


- © 2008 Canadian Medical Association
More than 40 million patients receive anesthesia each year in North America. The risks associated with anesthesia have progressively decreased, but the mechanisms of action of anesthetic drugs remain poorly understood. This lack of knowledge has limited the optimum use of drugs that are currently available and has slowed efforts to develop even safer anesthetics. Many complex and lengthy surgical procedures, often performed on medically compromised patients, have been made possible by modern anesthetic techniques. However, anesthetic drugs, like other medications, have limitations, contraindications and adverse effects.
One of the more common concerns expressed by patients who are about to undergo anesthesia is that they will remember intraoperative events.1 For some, this concern will likely be heightened with the Nov. 30, 2007, release of the movie Awake, about a young patient who experiences intraoperative awareness during cardiac surgery (www.awakethemovie.com). Many anesthesiologists are already reporting an increase in the number of patients raising questions about intraoperative awareness, and surgeons and primary care physicians may also soon be faced with such enquiries. In this commentary, we define the nature of the problem of awareness, identify the risk factors, describe strategies to reduce the incidence of intraoperative awareness and point to resources for further information.
Intraoperative awareness is the unexpected and explicit recall by patients of events that occurred during anesthesia. As many as 1 or 2 in every 1000 patients who receive general anesthesia experience this outcome, and the incidence may be even higher among children.2–4 Most patients who remember intraoperative events do not experience pain; rather, they have vague auditory recall or a sense of dreaming and are not distressed by the experience.5 However, some patients experience pain, which is occasionally severe. In a study involving 11 785 patients who had received general anesthesia, the incidence of awareness was 0.18% in cases in which neuromuscular blockers were used and 0.10% in the absence of such drugs.3 Of the 19 patients who experienced recall, 7 (36%) reported some degree of pain, ranging from soreness in the throat because of the endotracheal tube to severe pain at the incision site.3 Patients may remember these events immediately after surgery, or hours or days later.3 According to a study by Samuelsson and colleagues, most cases of awareness are inconsequential, but some patients experience prolonged and unwanted outcomes, including post-traumatic stress disorder or depression.6 Late psychological symptoms, including nightmares, anxiety and flashbacks, occurred in 15 of 46 patients (33%) who experienced awareness.6 Reports of intraoperative awareness generally apply only to patients who have received general anesthesia, since painless auditory recall by patients receiving regional (e.g., epidural) anesthesia is not surprising. Patients who receive regional anesthesia often receive medication for sedation and anxiolysis but are usually arousable.
In 2006 the Task Force on Intraoperative Awareness, established by the American Society of Anesthesiologists, released a “Practice Advisory for Intraoperative Awareness and Brain Function Monitoring.”7 The advisory identified certain patient characteristics and surgical factors that increase the risk of intraoperative awareness. Patient-related factors include age, limited cardiac reserves, drug resistance or substance abuse (including the long-term use of benzodiazepines, cocaine or alcohol) and a history of difficult intubation or previous episodes of intraoperative awareness. Certain procedures are associated with increased risk, including cesarean section, cardiac surgery, trauma surgery and procedures for which muscle relaxants are used. Preoperative consultation may be helpful in identifying patients who will be at risk for intraoperative awareness.
The causes of intraoperative awareness are as yet unknown, and the problem may be multifactorial. At least 4 broad categories of causes are plausible. First, unexpected patient-specific variability in dose requirements of anesthetic drugs may be a result of altered expression or function of target receptors. Second, patients may be unable to tolerate a sufficient dose of anesthetic because of low physiologic reserves related to factors such as poor cardiac function or severe hypovolemia. Third, physiologic characteristics that would indicate the need for a dose change may be masked by factors such as use of β-adrenergic receptor blockers or presence of a pacemaker. Fourth, intended drug delivery systems may be compromised by events such as equipment malfunction or misuse. Of these, the first category would be especially distressing because the patient would be exposed to a seemingly adequate dose of an anesthetic, but the resulting depth of anesthesia would be inadequate.
