Assessment and management of cannabis use disorders in primary care
BMJ 2010; 340 doi: https://doi.org/10.1136/bmj.c1571 (Published 01 April 2010) Cite this as: BMJ 2010;340:c1571
- Adam R Winstock, clinical senior lecturer, honorary consultant psychiatrist1,
- Chris Ford, clinical director2, general practice principal3,
- John Witton, research coordinator1
- 1National Addiction Centre, Institute of Psychiatry, King’s College London, London SE5 8AF
- 2Substance Misuse Management in General Practice (SMMGP), c/o NTA, Skipton House, London SE1 6LH
- 324 Lonsdale Road, London NW6 6SY
- Correspondence to: A R Winstock Adam.winstock{at}kcl.ac.uk
Summary points
Cannabis use is common, especially among young people
The greatest risk of harm from cannabis use is in young people and those who are pregnant or have serious mental illness
A tenth of cannabis users develop dependence, with three quarters of them experiencing withdrawal symptoms on cessation
Most dependent users have concurrent dependence on tobacco, which increases the health risks and worsens outcomes for cannabis treatment
Brief interventions and advice on harm reduction can improve outcomes
Psychoeducation (for a better understanding of dependence), sleep hygiene, nicotine replacement therapy (where indicated), and brief symptomatic relief form the mainstay of withdrawal management
Dependent users may present with symptoms suggestive of depression, but diagnosis and treatment should be deferred until two to four weeks after withdrawal to improve diagnostic accuracy
About a third of adults in the UK have tried cannabis, and 2.5 million people, mostly 16-29 year olds, have used it in the past year.1 Although most people who smoke cannabis will develop neither severe mental health problems nor dependence, regular use of cannabis may be associated with a range of health, emotional, behavioural, social, and legal problems, particularly in young, pregnant, and severely mentally ill people.2 3 The past decade has seen a shift in available cannabis preparations from resinous “hash” to intensively grown high potency herbal preparations, often referred to as skunk, which now dominates the UK market.4 Compared with traditional cannabis preparations, skunk tends to have higher levels of tetrahydrocannabinol, the main psychoactive constituent of cannabis, and lower levels of the anxiolytic cannabinoid cannabidiol. In January 2009 cannabis was returned to its original class B classification (from class C) under the UK Misuse of Drugs Act.
Despite high levels of use, only 6% of those seeking treatment for substance misuse in England cite cannabis as their major drug of concern, and most of those with cannabis use disorders do not have cannabis use as their presenting complaint (box 1).5 Low levels of treatment seeking may reflect a lack of awareness of the associated harms of cannabis.w1 This review highlights the adverse health outcomes associated with cannabis and outlines optimal approaches to assessing and managing cannabis use in primary care.
Box 1 What problems might cannabis users present with in primary care?
Respiratory problems, such as exacerbation of asthma, chronic obstructive airways disease, wheeze or prolonged cough, or other chest symptoms
Mental health symptoms, such as anxiety, depression, paranoia, panic, depersonalisation, exacerbation of an underlying mental health condition
Problems with concentration while studying or with employment and relationships
Difficulties stopping cannabis use
Legal or employment problems (arising from use of cannabis)
Methods
We searched electronic databases, including Medline and PsycINFO; the Cochrane Library; specialist websites; databases of England’s National Treatment Agency for Substance Misuse and of the UK centre DrugScope; the US National Institute on Drug Abuse; the European Monitoring Centre for Drugs and Drug Addiction; and Australia’s National Cannabis Prevention and Information Centre. We also consulted primary care providers and specialists in addiction treatment.
How does cannabis exert its effect?
Metabolites of cannabis act on the body’s endogenous cannabinoid system via type 1 cannabinoid receptors (CB1 receptors) in the central nervous system and CB2 receptors peripherally. They may modulate mood, memory, cognition, sleep, and appetite.w2
What are the effects of intoxication?
