


A baby girl was born at 31 weeks' gestation after an uneventful pregnancy. She weighed 1480 g, and her Apgar score was 2 at 1 minute and 6 at 5 minutes. Within minutes of being born, her respiratory rate was 61 (normal 20–40) breaths/min, with significant nasal flaring, prominent accessory muscle use and subcostal retractions. Her heart rate was normal (121 beats/min). There were signs of cyanosis, and the infant was admitted to the neonatal intensive care unit with a tentative diagnosis of transient tachypnea of the newborn (TTN).
Results of her bloodwork were within normal limits. A chest radiograph showed prominent perihilar interstitial thickening and fluid in the transverse fissure consistent with TTN. Mechanical ventilation was started and no feeding was given for 2 days, after which the patient was weaned successfully from her oxygen and the ventilation tube removed. However, 2 hours later she had increased difficulty breathing, with subcostal retractions, and required intubation a second time. After weaning to room air and extubation, her respiratory distress recurred over the next few hours. Bronchoscopy excluded congenital lower airway lesions or post-intubation injury.

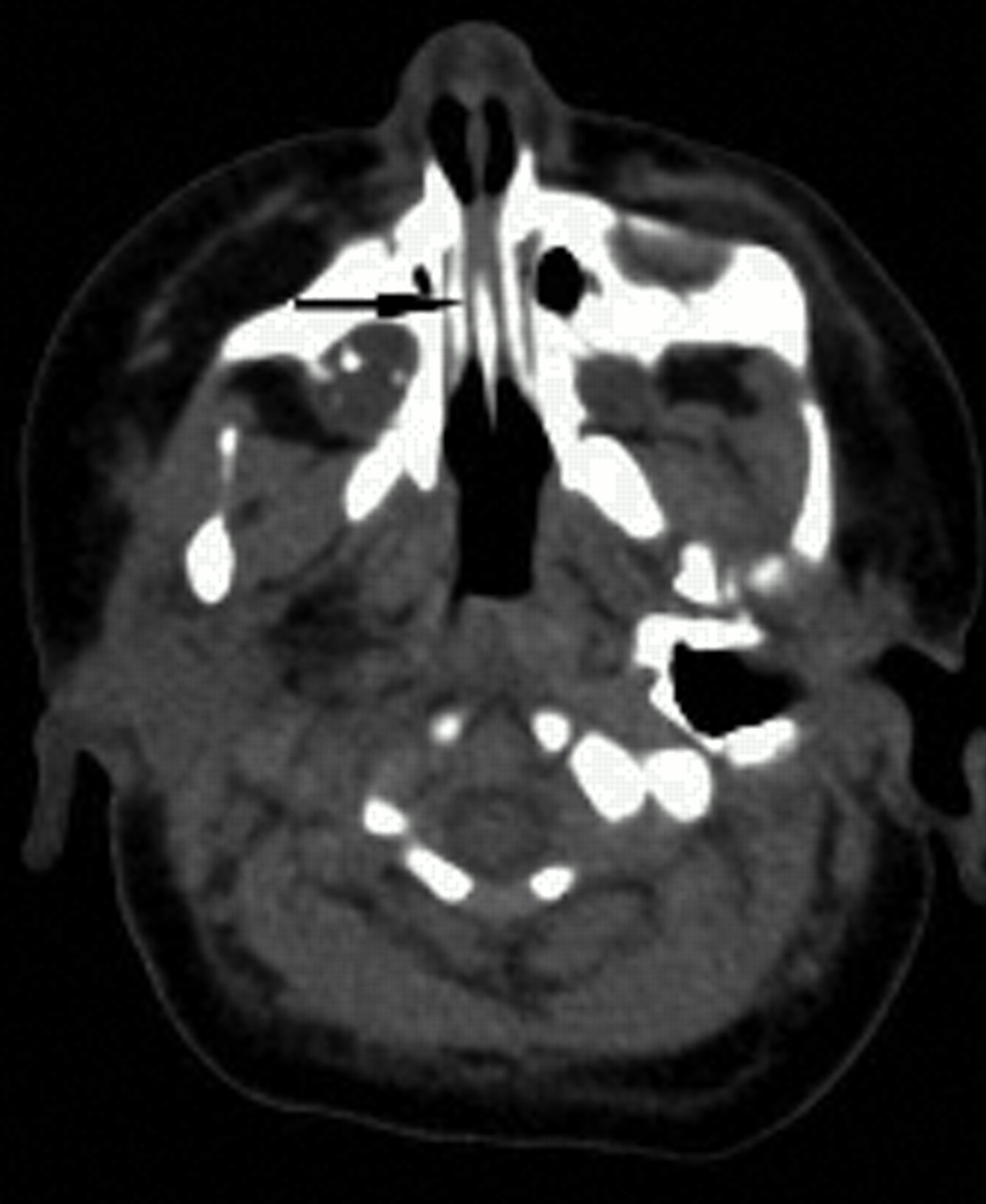
Fig. 1: Axial CT scan, showing bilateral midnasal stenoses (arrow).
A nurse performing routine nasal suctioning noted how tight the patient's nasal passages were. An axial nasal CT scan confirmed bilateral bony midnasal stenoses (Fig. 1, arrow). We progressively dilated the stenoses by inserting gradually larger endotracheal tubes and leaving them in place (no. 2.5 tube for 5–7 days, no. 3 tube for 5– 7 days, and then no. 3.5 tube for about 3–4 weeks) (Fig. 2). During this time the patient received gavage feeding. The intervention greatly eased her breathing. The tubes were removed, and the patient was sent home breathing room air and thriving without subsequent respiratory difficulty.

