Article Text

Statistics from Altmetric.com
- DSE, dobutamine stress echocardiography
- LV, left ventricle
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SPECT, single photon emission computed tomography
In recent years, it has become evident that myocardial dysfunction in ischaemic heart disease is not always a result of infarction and that contractile function can improve significantly after revascularisation.12 A number of non-invasive techniques have been developed in an attempt to identify these patients with dysfunctional but viable myocardium, since it is generally agreed that it is this group, as compared to the group with irreversible myocardial damage, that has a favourable clinical risk-to-benefit profile for undergoing coronary revascularisation. The primary aim of these non-invasive techniques is to provide a regional map of the heart in which the amount of viable myocardium is quantified. Unfortunately, currently available techniques, such as single photon emission computed tomography (SPECT), dobutamine stress echocardiography (DSE), and positron emission tomography (PET), have various limitations. For example, what is measured may not be the direct presence and exact quantity of viable myocytes, but a physiologic parameter, such as contractile reserve or perfusion, that has only an indirect relation to viability. Other limitations related to the specific technique include partial volume effects due to poor spatial resolution (SPECT, PET), attenuation and scatter artefacts (SPECT), errors in registration between comparison images (DSE), and the occasional inability to visualise all parts of the left ventricular myocardium (DSE).
In this article we will re-examine some fundamental concepts in the assessment of myocardial viability. We propose that even if a technique were available that could provide direct quantification of regional viability without technical limitations (no artefacts, infinite spatial resolution, etc), there would still be insufficient information to provide a comprehensive assessment of viability and thus insufficient information to provide the highest accuracy in predicting wall motion improvement or clinical benefit after coronary revascularisation. Certainly, there are additional factors that are not related to limitations in non-invasive testing that could reduce accuracy in predicting functional improvement. These have been well described and include perioperative or postoperative occult myocardial infarction, incomplete revascularisation as a result of diffuse atherosclerotic disease, or tethering of regions with extensive scarring adjacent to viable regions.34 For the purposes of this article we will not consider these clinical factors, but instead focus on issues related to the non-invasive assessment of viability. We will examine the hypothesis that “knowing how much is alive is not enough”. We will provide examples to support this argument and suggest potential solutions.
CONCEPT 1: NORMAL HEARTS HAVE SIGNIFICANT REGIONAL VARIABILITY IN THE TRANSMURAL EXTENT OF VIABLE MYOCARDIUM
It is known that there can be significant variation in diastolic wall thickness at different points around the left ventricle (LV). This variation occurs even if papillary muscles are excluded and healthy volunteers are studied.56 This observation then naturally proceeds to the conclusion that there can be significant variability in the transmural extent of viable myocardium at different locations of the normal LV. The images from patient A in fig 1 demonstrate this concept. The left panel (top row) shows a delayed contrast enhanced magnetic resonance image of a patient with a normal heart. Using this technique, regions of myocardial infarction or scar appear bright or “hyperenhanced”, while areas of viable myocardium appear black.78 In this image, which shows a mid ventricular short axis view during diastole, all myocardial regions appear black and thus are 100% viable. In the middle panel (top row) the LV endocardial and epicardial contours have been traced. Since the myocardium is fully viable, the diastolic wall thickness is equivalent to the transmural extent of viability for all myocardial regions. The right panel (top row) demonstrates wall thickness (or extent of viability) as a function of LV location as one progresses from the anterior wall (12 o’clock) counterclockwise to the inferior wall (arrow) and back to the anterior wall. In this normal heart, it is obvious that there is significant heterogeneity in the transmural extent of viable myocardium, with as much as 12 mm of viable myocardium in the portion of the inferior wall adjacent to the posterior papillary muscle and as little as 7 mm in the anteroseptal wall at the right ventricular insertion site.
