


Abstract
Background: Hypernatremic dehydration in neonates is a potentially devastating condition. Recent reports have identified breast-feeding malnutrition as a key factor in its pathophysiology.
Methods: Using a theoretical framework for breast-feeding kinetics, a retrospective chart review of all neonates less than 28 days of age who were seen at either British Columbia's Children's Hospital or the Vancouver Breastfeeding Centre between 1991-1994 was conducted to identify and classify possible causes of breast-feeding malnutrition among neonates who developed hypernatremic dehydration.
Results: Twenty-one cases hypernatremic dehydration were identified. Infant weight loss ranged from 8% to 30% of birth weight, and serum sodium levels ranged from 146 mmol/L to 207 mmol/L. In each case, maternal or infant factors (e.g., poor breast-feeding technique, lactation failure following postpartum hemorrhage and infant suckling disorders associated with cleft palate or ankyloglossia) that could interfere with either lactation or breast-feeding dynamics and account for insufficient breast milk intake were identified.
Interpretation: Prenatal and in-hospital screening for maternal and infant risk factors for breast-feeding malnutrition combined with early postpartum follow-up to detect excessive infant weight loss are important for the prevention of neonatal hypernatremic dehydration.
Hypernatremic dehydration is a potentially devastating condition. The number of anecdotal case reports of hypernatremic dehydration in neonates in the last few years has increased.[1–3] Recent studies have identified breast-feeding malnutrition as a key factor in its pathophysiology but have failed to classify the causes of insufficient milk intake.[4–6]
Early postpartum hospital discharge may leave mothers poorly prepared for breast-feeding and may contribute to increased neonatal morbidity.7 Some breast-feeding mothers perceive their milk supply is inadequate or recognize their baby is failing to thrive and rapidly resort to bottle feeding.8 In contrast, other mothers are aware of the unique characteristics of breast milk and persist with exclusive breast-feeding, reluctant to give additional formula despite excessive neonatal weight loss. These babies are at risk of developing malnutrition and hypernatremic dehydration, with the potential for seizures and permanent neurological and vascular damage if their condition is not recognized and treated early.9
Normal neonatal feeding is usually on demand every 2-4 hours, with a minimum intake of 30 mL/feed. Adequate breast milk intake depends on several interrelated stages: normal mammary development (mammogenesis), unimpeded initiation of lactation (lactogenesis), sustained ongoing milk synthesis (galactopoiesis) and effective milk removal. Milk removal depends on effective maternal and infant breast-feeding techniques, combined with an intact milk-ejection reflex, and total daily milk intake depends on the frequency and duration of feeds and the pattern of breast use.10 It is normal over the first week of life for the neonate to lose as much as 7% of its birth weight through normal diuresis. Neonates should start to gain weight within a few days and regain their birth weight by the tenth day of life. Either rapid weight loss or loss greater than 7% of birth weight is a cause for concern. The first signs of neonatal dehydration include the failure to have bowel movements or the presence of urate crystals, combined with weight loss.
Breast-feeding malnutrition in an exclusively breast-fed neonate can be defined as "failure to thrive because of inadequate daily breast milk intake." Many underlying factors can interfere with lactation and breast-feeding and contribute to the final common pathway leading to breast-feeding malnutrition[10, 11] (Fig. 1). Some authors, in noting a relationship between neonatal hypernatremic dehydration and elevated maternal breast milk sodium, have suggested a direct causal relationship.[12, 13] Yet, there has been little emphasis placed on evaluating the volume of breast milk intake or on the value of a clinical lactation and breast-feeding assessment to identify the causes of insufficient breast milk intake.

Fig. 1: Factors contributing to neonatal insufficient breast milk syndrome. Reprinted from Livingstone,10 with permission.
The purpose of this study was to identify and classify possible underlying causes of breast-feeding malnutrition that resulted in neonatal hypernatremic dehydration and to encourage physicians to perform careful breast-feeding assessments so that breast-fed neonates at risk for dehydration can be identified.
Methods
The British Columbia's Children's Hospital is a tertiary care referral centre in which approximately 30 000 patients are seen in the emergency department each year. The Vancouver Breastfeeding Centre is a community clinic for lactation and breast-feeding-related problems; it counsels approximately 800 new patients each year. All neonates seen at these 2 centres from 1991 to 1994 who were less than 28 days of age and with serum sodium concentrations exceeding 145 mmol/L were identified through a computer search. Additional selection criteria for our study included that the neonates were predominantly breast-fed with little or no formula supplementation and weight loss was more than 7% of birth weight.