The reasons why some patients require a higher dose of anesthetic than others remain unknown and may be multifactorial (Figure 1). In preclinical studies involving mice, Cheng and colleagues found that a genetic deficiency in one type of receptor for the inhibitory neurotransmitter γ-aminobutyric acid (receptors that contain the α5 subunit) conferred resistance to the memory-blocking properties of the anesthetic etomidate.8 These receptors are predominantly expressed in the hippocampus, a region of the brain that is critically involved in memory. In wild-type mice, the anesthetic was found to impair memory and learning; however, this impairment did not occur in genetically modified mice that lacked these receptors. Other preclinical studies have shown that the expression of this memory-blocking receptor changes after long-term exposure to alcohol or persistent seizures.9,10 Concurrent medications may also adversely affect the metabolism and distribution of anesthetic agents. Polymorphisms for the γ-aminobutyric acid A receptor 5 gene (GABRA5) exist in the human genome, and there are at least 3 distinct messenger RNA isoforms in human adult and fetal brain tissue.11 The functional consequences and prevalence of these variations remain unknown. Human studies have shown that the immobilizing dose of anesthetic may vary by as much as 24% in populations with different genetic backgrounds.12 Thus, pharmacogenetics may be one factor contributing to intraoperative awareness.
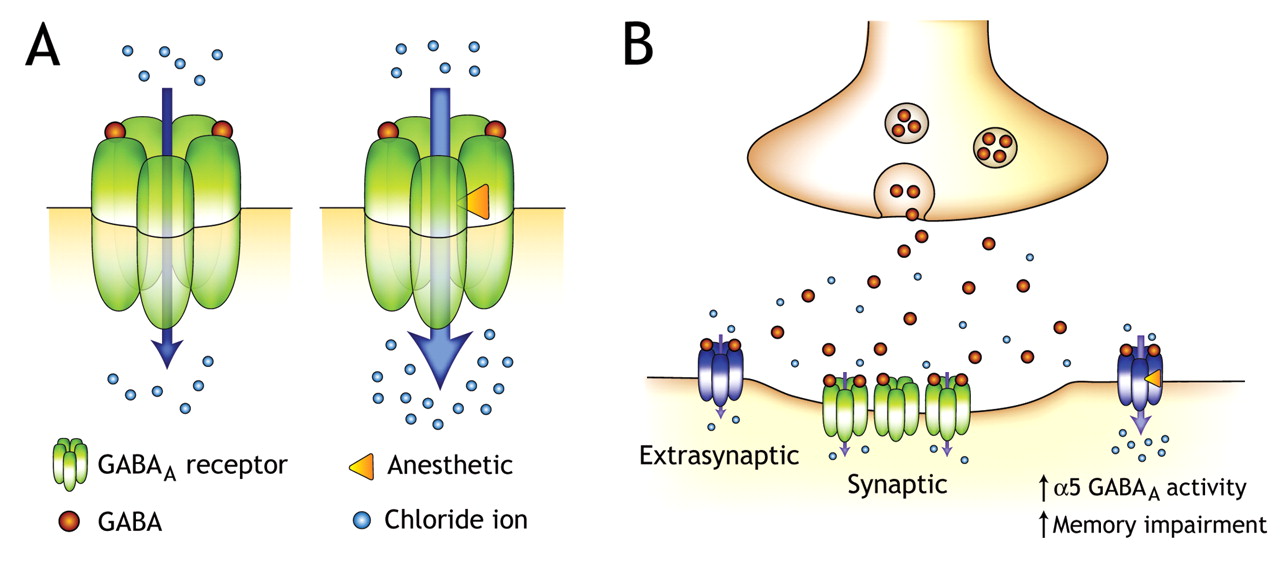
Figure 1: Effect of anesthetics on neurotransmission in the brain. A: When γ-aminobutryic acid (GABA) binds to the GABAA receptor, a pentameric ion channel, it causes a conformational change that opens the channel pore and allows the flux of chloride ions across the cell membrane. Many general anesthetics, barbiturates and benzodiazepines increase the potency of GABA at the GABAA receptor level and thereby increase chloride flux. Generally, this causes membrane hyperpolarization and a reduction in the excitability of neurons. B: Learning and memory during anesthesia, like other forms of memory, are processed via specific brain structures, particularly the hippocampus. Normal function in these structures depends on a delicate balance between excitatory and inhibitory neurotransmission. Synaptic GABAA receptors are the primary mediators of inhibitory neurotransmission. Extrasynaptic GABAA receptors are also present, have a unique subunit composition and are particularly sensitive to modulation by general anesthetics. Sustained inhibition via enhanced activation of these extrasynaptic receptors may contribute to the memory-blocking properties of anesthetics. Ongoing research is evaluating whether genetic variations in GABAA receptor structure among individuals account for variable sensitivity to anesthetics. Modified with permission from Elsevier (Pharmacol Biochem Behav).17 Image by: Robert Bonin
What can be done to reduce the incidence of intraoperative awareness? Awareness results in part from the inability to accurately measure the depth of anesthesia. This is especially true for the memory-blocking component of anesthesia. The dose of anesthetic is best adjusted by an experienced anesthesiologist, who relies on a multitude of parameters to judge the degree of anesthesia, including patterns in heart rate, blood pressure, lacrimation and movement. Standard intraoperative monitoring devices measure pulse oximetry; noninvasive blood pressure; electrical activity in the heart; airway pressure; and the concentrations of oxygen, carbon dioxide and anesthetic vapour. Unfortunately, episodes of awareness have occurred