Most people smoke cannabis for its relaxant and euphoriant effects (box 2). The impact of higher potency cannabis will depend partly on its ratio of tetrahydrocannabinol to cannabidiol and whether users are able and willing to titrate their consumption as they might alcohol.3 6 The authors of a recent review suggested that more potent forms may increase the risk of dependence and adverse psychological experiences.3
Box 2 Physiological and psychological effects of cannabis*
Psychological (mood/perceptual) effects
A sense of euphoria and relaxation
Perceptual distortions, time distortion, and the intensification of sensory experiences
Impairment of attention, concentration, short term memory, information processing, and reaction time
Feelings of greater emotional and physical sensitivity
Anxiety, panic, and paranoia
Physiological effects
Increase in appetite
Increase in heart rate, decrease in blood pressure
Conjunctival injection and suffusion
Dry mouth
Impaired psychomotor coordination and sedation
*The effects peak after 30 minutes and last for two to four hours
Routes of use
Cannabis is often rolled in a cigarette paper and smoked with tobacco in a “joint” or “spliff,” and it produces inhaled carcinogens. Most carcinogens in tobacco are present in cannabis. Typical cannabis use results in a larger volume of smoke being inhaled than with ordinary tobacco products and a fivefold increase in concentrations of carboxyhaemaglobin.7 Tetrahydrocannabinol is fat soluble and is absorbed from the gastrointestinal tract. Although oral ingestion of cannabis avoids the risks associated with smoking, secondary active metabolites are formed and dose titration is difficult.w3 Oral use may lead to intense, unpredictable prolonged intoxication.w4
Harms and risks associated with the use of cannabis
Table 1 (table 1⇓) outlines the harms and risks associated with cannabis use, such as acute and chronic effects and possible risks in specific populations.
Harms and risks associated with cannabis use. Adapted from the 2009 guidelines from Australia’s National Cannabis Prevention and Information Centrew7 and from Hall and Degenhardt3
Associations with use at young age
Large population based longitudinal studies have shown that the earlier the age of first use of cannabis, the greater the risk of dependence, other problems of substance misuse, mental health problems, and poor emotional, academic, and social development.3 w5 Vulnerability to the reinforcing positive effects of cannabis use and to dependence, has a heritable component.w6
Pulmonary harms
Cannabis smoking shows a dose-response relation with pulmonary risk in the same way that tobacco smoking does. A longitudinal study of young cannabis smokers showed that regular heavy use can produce chronic inflammatory changes in the respiratory tract, resulting in increased symptoms of chronic bronchitis such as coughing, shortness of breath, production of sputum, and wheezing.8 A study comparing results of pulmonary function tests and computed tomography scans across different smoking groups estimated that one cannabis joint caused the equivalent airflow obstruction associated with smoking two and a half to five cigarettes.9 A recent cross sectional study examining an older population of smokers suggests that concurrent smoking of cannabis and tobacco leads to synergistic respiratory harm, whereas smoking cannabis alone probably does not lead to chronic obstructive pulmonary disease.10 However, a large case-control study from New Zealand does suggest that cannabis smoking is an independent risk factor for lung malignancy; heavy smokers (more than 10 years of smoking cannabis joints) had a relative risk of 5.7 after adjustment for age, tobacco use, and family history of lung cancer.11 A large prospective study found that cannabis use may be a risk for coronary events, especially in those with pre-existing cardiovascular disease.w8
Mental health and cognition
Observational evidence associates cannabis use and psychotic disorders, but causality is not established.w9 Cannabis use is associated with double the risk of schizophrenia (from 0.7 in 1000 to 1.4 in 1000), and some evidence exists that starting use under the age of 16 years increases the risk.12 A cross sectional study showed that a family history of psychotic illness and a personal history of unusual experiences raised the risk of psychotic illness associated with cannabis use.13 A recent review highlighted consistent evidence that onset of schizophrenia presents earlier (by 1.9-6.7 years) in male cannabis smokers.14 A recent systematic review found that cannabis use was associated with increased relapse and non-adherence to medication in patients with schizophrenia.15
Cross sectional and cohort studies have found higher levels of depressive symptoms in cannabis users than in non-users.w10 However, a systematic review concluded that cannabis use does not cause affective disorders.12 Rates of cannabis use are higher in those with anxiety disorders than in those without, and heavy users of cannabis have higher levels of anxiety, but the nature of this relation is not clear.16
Differentiating between chronic cannabis intoxication and psychiatric disorders
The presenting symptoms of chronic cannabis use and intoxication can sometimes be confused with those of depression (lethargy, sleep and appetite disturbance, social withdrawal, problems at work or at home, cognitive impairment). Symptoms may improve or resolve outside periods of intoxication or withdrawal. Psychiatric disorders that are unrelated to cannabis use may have been present before the onset of use and their symptoms are likely to persist with abstinence from cannabis. If symptoms resolve when cannabis use ceases, the likelihood of a primary psychiatric diagnosis diminishes. In a small inpatient withdrawal study of 20 heavy users of cannabis, mean baseline depression symptom scores reduced to normal levels after four weeks of abstinence.17 The diagnosis of a depressive disorder and start of antidepressants should therefore usually be deferred until after a period or two to four weeks of abstinence. Resolution of affective symptoms after cessation may act as a good motivator for maintaining abstinence (fig 1⇓).