Maternal and infant hospital charts were reviewed, and mothers were interviewed by telephone. Data were also obtained from the standard clinical breast-feeding assessment, routinely performed on patients referred to the Vancouver Breastfeeding Centre. This assessment included a detailed maternal and infant history and examination, an observation of breast-feeding, a standard test feed (i.e., measurement of infant's weight before and after a feed) and the volume of residual pumped breast milk. On the basis of breast-feeding kinetics,14 the data were classified for possible causes of insufficient breast milk intake (Table 1).
Table 1: Factors associated with insufficient milk intake
Results
Twenty-one cases of hypernatremic dehydration in breast-fed neonates were identified (Table 2); 8 neonates presented to the Vancouver Breastfeeding Centre and under went a detailed clinical breast-feeding assessment; 13 cases were referred directly to the hospital by a family physician or pediatrician and did not have a detailed breast-feeding assessment. Infant age at presentation ranged from 3 days to 14 days (mean 8 days). Presenting complaints included weight loss, failure to gain weight, lethargy, poor feeding and infrequent or absent bowel movements. Three of the neonates had passed 1 or no stools in the preceding 7 days, and 2 had passed none in the preceding 2 days. Two had documented seizures. Nineteen of the neonates were exclusively breast-fed and 2 had been supplemented with approximately 30 mL of expressed milk every 2-4 hours for the 48 hours prior to admission.
Table 2: Characteristics of 21 cases of hypernatremic dehydration in breast-fed neonates
Infant birth weight ranged from 2950 g to 4695 g, and weight loss ranged from 8% to 30% (mean 19.3%) of birth weight. On initial examination signs of dehydration (i.e., dry mucous membranes, sunken fontanelle, poor skin turgor) were noted in only 11 cases and mild jaundice, in 8 cases; 2 babies had ankyloglossia (tongue-tie), 1 had significant retrognathia and 1, a cleft lip and palate. No other underlying pathological conditions were detected. Infant serum sodium on initial testing ranged from 146 mmol/L to 207 mmol/L (mean 161 mmol/L). In each case the clinical diagnosis was failure to thrive, malnutrition and hypernatremic dehydration because of insufficient breast milk intake. Of the 21 neonates, 17 were admitted to hospital and 4 were treated as outpatients.
Seventeen mothers were primigravid and 16 had spontaneous vaginal deliveries; 10 mothers experienced excessive postpartum hemorrhages with anemia.
On the basis of the chart review, possible underlying causes of low breast milk intake were classified according to inadequate maternal milk synthesis, inefficient milk removal or inadequate daily infant milk intake. Inadequate maternal milk synthesis was further subdivided into failure of mammogenesis, lactogenesis, or galactopoiesis. The results are as follows.
Clinical symptoms and signs of successful mammogenesis include prenatal breast tenderness and growth. One mother had failure of mammogenesis; she had small hypoplastic breasts, which had not enlarged prenatally. Her 2 other breast-fed children had required supplementary feeding because of a lack of milk production. This case was confounded by inadequate breast stimulation, a result of infrequent feeds; the first breast-feed took place immediately post partum, but because of neonatal sleepiness feeds were on demand only every 7-9 hours. On day 3 the mother felt her milk was in, but only expressed 15 mL on pumping; no supplements were given. By day 7 the neonate had lost 18% of his birth weight. On examination the neonate had retrognathia and the tongue was positioned at the roof of his mouth during the feed, thereby interfering with milk removal. The test feed was 0 g.