with no changes in hemodynamic parameters. To supplement the clinical signs, monitors have been developed to measure the electrical activity in the brain while the patient is anesthetized. These monitoring systems can be divided into 2 broad groups: those that analyze electroencephalographic activity using electrodes placed on the patient's forehead and those that acquire and analyze evoked responses to auditory stimuli. Some devices also analyze electromyographic activity recorded from scalp muscles. The electrical activity measured by these devices does not directly quantify the level of consciousness or memory, but it may indicate associated neuronal processes. Also, the values measured by these devices do not have uniform sensitivity across different anesthetic drugs, combinations of drugs or types of patients.
Intraoperative awareness may occur even when monitoring devices are in use. A recent study by Myles and colleagues5 suggested a lower incidence of awareness among high-risk patients monitored with the Bispectral Index system (Aspect Medical Systems, Norwood, Massachusetts). A prospective nonrandomized cohort study involving 19 575 patients was designed by Sebel and colleagues to establish the incidence of awareness with recall during routine general anesthesia and to determine Bispectral Index values associated with intraoperative awareness. The authors found no statistically significant difference when the monitor was used (0.18% of patients) compared with when it was not used (0.10% of patients).2 Uncritical and widespread reliance on brain monitors could result in certain patients not experiencing awareness but being compromised by relative overdose. Conversely, other patients might receive insufficient doses. In the “Practice Advisory for Intraoperative Awareness and Brain Function Monitoring,” the consensus opinion based on the medical literature and on responses from consultants and members of the American Society of Anesthesiology was that brain function monitoring is not routinely indicated for patients receiving general anesthesia, either to reduce the frequency of intraoperative awareness or to monitor the depth of anesthesia.7 In response to the statement, “Brain function monitors are valuable and should be used to reduce the risk of intraoperative awareness for patients with conditions that may place them at risk for intraoperative awareness,” about 63% of consultants agreed or strongly agreed with the statement, compared with 14% who were uncertain, 14% who disagreed, or 9% who strongly disagreed. This task force report was explicit in indicating that it was intended only as a practice advisory rather than a practice standard because of the lack of sufficient numbers of controlled studies needed to make firm recommendations. The practice advisory also recommended the use of benzodiazepines for prophylactic amnesia for high-risk patients, but the decision to use this therapy should be made on a case-by-case basis.7
If intraoperative awareness does occur, the patient should be assessed, reassured and referred back to the anesthesiologist for follow-up care. Episodes of awareness should be addressed in a frank and expert manner. This begins with a discussion aimed at understanding and documenting the patient's experience and identifying contributing factors. If appropriate, the anesthesiologist should provide an explanation of why the awareness occurred and reassurance that the likelihood of a recurrence is slim. The patient should be instructed to inform future anesthesiologists about the event. Some patients should be referred for ongoing supportive care and psychological counselling.
