Article Text

Abstract
Objectives To assess death rates among patients waiting for cardiac valve surgery or isolated coronary artery bypass surgery (CABG), and to determine independent risk factors for death while waiting for isolated CABG.
Design Prospective cohort analysis based on an inclusive registry.
Setting Nine cardiac surgical units in Ontario, Canada.
Patients 29 293 consecutive patients scheduled for cardiac surgery between October 1991 and June 1995.
Main outcome measures Death rates while waiting for surgery were determined among patients scheduled for isolated CABG, isolated valve surgery, or combined procedures. Predictors of death among patients with isolated CABG were determined from multivariate analysis.
Results There were 141 deaths (0.48%) among 29 293 patients. Adjusting for age, sex, and waiting time, patients waiting for valve surgery had a significantly increased risk of death compared with patients waiting for CABG alone (adjusted odds ratio 1.88, 95% confidence interval (CI) 1.23 to 2.88, p = 0.004). Results were similar for patients waiting for combined valve and CABG procedures compared with those who were waiting for isolated CABG. Independent risk factors for death while waiting for isolated CABG included: impaired left ventricular function (odds ratio 2.47, 95% CI 1.59 to 3.84, p < 0.001); advancing age (for each decade, odds ratio 1.41, 95% CI 1.10 to 1.80, p = 0.007); male sex (odds ratio 1.95, 95% CI 1.00 to 3.81, p = 0.05); and waiting longer than the maximum time recommended in Canadian guidelines for a patient’s clinical profile (odds ratio 1.59, 95% CI 1.01 to 2.51, p = 0.044). After scaling waiting time to surgery or death continuously in days, the same predictors emerged.
Conclusions Patients waiting for valve surgery have a higher risk of death than patients waiting for isolated CABG. Guidelines to promote safer and fairer queuing for non-CABG cardiac surgery are needed. Shorter waiting lists, better compliance with existing guidelines, and guideline revisions to upgrade patients with left ventricular dysfunction could generate additional reductions in the already low risk of death for patients waiting for isolated CABG.
- cardiac surgery
- waiting lists
- rationing
Statistics from Altmetric.com
Waiting lists for hospital services may promote optimal use of scarce medical resources, but queuing obviously imposes a burden on patients waiting for life enhancing or prolonging services.1 ,2 Lengthy waiting lists for cardiac surgery may lead to some potentially avoidable deaths.3-6
In Ontario, Canada (1996 population, 11.5 million) patients scheduled for cardiac surgery in the province’s nine cardiac surgical centres are entered in a registry containing demographic and clinical data, which enables patients to be followed while on the waiting list. We have previously reported the experience of a one site pilot project for this initiative4 and the results for the first two years for patients waiting for isolated coronary artery bypass graft surgery (CABG) in the full multicentre registry.3 Isolated CABG accounts for about 75% of adult cardiac surgery, and mortality while waiting for cardiac valve surgery has never been addressed.
The number of events in our initial report3 were too few to determine independent predictors for death while waiting for isolated CABG. Our univariate analysis, together with univariate analysis of a small Swedish cohort,5 and a case-control study reported by Suttorp et al,6 indicate that potential risk factors for death while waiting for isolated CABG are left ventricular dysfunction, severe symptoms, left main or extensive multivessel coronary artery disease, diabetes mellitus, advancing age, and high risk non-invasive test results. The same predictors can also be inferred from analyses of randomised trials comparing early CABG to medical treatment with variable crossover to CABG for symptomatic deterioration—that is, similar to the waiting list experience; patients with these characteristics do worse with medical treatment.7 ,8 Data from a large prospective cohort study with multivariate analysis are required to confirm whether these factors confer an independent risk for death while waiting for surgery.
The main purposes of this study were to assess death rates among patients waiting for cardiac valve surgery and isolated CABG, and to determine independent risk factors for death while waiting for isolated CABG.
Methods
Details of data collection and validation have been reported.3 Waiting list deaths are audited on an ongoing basis to confirm whether they are cardiac or sudden and therefore presumed cardiac. Waiting time is defined as starting at the time that the patient is accepted for surgery by the cardiac surgeon. A previously published urgency rating score (URS) is calculated for all patients undergoing isolated CABG.9 Currently, symptom severity accounts for about 60% of the score, anatomy 25%, non-invasive test results 15%, and left ventricular function less than 10% of the variation in scores. The URS is used as a guideline for maximum recommended waiting times for surgery, and there is good compliance in our province—that is, patients with a higher mortality risk while waiting for surgery have appropriately shorter waiting times.3 Lack of significance for particular clinical factors does not mean that they are not risk factors for death while waiting for surgery, but rather that the queuing process has successfully upgraded patients with those factors and thereby limited their impact.
In contrast, practitioners retain latitude to enter patients individually to the waiting list, and the timing of surgery for otherwise similar patients varies among practitioners and centres. Furthermore, as caseloads ebb and flow, waiting list lengths are affected by the extent of supply and demand mismatch. Hence, even if practitioners have successfully mitigated the impact of specific clinical factors by matching waiting times to patient characteristics and risks of death while waiting for surgery, waiting time itself may be a risk factor.
STATISTICAL ANALYSIS
Primary comparisons were between patients who survived to surgery and those who died while on the waiting list. We excluded patients who were registered twice because they underwent surgery at a centre different from the original booking hospital, as well as four patients who had surgery indefinitely deferred after suffering a myocardial infarction while waiting for surgery.
Continuous variables are expressed as median with 25th to 75th centile or interquartile ranges. A logistic regression model was developed to determine the influence of cardiac valve surgery on waiting list mortality relative to that of isolated CABG. Factors included were sex, age scaled in 10 year increments, and waiting time in days.