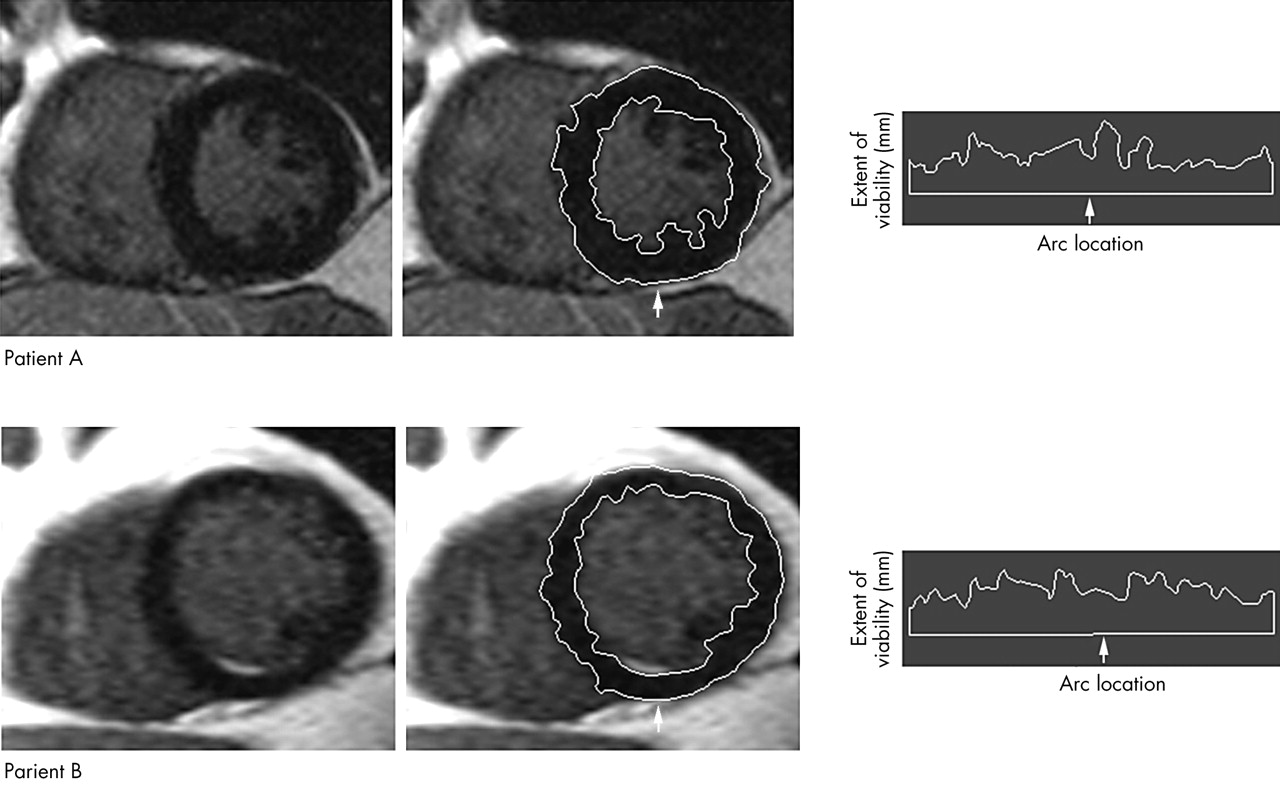
Regional variation in the absolute amount of viable myocardium in a patient with a normal heart (A), and a patient (B) with a subendocardial inferior wall infarction. See text for details.
This heterogeneity in the extent of viable myocardium has direct clinical implications. For example, a region with 70% the viability of the region with the maximum amount of viability may represent either a normal region with 70% the wall thickness of the thickest region or a region with a subendocardial myocardial infarction. The images from patient B in fig 1 underscore this concept. This particular patient had a clinically documented myocardial infarction caused by occlusion of the right coronary artery which was reopened during primary angioplasty. In the left panel (bottom row) the contrast enhanced magnetic resonance image (MRI) demonstrates a small subendocardial region of hyperenhancement in the inferior wall (arrow) which denotes the presence of subendocardial infarction. In the middle panel (bottom row), endocardial and epicardial contours have again been traced on the contrast enhanced MRI image similar to that in patient A. One difference, however, should be noted. The endocardial contour is along the border of viable myocardium (black myocardium), thus, the infarcted region is not included. The right panel (bottom row) correspondingly demonstrates the transmural extent of viability along the circumferential profile of the heart. Note that in this patient, the intrinsic variation in the extent of viable myocardium for non-infarcted regions is greater than the reduction in viable myocardium for the region with subendocardial infarction, thus rendering the subendocardial infarction “invisible” by techniques that can only assess viable myocardium.