Gaps remain in our understanding of how general anesthetics modify memory and consciousness. Indeed, the biological basis and specific brain regions that contribute to consciousness and various forms of memory remain to be elucidated. Large-scale studies of the efficacy of brain-monitoring devices in the prevention of awareness are required. At present, no monitor can guarantee that a patient is unaware while receiving a general anesthesia. It is also necessary to learn more about patients' experiences of intraoperative awareness. The American Society of Anesthesiologists has established a registry for patients who experience awareness (www.AwareDB.org). The program will provide information on patients' understanding of awareness and on their perspectives of how anesthesiologists might effectively intervene when patients have experienced intraoperative awareness. The registry is now enrolling patients who will complete a survey about their experiences and, if requested, submit copies of their medical records for analysis. The registry has a federal certificate of confidentiality to protect the privacy of those who participate. Other studies are required to determine whether alterations in specific gene products, such as anesthetic target receptors, are linked to awareness. If so, genetic screening might help to identify patients at risk for intraoperative awareness. Improved education is needed to understand intraoperative awareness and the ability of medical personnel to manage such an event — an ability that is often poor or lacking.13 Several sources of information are available, including reviews7,14–16 and a patient information pamphlet from the American Society of Anesthesiologists (www.asahq.org/patientEducation/Awarenessbrochure.pdf). A briefing on awareness will soon be available on the Canadian Anesthesiologists' Society website (www.cas.ca).
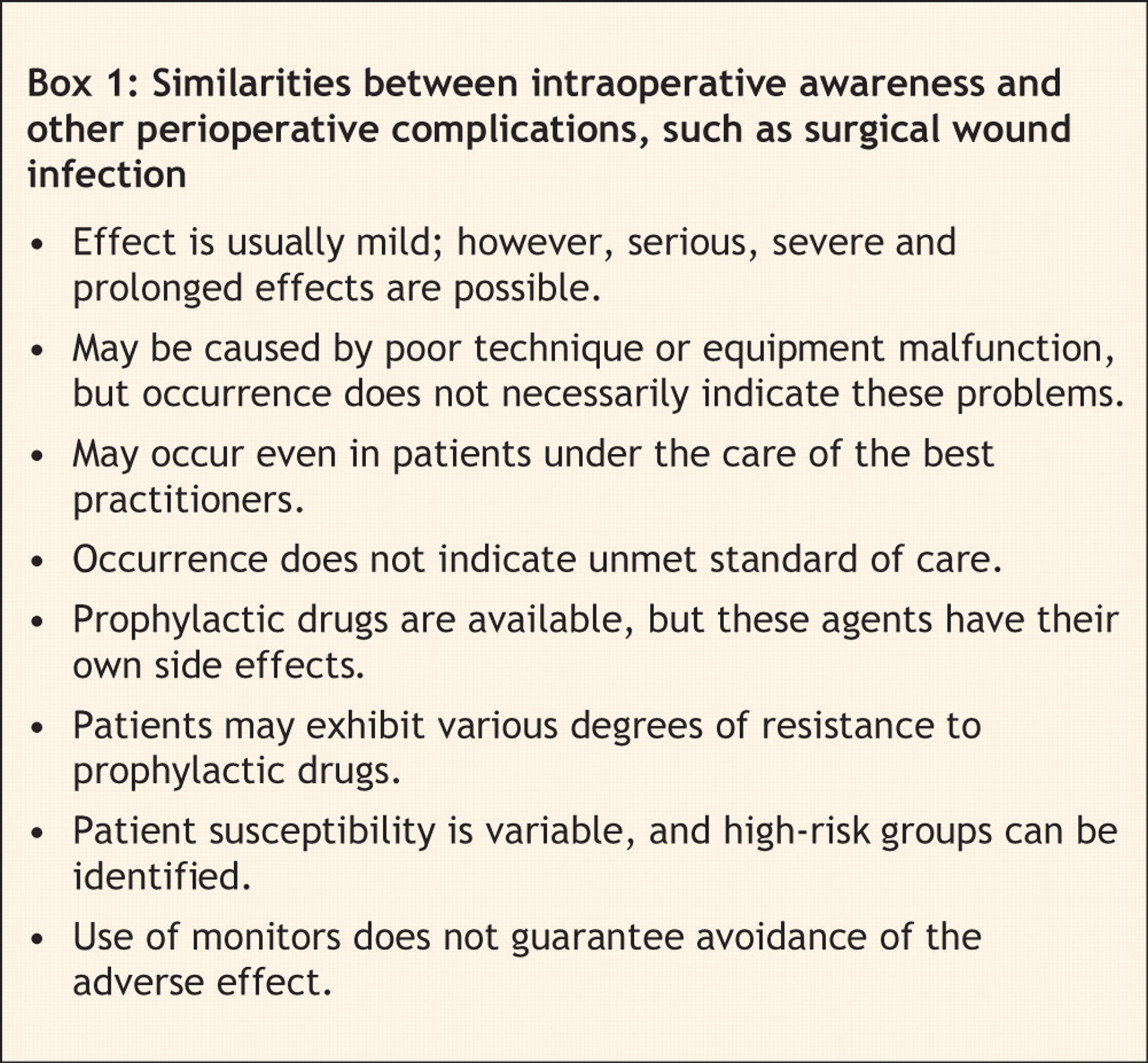
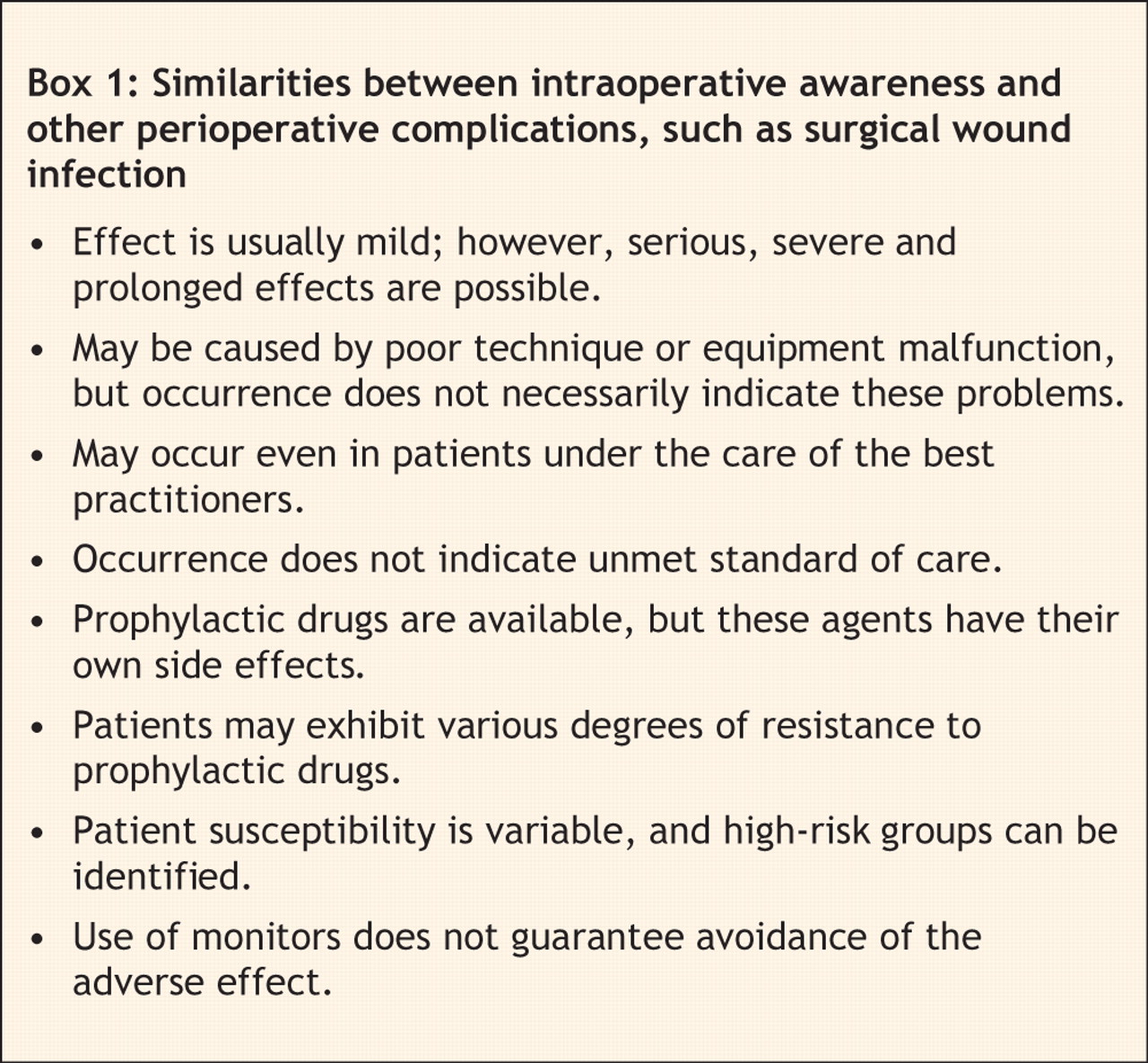
In summary, immense efforts have been made to understand the effects of anesthetics on physiologic processes and to develop strategies and technologies to manage the adverse effects of these drugs. As a result, general anesthesia is relatively safe, to such an extent that patients (and even physicians) often discount the associated risks. However, certain risks remain, including the possibility of intraoperative awareness. Intraoperative awareness should be viewed as a recognized risk, with many features similar to those of intraoperative and perioperative events, such as surgical wound infection (Box 1). As champions of patient safety, anesthesiologists are directing research and patient care efforts toward reducing the incidence and consequences of this adverse event.
Key points of the article
• Intraoperative awareness, which is the unexpected recall of events that occur during anesthesia by patients who receive general anesthesia, occurs in up to 1 to 2 per 1000 patients. Most patients do not experience pain but, rather, have vague recall of auditory events or dreaming. However, approximately 36% of patients who experience recall report some degree of pain, which is occasionally severe.
• Risk factors for awareness include patient age, cardiac reserve and substance abuse. Procedures associated with increased risk include cardiac and trauma surgery and cesarean section.
• Preventative strategies include monitoring by a skilled anesthesiologist and possibly the use of benzodiazepines. Current neurophysiologic monitors aimed at estimating the depth of anesthesia are not recommended for routine use.
Footnotes
-
Contributors: All authors contributed substantially to the conception and content of the article, drafted and revised the manuscript critically for important intellectual content and approved the final version for publication.
Acknowledgements: The authors thank Brian Kavanagh, professor and chairman, Department of Anesthesia, University of Toronto, for his suggestions and criticism of the manuscript and Robert Bonin, PhD candidate, Department of Physiology, University of Toronto, for creating the figure. The studies of GABAA receptors described were supported by the Canadian Institutes of Health Research.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