Fig 1 Decision pathway for assessing affective symptoms in cannabis users
{kind=link}
Recent imaging studies have identified reductions in the volumes of the amygdala and hippocampus that are related to cannabis use,18 consistent with studies that have identified duration of use and dose related impairments in memory and attention in long term heavy users of cannabis.19
Identifying the cannabis user for whom use is a problem
Although problems of cannabis use can arise at any level of use, however low, cannabis use disorders and other problems are more likely to arise in long term, heavy daily users than in casual, infrequent users. Screening questions about cannabis use and other substance use can accompany other lifestyle questions about tobacco and alcohol use and can be raised during consultations on smoking, mental health, and sleep disturbances (fig 2⇓). Some patients may try to avoid such questions or they may ask subtle questions to check that drug use is OK to talk about. Others will be relieved to be asked. Questions should focus on frequency of use and amount used. If a patient’s cannabis use is not impairing any aspect of psychosocial functioning, and he or she seems to control the use and recognise the risks and when use might be considered a problem, then the intervention can be restricted to giving health information and discussing risks.
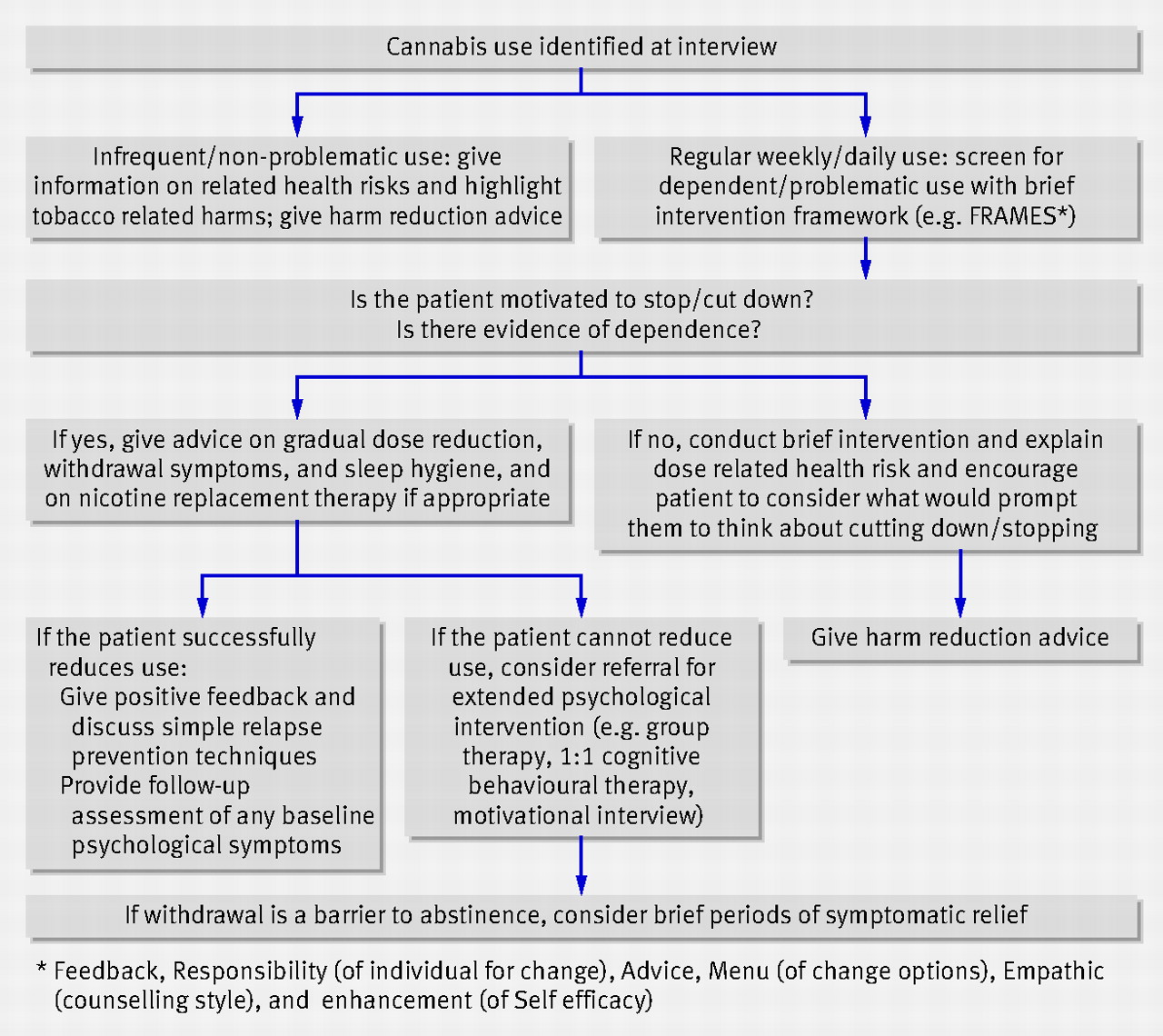
Fig 2 Identifying and responding to cannabis use disorders
{kind=link}
Box 3 lists questions that may be useful in quantifying the level of use and confirming the presence of a cannabis use disorder. Both ICD-10 (the international classification of diseases, 10th revision) and the DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision) recognise cannabis as a substance that causes dependence. About 1 in 10 users develops dependence.20 Dependence is defined by a cluster of symptoms, including loss of control, inability to cut down or stop, preoccupation with use, neglecting activities unrelated to use, continued use despite experiencing problems related to use, and the development of tolerance and withdrawal (which results from the body requiring (but not receiving) more of the drug to achieve the same effect).
