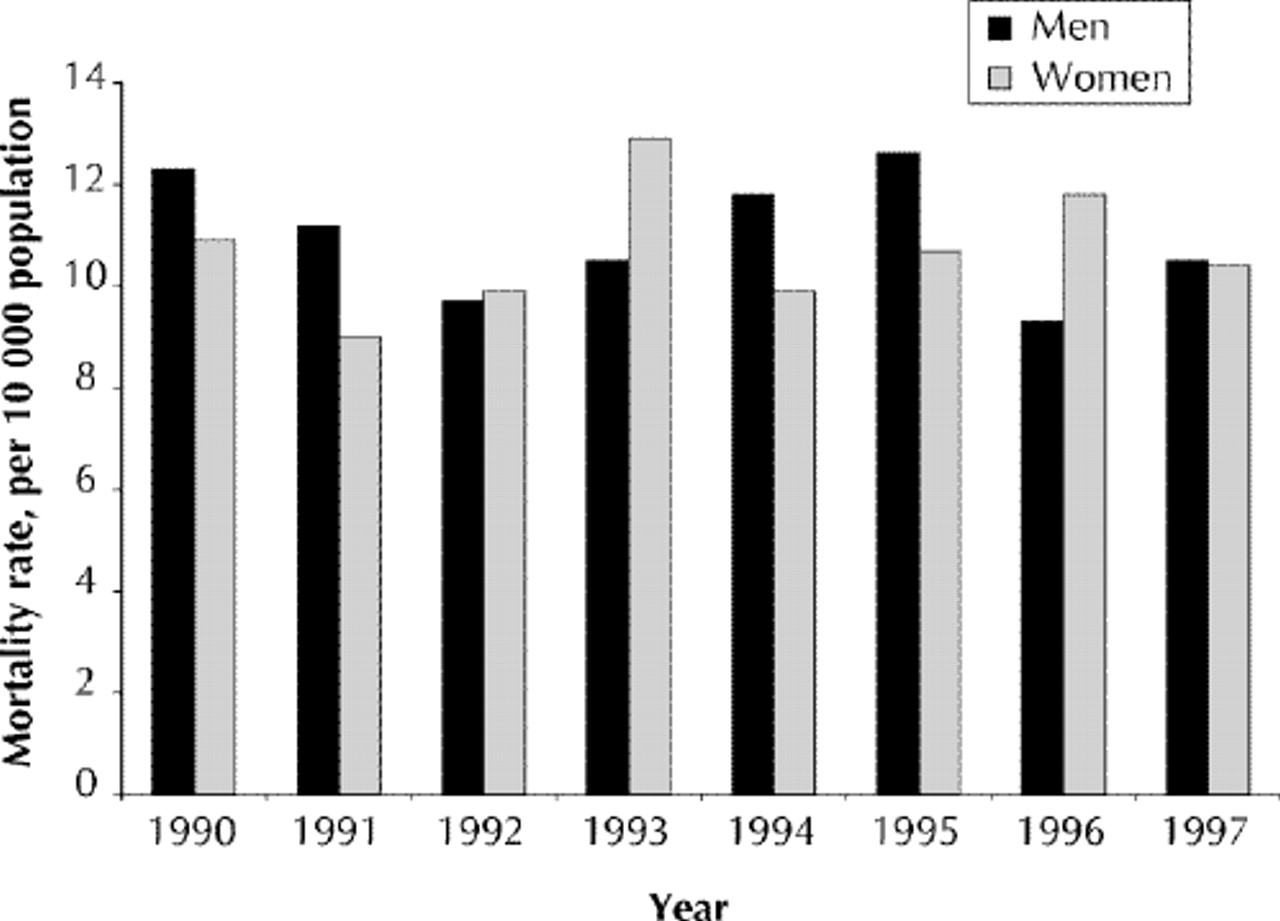
Fig. 1: Age-adjusted rates of mortality from congestive heart failure for individuals aged 65 years or more in Montreal from 1990 to 1997.
Between 1990 and 1997, all CVD deaths increased by 1.7% in men and by 3.6% in women. The proportions of CHF deaths among all CVD deaths in women were higher compared with those in men, and increased in women from 5.6% in 1990 to 6.2% in 1997 (p = 0.01, Table 1).
Table 1.
Death rates from CHF ranged between 2.0 per 10 000 population in 1990 and 3.1 per 10 000 population in 1997 among the 65–74-year age group, between 10.0 per 10 000 population in 1990 and 13.1 per 10 000 population in 1997 in the 75–84-year age group, and between 41.2 per 10 000 population in 1990 and 62.4 per 10 000 population in 1997 for those aged 85 years and more. Men consistently had higher mortality rates than women among individuals aged less than 85 years, however women aged 85 years and more had higher rates in 1991 and 1996.