Clinical symptoms and signs of successful lactogenesis include a sensation of "milk coming in," postpartum breast enlargement or engorgement and the production of colostrum. Five mothers experienced prenatal breast tenderness and enlargement, suggesting normal mammogenesis, but experienced no postpartum breast changes. They breast-fed on demand every 2-4 hours. The infant test feeds combined with the residual volume of maternal breast milk expressed were less than 30 mL, indicating inadequate milk synthesis (normal range, 60-80 mL). Four mothers had documented postpartum hemorrhages and 1 experienced "moderate" blood loss. All had a significant fall in hemoglobin (mean 29 g/L), and none received a blood transfusion. Each mother had a tentative diagnosis of pituitary disruption secondary to postpartum hemorrhage causing failure of lactogenesis.15 Breast milk sodium was measured in 4 mothers and found to be elevated.[16, 17]
Clinical symptoms and signs of successful galactopoiesis include copious milk production, combined with prefeed breast fullness, followed by postfeed softening. Of the 7 mothers who experienced failure of galactopoiesis 6 experienced definite breast growth during pregnancy and some degree of breast engorgement post partum, suggesting normal mammogenesis and lactogenesis, but they had little ongoing milk production. Failure of galactopoiesis was due to inadequate ongoing breast stimulation and drainage, which led to rapid involution and drying of the milk supply. The only multiparous mother in this group had successfully lactated previously.
Factors contributing to inadequate breast stimulation and drainage included difficulty latching onto the breast (6 neonates), inverted nipples (1 mother) and ankyloglossia contributing to a suckling disorder (1 neonate). Three babies were described as very sleepy in nature and feeding, attempted every 2-4 hours, lasted up to 90 minutes. In 2 other cases the infants were feeding sufficiently often but were unsettled after feeds. Two infants received supplements for 36 hours before presentation; both had test feeds of 0 g. The breast milk sodium concentration was elevated in 3 of 4 cases measured.
Efficient milk removal depends on correct maternal positioning and latching and normal infant suckling dynamics; 9 of the 21 infants demonstrated poor breast-feeding techniques, which resulted in ineffective milk removal. They breast-fed on demand every 2-4 hours for 20-90 minutes. The mothers experienced definite prenatal and postpartum breast enlargement, indicating normal mammogenesis and lactogenesis. Two mothers had postpartum hemorrhages with a significant drop in hemoglobin, but ongoing galactopoiesis seemed adequate, as indicated by the high volume of residual milk expressed at the time of presentation. Both multiparous mothers had previously breast-fed successfully. Factors contributing to inefficient mild removal included a minor cleft lip and palate (1 neonate), ankyloglossia (1 neonate), sleepiness during feeding (1 neonate) and inverted nipples (1 mother). All of these mothers had difficulty getting their babies to latch and breast-feed properly, and this resulted in insufficient milk removal by the neonate. Breast milk sodium was high in 1 of 5 cases measured.
Management
Therapy for hypernatremia involved ensuring adequate calorie intake and correcting the electrolyte imbalance through careful oral rehydration. If a standardized test feed showed insufficient breast milk intake complementary feeds were given with expressed breast milk or formula using a bottle with a wide-based nipple. If the neonate's serum sodium was significantly elevated admission to hospital was required for controlled oral or intravenous rehydration.18
The management for the mothers focused on increasing milk yield through regular, effective breast-feeding using both breasts for each feed. Mothers were taught correct position and latch techniques to ensure optimal milk removal and instructed to pump each breast after feeds to enhance stimulation and drainage. Domperidone, a dopamine antagonist that blocks prolactin inhibition and can increase maternal milk synthesis, was prescribed in 7 cases.