These two patient examples highlight the differences between techniques that can visualise only viable myocardium as opposed to techniques that can visualise viable and infarcted myocardium. Additionally, it is important to recognise that the use of different techniques often leads to differences in the way in which viability is quantified, although the nomenclature used may be the same. For example, when only viable myocardium is assessed, the “percentage of viable myocardium” in a given segment generally refers to the amount of viability in the segment normalised to the segment with the maximum amount of viability, or to data from a sex specific database of normal controls. Conversely, when both viable and infarcted myocardium are assessed, the “percentage of viable myocardium” in a given segment generally refers to the amount of viability in the segment normalised to the total amount of viability plus infarction in the same segment. These differences in the way in which viability is quantified can alter clinical interpretation. For the normal heart in patient A, the first method would show that there is significant regional variability in the extent of viable myocardium (60–100% of maximum viability), whereas the second method would show essentially no variability since all segments would be classified as 100% viable. Likewise for patient B, the first method would not be able to identify the region of subendocardial infarction since the extent of viable myocardium is within the normal variation of non-infarcted myocardium; however, the second method would clearly identify the region with subendocardial infarction since this region would be the only region with less than 100% viable myocardium.
As expected, recent studies have indicated that subendocardial infarcts are routinely missed by assessment of wall motion, thallium SPECT, sestamibi SPECT, and PET.9–11 One might presume, however, that the detection of subendocardial infarcts has little clinical relevance to the determination of myocardial viability since by definition the majority of myocardium is viable. Although strictly true, the inability to detect subendocardial infarction is only a symptom of a larger problem—that is, that there is a level of uncertainty regarding the regional presence and extent of non-viable myocardium when only viable myocardium can be assessed. For example, a segment with an average 5 mm thickness of viable myocardium may be a rather thin segment (for example, 7 mm thick) with 2 mm of subendocardial infarction, or a thicker segment (for example 11 mm thick) with 6 mm of subendocardial infarction. In these two possibilities, the absolute level of viability is the same (that is, 5 mm); however, the extent of viability as a percentage of the wall thickness is 71% (5/7) in the first situation, and 45% (5/11) in the second. We propose that the first situation is more likely than the second to result in contractile improvement following revascularisation. This issue will be discussed further in the following section.
CONCEPT 2: REGIONS WITH THINNED MYOCARDIUM MAY BE VIABLE