Admissions to hospital
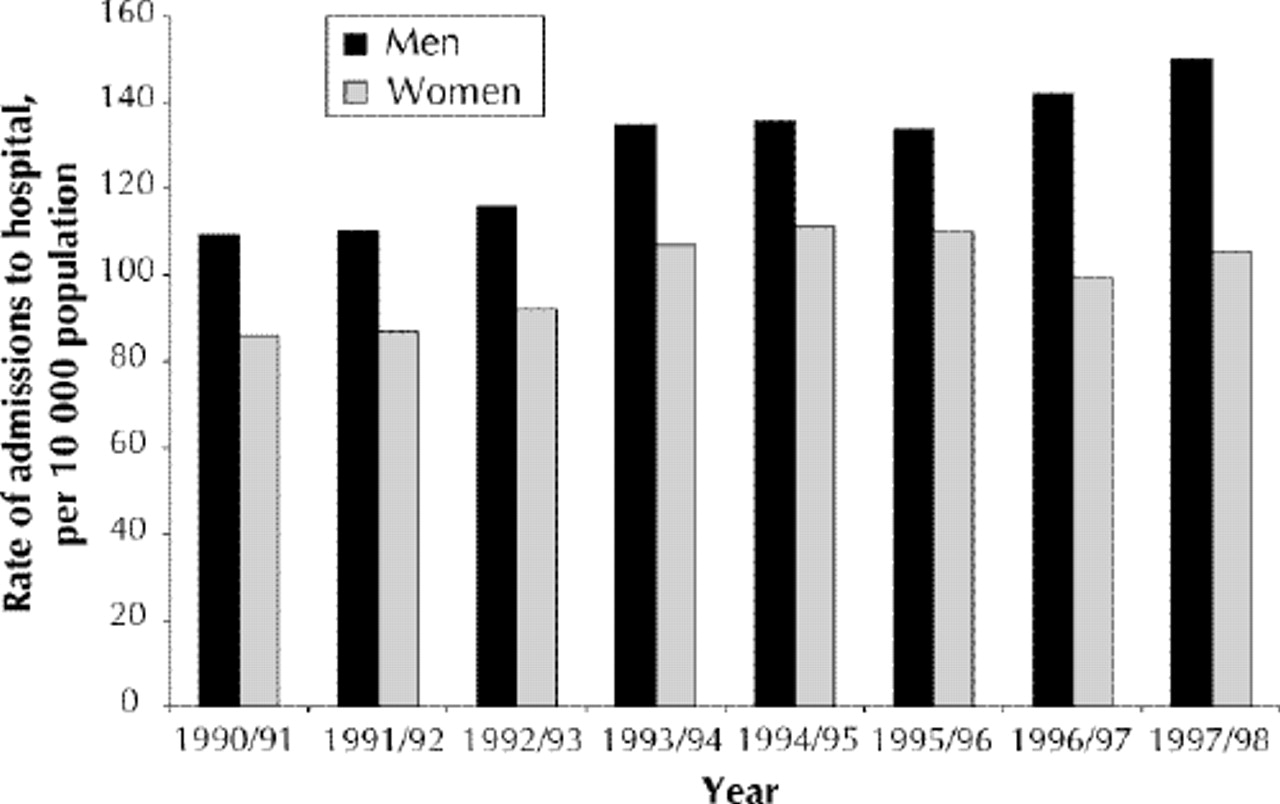
Annual crude and age-adjusted rates of admission to hospital increased significantly (p < 0.001) for both men and women. Rates for men remained higher than those for women (Fig. 2). Rates of admission to hospital increased in all age groups, but most rapidly in those aged 85 years or more. There was an increase in both the number of admissions and patients admitted (Table 2). During the study period, mean length of stay decreased from 16.4 days in 1990/91 to 12.2 days in 1997/98, and length of stay was consistently higher in women than in men.
Table 2.
{kind=link}
{kind=link}
Fig. 2: Age-adjusted rates of admission to hospital for congestive heart failure for individuals aged 65 years or more in Montreal from 1990/91 to 1997/98.
The rate of readmission for all causes following a first admission for CHF during that year increased significantly from 16.6% to 22.0% within one month of discharge (p < 0.001) and from 46.7% to 49.4% (p = 0.03) within 6 months. Readmissions within one month due to cardiovascular problems rose from 10.3% to 13.5% (p < 0.001) and from 29.9% to 32.9% (p = 0.003) within 6 months.
Interpretation
Although mortality rates did not change significantly, an increase was observed in the number of women dying from CHF as opposed to other CVD-related mortality. Rates of admission to hospital increased significantly for both men and women, whereas respective inpatient days per episode decreased for both sexes. Concurrently, readmission rates increased among both men and women.
The information obtained from these administrative databases has its limitations. First, these databases do not store information on clinical severity. Second, diagnostic coding may be problematic; because only primary diagnoses of CHF were considered for this study, we may well have underestimated the number of people with CHF.15 Although these factors may affect the absolute number of admissions to hospital and deaths, this probably does not affect the overall conclusions regarding the trends observed through time.
Declining length of stay may be due to improvements in the management of CHF or increased pressure on beds because of an increasing number of patients. During the study period, the number of hospital beds available in Montreal decreased as part of the health care reforms that were introduced in Quebec, which involved a shift toward more ambulatory care and the closure of several hospitals.16
Differences between women and men in admissions and mortality may reflect differing clinical profiles associated with different mortality risks for men and women. In men, coronary artery disease is the more frequent underlying cause of CHF, whereas in women it is associated with diabetes, hypertension or atrial fibrillation, and left ventricular systolic function is often preserved.17 Gender differences in the use of services may reflect different requirements, demographic differences or differences in access to services by men and women, as has been observed for coronary heart disease.18,19
Specific CHF programs and specialized clinics are being introduced in Montreal, subsequent to our study. Some studies suggest that these measures reduce hospital admissions and improve quality of life.20 In order to evaluate continuously the use, cost and outcome of CHF service provision in Montreal, a multicentre prospective monitoring system is currently being established.21
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
References
In this issue
Article tools






Jump to section
Related Articles
Cited By...
- Multidisciplinary heart failure clinics: Are they effective in Canada?
- Beta-blockers and angiotensin-converting enzyme inhibitors/receptor blockers prescriptions after hospital discharge for heart failure are associated with decreased mortality in Alberta, Canada
- Trends and ethnic differences in hospital admissions and mortality for congestive heart failure in the elderly in Singapore, 1991 to 1998
- Congestive heart failure: What can we offer our patients?
More in this TOC Section
Similar Articles