Fig. 2: An endotracheal tube was inserted into each nostril to dilate the midnasal stenoses. The tip of the tubes are estimated to be at the nasopharyngeal level.
Neonates have to breathe through their nose because the entire length of their tongue abuts against the hard and soft palates, and because the high position of their epiglottis (at the level of the third and fourth cervical vertebrae compared with the fifth and sixth vertebrae in adults) causes increased resistance of the oral airway.
The nasal passages can be divided into 3 anatomic regions: pyriform aperture, middle nasal cavity and posterior choana. Anterior nasal obstructions are usually due to isolated pyriform aperture stenoses or a lack of cleavage of the frontal hemispheres, which results in holoprosencephaly in addition to a central maxillary incisor. Posterior obstructions, such as bilateral choanal atresia, are usually part of the CHARGE association (a syndrome of associated birth defects, including coloboma of the eye, heart anomaly, choanal atresia, growth retardation, and genital and ear anomalies).
Midnasal obstructions are often due to nasal edema from inflammation and infections.1 Isolated midnasal stenoses are uncommon and occur in patients with genetic syndromes with midface hypoplasia, such as fetal alcohol syndrome, Crouzon's disease and Apert's syndrome. However, our patient did not have any of these anomalies. Rare causes of midnasal stenosis include tumour, cyst or encephalocele.2
Children with complete nasal obstructions usually present with cyclic cyanosis, made worse by feedings but relieved by crying;3 however, the cause of the respiratory distress can sometimes be delayed in children who have undergone endotracheal intubation and given gavage feedings (as in our patient). Nasal obstruction should be suspected if a no. 5 French catheter is not easily passed through the nostrils during airway suctioning or placement of a nasogastric feeding tube.
Midnasal stenosis can be managed immediately by suctioning airway secretions, humidifying nasal passages with saline nasal drops and using gavage feeding. An oral airway can be maintained temporarily with a McGovern nipple (a large synthetic nipple similar to that used on a feeding bottle but with its end cut off) inserted and held in place by tying it around the baby's occiput. By 6 months of age, the baby's midface has usually grown sufficiently that interventions are rarely required past this point. Because of our patient's recurrent episodes of respiratory failure, we opted to dilate her nasal passages progressively rather than use expectant treatment.
Footnotes
-
Competing interests: None declared.
In this issue
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