Interpretation
In each of our cases there was a correlation between breast-feeding malnutrition and neonatal hypernatremic dehydration. Maternal or infant factors that preexisted could have affected different phases of lactation or breast-feeding and resulted in breast-feeding malnutrition; prenatal or early postpartum screening could have identified all of these factors.19 One mother had a lack of mammogenesis, which resulted in primary failure of lactation, the etiology of which was unclear.20 Five mothers were identified as having a failure of lactogenesis. A common factor in these cases was a history of postpartum hemorrhage, defined as loss of more than 500 mL of blood during the first 12 hours after delivery. All of these mothers had significant postpartum hemorrhages, compared with only 4 of the 15 who had evidence of successful lactogenesis. Postpartum hemorrhage may cause temporary pituitary ischemia or disruption and result in hypolactation. None of the mothers in this study were diagnosed with Sheehan's syndrome. It should be noted that measured blood loss is usually twice the estimated amount,21 and the literature suggests there is no relation between the amount of blood loss within the definition of postpartum hemorrhage and the subsequent development of anterior pituitary deficiency.[22, 23]
Infrequent breast stimulation and drainage associated with a nondemanding, sleepy infant can lead to galactopoiesis failure. This is related to inadequate prolactin surges and a build up of local inhibitory factors in the milk.24 Ineffective milk removal was primarily associated with poor breast-feeding techniques (i.e., incorrect position and latch). In several cases there were also compounding factors, including maternal and infant anatomical abnormalities that interfered with suckling dynamics. There is debate in the literature regarding the significance of ankyloglossia in relation to breast-feeding. It is generally accepted that there are cases where it impedes suckling, and frenotomy can resolve the sucking disorder.25 However, one survey found ankyloglossia in 3.7% of breast-fed infants.26
Breast milk sodium, measured in 13 cases, was elevated in 8. The clinical significance of high breast milk sodium levels is unclear. It may reflect a delay in maturation of colostrum into mature milk, or it may result from milk stasis and premature weaning and the subsequent reabsorption of fluid. It was probably not the direct cause of neonatal hypernatremia.27
Seventeen of the mothers were primiparous, and this may represent a compounding factor because the mothers lacked experience and failed to recognize the severity of their infant's illness. Despite severe malnourishment, 8 neonates did not exhibit characteristic signs of dehydration, such as sunken fontanelles and lack of skin turgor. This may mislead clinicians to underestimate the degree of dehydration. Lack of bowel movements and the presence of urate crystals are both sensitive markers for dehydration.
The prevention of breast-feeding malnutrition and hypernatremia in breast-fed neonates begins with prenatal and early postpartum screening to identify possible maternal and infant factors that could interfere with successful lactation and breast-feeding, as well as with anticipatory guidance regarding basic breast-feeding techniques.[28–32]
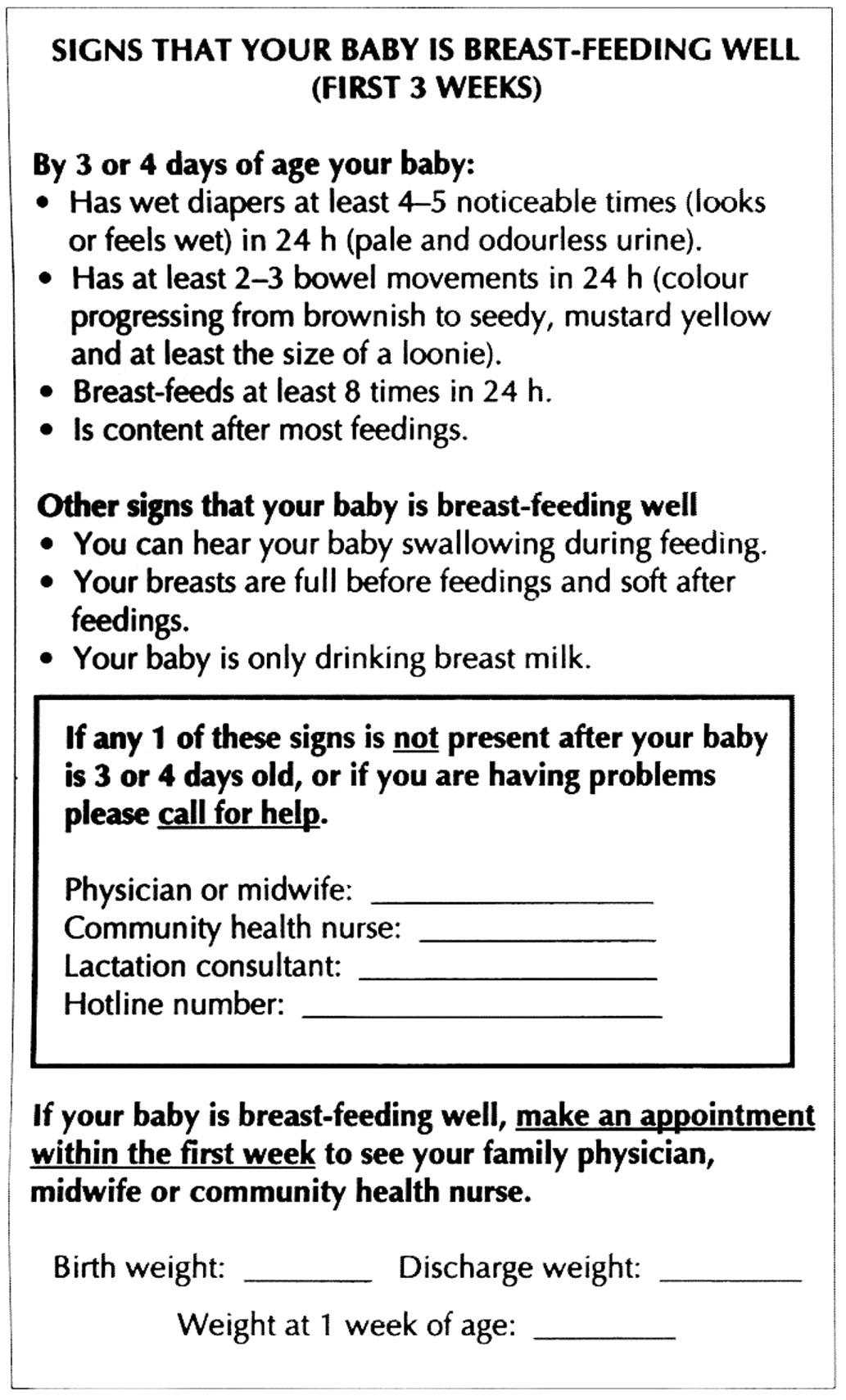