Box 3 Questions to ask cannabis users to identify problems, including withdrawal
How long does a gram (or an eighth of an ounce (3.5 g)) last you? How many joints a day do you smoke? How many joints do you make from a gram?
On how many days a week or month do you smoke?
Do you mix it with tobacco? Do you smoke cigarettes as well?
Does your cannabis use cause you any problems, such as anxiety, cough, interference with your sleep or appetite?
Does your smoking ever interfere with what you want to do or what you have to do, such as working or studying?
Have you ever thought about cutting down or stopping?
Have you ever tried to cut down or stop? What happened? Were you able to sleep? Do you get irritable or moody?
If you managed to stop for a while, how did you feel afterwards?
What if assessment suggests problematic use or dependency?
Although some dependent users recognise their use as problematic, others may not, and in such cases a motivational approach may be appropriate: to raise awareness of the consequences of use, explore and resolve ambivalence, and subsequently motivate change.21 Asking the patient to draw up a pros and cons table can be good way to get them to think about their use (table 2⇓). Although abstinence may be an optimal outcome, a reduction in use may be a more attainable initial goal.22
Pros and cons of cannabis use—a decisional matrix
No intervention to date has proved consistently effective for the majority of those with dependence on cannabis. Trials in the United States and Australia support four methods of behavioural based interventions: motivational interviewing, motivational enhancement therapy, cognitive behavioural therapy, and contingency management.