Prior studies have indicated that in patients with coronary artery disease and ventricular dysfunction, regions with thinned myocardium represent scar tissue and cannot improve in contractile function after coronary revascularisation.1213 In fact Cwajg and colleagues13 conclude that a “measurement of end diastolic wall thickness less than or equal to 6 mm virtually excludes the potential for recovery of function”. One should be aware, however, that there are no prospective randomised trials which have evaluated the role of non-invasive viability testing in patients who are potential candidates for revascularisation. All published studies, so far, represent small retrospective, observational series of patients. As stated in a recent editorial on the subject: “under these circumstances, one cannot ignore the distinct potential for important patient selection biases, related to symptoms, LV function and angiographic severity of CAD.”14
Contrary to the existing literature, we propose that myocardial thinning should not be equated with the lack of myocardial viability, and that in some patients, these regions can improve in contractile function after revascularisation. Although data are lacking on this subject, we will demonstrate a patient case that strongly suggests that this hypothesis is correct.
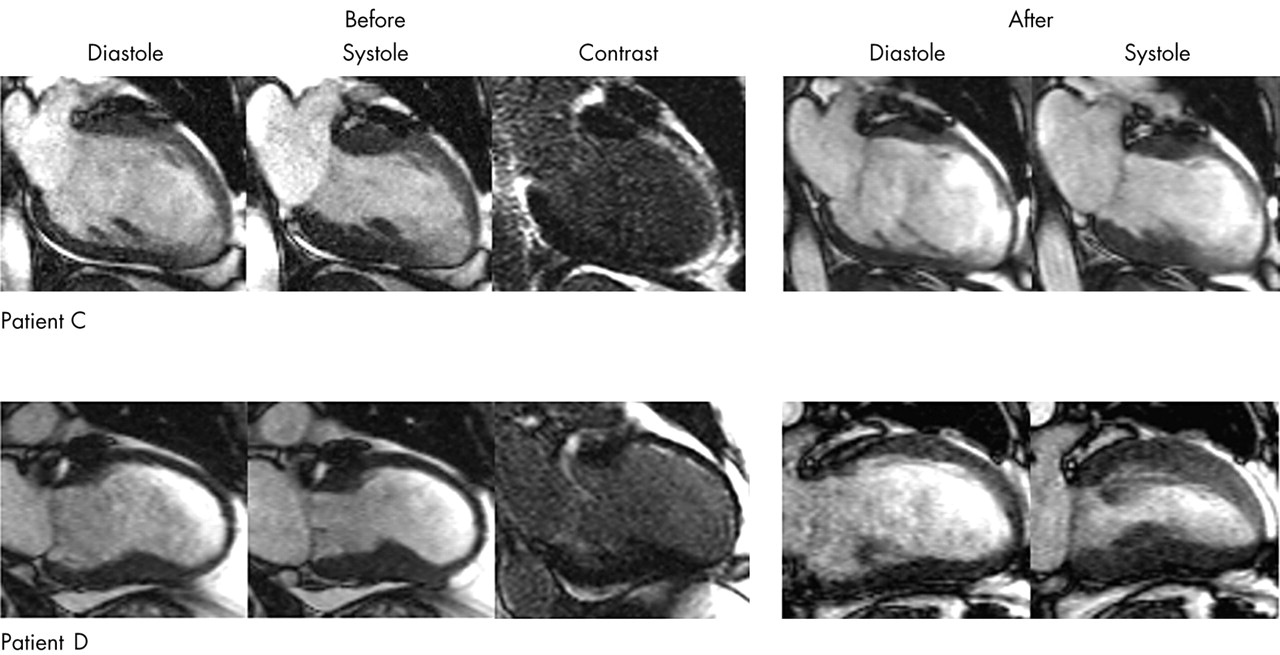
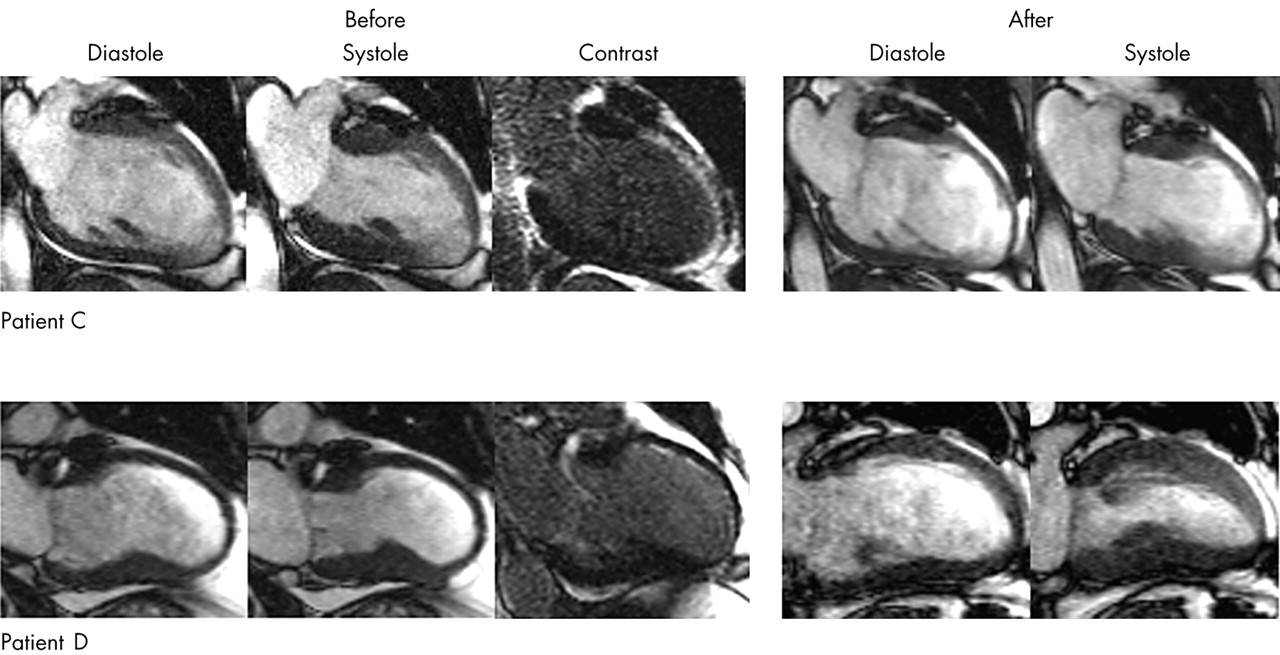
Figure 2 shows MRI images of two patients (C and D) who both have significant coronary artery disease and chronic LV dysfunction. The left hand panels represent long axis cine images acquired before coronary revascularisation (full motion cine images may be viewed at http://dcmrc.mc.duke.edu/heart/). Two points should be noted on these images. First, both patients have severe regional dysfunction of the anterior wall with near akinesis occurring in patient C (top row) and dyskinesis in patient D (bottom row). Second, patient D has associated thinning of the anterior wall (diastolic wall thickness of 5.0 mm) while patient C does not (diastolic wall thickness of 8.0 mm). Based on these cine images and the existing literature, one might expect that there is more viable myocardium in the anterior wall of patient C than in patient D, and in fact question the need for viability testing at all in patient D since the thinned, dyskinetic anterior wall must undoubtedly be scar tissue and thus non-viable. The contrast enhanced MRI images acquired before revascularisation (middle panels), however, indicate a different clinical interpretation. In patient C, there is a bright endocardial rim of hyperenhancement (infarction) that measures on average 4.5 mm in thickness. The remaining epicardial rim of tissue which is black (viable) measures 3.5 mm in thickness (total thickness 8 mm). In patient D, there is also an endocardial rim of hyperenhancement, but it measures on average only 1.5 mm in thickness. The epicardial rim which is viable measures 3.5 mm in thickness (total thickness 5 mm). Note that in both patients the absolute amount of viable myocardium is the same (3.5 mm); however, when the extent of viability is expressed as a percentage of the total amount of myocardium in the segment, patient C has less than 50% viable myocardium (3.5/8, 44%) whereas patient D has greater than 50% viable myocardium (3.5/5, 70%). The right hand panels in fig 2 represent cine images acquired two months after coronary revascularisation. Patient C exhibits no improvement in contractile function in the anterior wall and in fact develops diastolic wall thinning in this region. Conversely, patient D exhibits not only significant improvement in contractile function in the anterior wall, but also recovery of diastolic wall thickness in this region (from 5 mm to 9 mm).