On the basis of these findings, an interdisciplinary committee comprising representatives from the hospital and community recommended that all mothers should be taught the signs of successful breast-feeding and the warning signs of dehydration (Fig. 2). The Baby Friendly Hospital Initiative encourages health professionals to teach all mothers the skills of breast-feeding and stresses the importance of early routine postpartum follow-up, which should include frequent monitoring of infant growth.[33, 34] If a neonate loses more than 7% of its birth weight, if weight continues to fall after the first week, or if the birth weight has not been regained within 10 days, a clinical lactation and breast-feeding assessment is warranted. This will aid in the early detection of insufficient breast milk intake and failure to thrive and in the prevention of hypernatremic dehydration.

{kind=link}
{kind=link}
Fig. 2: Brochure given to new mothers at the time of hospital discharge explaining the signs that indicate breast-feeding is going well.
As with all retrospective studies, bias may have been introduced because some of the records we reviewed were incomplete. A prospective study of the incidence of hypernatemic dehydration in exclusively breast-fed infants would further define the scope of the problem.
Financial assistance for this project was provided by the Optimist Club of downtown Vancouver.
Competing interests: None declared.
Acknowledgments
CMAJ will award prizes for the best essays on any health-related subject submitted during calendar year 2000. A $2000 prize will be awarded for the best entry submitted by a medical student or resident. There is also a $2000 prize for the best entry submitted by any author. These new contests replace the Logie Medical Ethics Essay Contest for medical students.
We are looking for reflective essays of up to 1500 words. Manuscripts must be original and must be submitted only to CMAJ. Winners will be selected by a committee appointed from the CMAJ Editorial Board. Winning entries will be selected based upon originality, quality of writing and relevance to health or health care. To win, a manuscript must be suitable for publication. If suitable entries are not received, prizes will not be awarded. All papers submitted will be considered for publication in CMAJ.
Authors should submit their papers with a covering letter stating that they wish the manuscript to be considered for the essay prize, and should indicate their status regarding training. Send entries and queries to: Dr. John Hoey, 1867 Alta Vista Dr., Ottawa ON K1G 3Y6; hoeyj{at}cma.ca
Footnotes
-
This article has been peer reviewed.
Reprint requests to: Dr. Verity Livingstone, Department of Family Practice, 690 W 11th Ave., Vancouver BC V5Z 1M1; fax 604 875-5017; [email protected]
References
In this issue
Article tools






Jump to section
Related Articles
Cited By...
- Providing breastfeeding support during the COVID-19 pandemic: Concerns of mothers who contacted the Australian Breastfeeding Association
- Tongue Tie and Frenotomy in the Breastfeeding Newborn
- Reference chart for relative weight change to detect hypernatraemic dehydration
- Index of Suspicion in the Nursery *
- Hypernatraemia in the first few days: is the incidence rising?
- Hypernatraemic dehydration and breast feeding: a population study
More in this TOC Section
Similar Articles
Collections