Cognitive behavioural therapy and contingency management have the most evidence for reduction in cannabis use and maintaining abstinence.22 For younger users, family based interventions may be more effective.22 Brief, behaviourally based interventions suitable for delivery by general practitioners may be effective. One randomised study of a brief motivational intervention in young users showed a reduction in cannabis use from 15 days to five days a month, and at three months one in six were abstinent.23 Extended abstinence can be supported through maintaining motivation and the use of relapse prevention techniques.22 A randomised trial that enrolled members of the general public who fulfilled criteria for dependency explored contingency management (money vouchers for continued abstinence) and motivational and cognitive behavioural therapy interventions for maintaining abstinence. Contingency management alone led to the highest rates of initial abstinence in adult cannabis smokers, but longer term abstinence was helped by the use of coping skills and post-treatment self efficacy training.24 A computer based intervention to treat comorbid depression and cannabis dependence tested in a randomised controlled trial seemed to have potential in managing this group.w11
Figure 2⇑ outlines in an algorithm how to identify and respond to cannabis use disorders.
How to manage withdrawal
Symptoms of withdrawal (table 2⇑) may be a barrier to abstinence as they may be of similar intensity to those accompanying tobacco cessation. As many as 85% of users experience withdrawal.20 A cross sectional survey of treatment seekers found that concurrent use of cannabis and tobacco makes it harder to quit either substance25 and withdrawal tends to be more severe in cannabis users who are also heavy users of tobacco and in cannabis users with mental illness. Withdrawal symptoms peak on day 2 or 3, and most are over by day 7. Sleep problems and vivid dreams can continue for two to three weeks.20
No evidence based pharmacological intervention exists for managing cannabis withdrawal.26 Some small studies exploring the utility of oral tetrahydrocannabinol show promise in reducing withdrawal and craving.27 If bupropion is used in nicotine dependence it must begin at least one week before cessation of both substances, as starting treatment on day 1 of cannabis cessation may exacerbate withdrawal symptoms.28 Our experience is that providing a patient with information about withdrawal symptoms may help them to prepare for discomfort, which if severe can be alleviated with a few days of symptomatic relief. Most dependent users, however, probably do not require any drug intervention to manage their withdrawal. Box 4 outlines what advice to give to patients on managing withdrawal.
Box 4 Management of withdrawal
Advise gradual reduction in amount of cannabis used before cessation
Suggest that the patient delays first use of cannabis till later in the day
Suggest that the patient considers use of nicotine replacement therapy if he or she plans to stop separate tobacco use at the same time
Advise the patient on good sleep hygiene, including avoidance of caffeine, which may exacerbate irritability, restlessness, and insomnia
Suggest relaxation, progressive muscular relaxation, distraction
Suggest psychoeducation sessions for the user and family members on the nature, duration, and severity of withdrawal, to help with a better understanding of dependence and reduce likelihood of relapse
Advise the patient to avoid the cues and triggers associated with cannabis use
Prescribe short term analgesia and sedation for withdrawal symptoms if required
If irritability and restlessness are marked, consider prescribing very low dose diazepam for three to four days
Cessation of use can be monitored with urine tests over several weeks for the inactive metabolite of cannabis (carboxy-tetrahydrocannabinol); heavy smokers may continue to be positive for cannabis for up to six weeks.w12
Harm minimisation for those who choose to continue using cannabis
Initial assessment and feedback could focus on the pulmonary harms of smoking, citing strategies that target both tobacco and cannabis (for example, Health Scotland’s publication Fags ‘n’ Hash29).
Water pipes (also known as bongs), which cool and filter smoke, are not a safer way of smoking. They filter out more tetrahydrocannabinol than they do tar, resulting in greater tar delivery to the lungs.w13 The role of vaporisers (which heat the plant material, releasing the tetrahydrocannabinol as a vapour but avoiding combustion) as an effective harm reduction intervention is uncertain.w13- w15 Box 5 outlines advice for patients on how they can reduce their risk of harm from cannabis use.