{kind=link}
{kind=link}
Cine and contrast enhanced MRI images of two patients (C and D) before coronary revascularisation and cine images two months after revascularisation (full motion cine images may be viewed at http://dcmrc.mc.duke.edu/heart/). See text for details.
Three fundamental points are raised by these patient examples. First, it is apparent that a method that can quantify only viable myocardium, even if technically flawless (infinite spatial resolution, no attenuation artefacts, etc), provides insufficient information to allow a comprehensive assessment of myocardial viability. Since both patients had the same reduced amount of viable myocardium (3.5 mm thick), we would have predicted, incorrectly as it turns out, that both patients would not improve in contractile function following revascularisation. Second, it is evident that the absolute amount of viable myocardium in a given region is dynamic and can increase or decrease as a result of ventricular remodelling. Whereas it is common knowledge that myocardial viability can decrease—for example, due to myocardial infarction with associated wall thinning—the reverse process in which regions of thin myocardium become thick with an absolute increase in the transmural extent of viability (as in patient D) has not been previously described. Third, it appears that quantification of non-viable myocardium in addition to viable myocardium is important in predicting contractile improvement following revascularisation. For example, incorporating information regarding non-viable myocardium into a ratio of viable to total myocardium (viable plus non-viable) within the same region would lead to the conclusion that the anterior wall of patient D has a higher percentage of viable myocardium (70%) than patient C (44%) and thus is more likely to improve in contractile function. The follow up cine images in fig 2 demonstrate that this prediction is correct.
SUMMARY
In this article we have re-examined some fundamental concepts in the assessment of myocardial viability. Although counterintuitive, we have explored the proposal that “knowing how much is alive is not enough” to provide a comprehensive assessment of myocardial viability. In part, we believe this is the consequence of two physiological precepts. First, normal hearts have significant regional variability in the transmural extent of viable myocardium. This intrinsic heterogeneity leads to uncertainty regarding the presence and extent of non-viable myocardium when using a technique that is able to detect or assess only viable myocardium. Second, for a given region, the absolute amount of viable myocardium may be dynamic and thus decrease or increase over time. A patient example was demonstrated in which a “thinned” anterior wall nearly doubled in diastolic wall thickness following coronary revascularisation. For this patient, the ratio of viable to total myocardium (viable plus non-viable) in the dysfunctional region was more accurate that the absolute amount of viable myocardium alone in predicting functional improvement. It was postulated that non-invasive methods should identify and assess non-viable myocardium as well as viable myocardium since the combined data appear to provide a more accurate and comprehensive evaluation of myocardial viability.
Acknowledgments
Supported in part by NIH, R01-HL64726 (RJK)
REFERENCES
Linked Articles
- Mini-symposium
- Miscellanea