Box 5 Advice for patients on reducing their risk of harm from cannabis*
Do not mix cannabis with tobacco
Avoid daily and binge use
Do not use a cigarette filter—this will reduce the ratio of cannabis to tar (30% less cannabis, 60% more tar)
Do not hold smoke in your lungs—this will not get you more stoned but will increase tar and carcinogens coming into contact with your lungs
Do not inhale too deeply—most tetrahydrocannabinol is absorbed from the upper airways
Do not mix cannabis with alcohol and/or other drugs such as cocaine
Remove stalks and leaves
Do not use too many papers
Avoid using a bong (water pipe)—pulling on a bong or using a bucket may cool smoke but will also force smoke deeper into your lungs and may filter out more tetrahydrocannabinol than tar
Avoid plastic bottles/pipes/aluminium foil as these can increase toxic fumes
If you do use pipes and/or bongs clean them thoroughly
Avoid cannabis use if you have a history of serious mental illness
Do not drive while intoxicated especially if you have consumed alcohol as well as cannabis
*Adapted from 1999-2005 HIT UKw16
When to refer to a specialist
Persistent use despite recognition of harms and unsuccessful attempts to reduce use should lead to specialist referral; consider specialist referral also for those with severe comorbid mental health problems and those who are pregnant.
Ongoing research
A multicentre European trial is examining risk and protective factors and multidimensional family therapy for adolescents
US trials are investigating effective interventions to manage withdrawal and to support abstinence in otherwise healthy populations, including the use of computerised treatments, contingency management with adolescents, and cannabis patches
The UK MIDAS trial is examining whether an integrated intervention that combines motivational interviewing and cognitive behavioural therapy can effectively reduce use in those with severe mental illness
Unanswered questions
What is the precise nature of the association between cannabis use and development of schizophrenia?
How do higher potency strains of cannabis affect the physical and psychological risks of individuals and the population as a whole?
What is the degree of recovery in cognitive functioning with prolonged abstinence?
What is the neurobiological mechanism underlying cannabis withdrawal?
Tips for non-specialists
Most cannabis users will not develop dependence or severe mental health problems. Concerns should be highest for daily smokers, adolescents, those who are pregnant, and those with coexisting severe mental illness
A gradual reduction in tolerance and levels of use among daily smokers can be helped by getting users to delay the time of first use in the day and to engage in other daytime activities
The insomnia, irritability, and craving that can occur for a few days on cessation of cannabis can be a barrier to attaining abstinence. Cessation is less likely to result in serious withdrawal symptoms if use has fallen to lower levels before quit attempts
If users are reluctant to accept the possibility of a causal relation between cannabis use and an adverse psychological experience or state, encouraging a period of abstinence and self monitoring using a diary and feedback from trusted friends or family members can be useful
Consider discussing concurrent tobacco dependence with patients even if they only use tobacco when they use cannabis
Additional educational resources
Know Cannabis (www.knowcannabis.org.uk)—Self help website
Talk to Frank (www.talktofrank.com/section.aspx?ID=110)—Self help website, with helpline (phone/online)
Young Minds (youngminds.org.uk)—Self help website focusing on young people’s mental wellbeing
Marijuana Anonymous (www.marijuana-anonymous.org)—Online support group for users wishing to quit
Connexions (www.connexions.gov.uk)—Website for young people aged 13-19 years that offers support and links them with a practitioner or personal adviser
Helpfinder, DrugScope (www.drugscope.org.uk/resources/databases/helpfinder.htm)—DrugScope’s database of drug treatment services
Notes
Cite this as: BMJ 2010;340:c1571
Footnotes
Contributors: ARW conceived the review, wrote the initial draft, prepared the final draft, and is the guarantor; CF helped with conception of the review and wrote the screening and assessment sections; JW helped with the literature search and the preparation of the final draft for submission.
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare (1) no support from any company for the submitted work; (2) no relationships with any companies that might have an interest in the submitted work in the previous 3 years; (3) their spouses, partners, or children have no financial relationships that may be relevant to the submitted work; and (4) no non-financial interests that may be relevant to the submitted work.
Provenance and peer review: Not commissioned; externally peer reviewed.