A multiple logistic regression model for patients undergoing isolated CABG included the following variables: severe angina, modified Canadian Cardiovascular Society classes IVB or IVC9; left main coronary stenosis, measured as 50% luminal diameter reduction by standard visual/caliper assessment; multivessel coronary artery disease, either two vessels affected, with proximal left anterior descending artery involvement, or three vessels affected, with more than 70% luminal diameter reduction; impaired left ventricular function, graded III or IV by qualitative assessment of either echocardiograms or nuclear ventriculograms, or estimated ejection fractions of less than 35–40% in contrast ventriculograms at catheterisation; age scaled in 10 year increments; sex; and excess waiting time defined in relation to surgery or death as whether the patient waited longer than the maximum waiting time recommended for an individual with that clinical profile and corresponding URS. Complete data on the presence or absence of diabetes mellitus were not available.
The seven variables were entered and backward stepwise logistic regression undertaken with a threshold to exclude of 0.40. All remaining variables were examined for independent effects. The following changes to the model were examined in sensitivity analyses: severe angina scaled as classes III-IV in general, based on evidence from the chronic stable angina trialists’ overview that this broader group may be at higher risk7; grade IV ventricular function analysed separately, rather than combined with grade III; left main and multivessel disease combined as a single anatomical jeopardy variable, rather than as separate factors; and leaving time or age and sex out of the model.
We also included time effects in this multivariate model in two alternative ways: as absolute waiting time in days to death or surgery, or waiting time as a percentage over or under the maximum recommended for an individual with that URS. Because waiting times do not follow a normal distribution, these latter analyses were repeated after log transformation.
All analyses were performed using STATA version 4.0 (STATA Corporation, College Station, Texas, USA).
Results
Between October 1991 and June 1995, 30 849 registered patients underwent cardiac surgery or died while waiting. The planned procedures were: isolated CABG 22 655 (73.4%), isolated valve surgery 4600 (14.9%), combined CABG and valve surgery 2038 (6.6%), and other operations—for example, repair of congenital heart disease and pericardial surgery, 1556 (5.1%). The last were excluded (four deaths), leaving 29 293 patients for analysis.
DEATHS WHILE WAITING FOR SURGERY
Among patients scheduled for valve surgery or CABG, or both, 141 (0.48%) died while waiting for surgery. Table 1 shows death rates according to the planned surgical procedure. The observed differences in waiting list mortality among patients undergoing isolated CABG (0.40%), isolated valve surgery (0.65%), and combined CABG and valve surgery (0.98%) were significant (p = 0.001).
Numbers of patients, deaths, demographic characteristics, and median waiting times for patients waiting for isolated CABG, isolated cardiac valve surgery, or combined procedures
Logistic modelling confirmed that valve surgery, either alone or in combination with CABG, was associated with a significantly increased risk of death while waiting compared with that for CABG alone (table2). For example, the crude odds ratio for isolated valve surgery compared with that for isolated CABG was 1.63 (95% confidence interval (CI) 1.08 to 2.46, p = 0.021). After adjusting for age, sex, and waiting time, the odds ratio rose to 1.88 (95% CI 1.23 to 2.88, p = 0.004). Findings were similar for patients who had CABG and valve surgery compared with those who underwent isolated CABG (table 2).
Mortality rates for patients waiting for isolated CABG, isolated cardiac valve surgery, or combined procedures
We also compared patients waiting for combined valve and CABG procedures to those undergoing isolated valve surgery, but the small number of deaths meant that the results were inconclusive. There was a trend to higher death rates with combined procedures (crude odds ratio 1.51, 95% CI 0.86 to 2.66, p = 0.155), but this was diminished after adjustment for age, sex, and waiting time (adjusted odds ratio 1.20, 95% CI 0.66 to 2.17).
DEATHS WHILE WAITING FOR ISOLATED CABG
Patient characteristics and waiting times
Table 3 shows the characteristics of patients waiting for isolated CABG. Figure 1 shows the waiting time distribution among patients (99.6%) who survived to surgery.
Characteristics of patients requiring isolated isolated CABG (n = 22 655)

Distribution of waiting times for isolated coronary artery bypass graft surgery (CABG) (to completion) in Ontario, Canada for more than 22 000 patients between October 1991 and June 1995.
Independent risk factors
Impaired left ventricular function and increasing age were highly significant factors, independently associated with waiting list death (table 4). Male sex was a significant risk factor, with an odds ratio of 1.95, roughly equivalent to a 20 year age differential. The point estimates for both left main and multivessel coronary artery disease were suggestive of an independent increase in death rates (both odds ratios are about 3.8), but neither factor reached nominal significance, probably because numbers in the comparison group were small (only 6.28% of patients had limited vessel disease).
Factors potentially associated with death among 22 655 consecutive patients waiting for isolated CABG
Sensitivity analyses show that the estimated impact of the remaining factors were little changed when waiting times or age and sex were eliminated from the model. Results were statistically similar when multivessel and left mainstem disease were combined: 0.07% (95% CI 0.002 to 0.40) of patients with limited anatomical disease died compared with 0.40% (95% CI 0.32 to 0.49) of those with more extensive coronary stenoses. Severe angina remained non-significant as a risk factor despite broadening the definition to include patients with class IVA and III. Redefining impaired left ventricular function as grade IV only, the factor remained significant and the odds ratio rose to 4.05 (95% CI 2.30 to 7.12), as expected given the greater severity of the subgroup.
Time effects
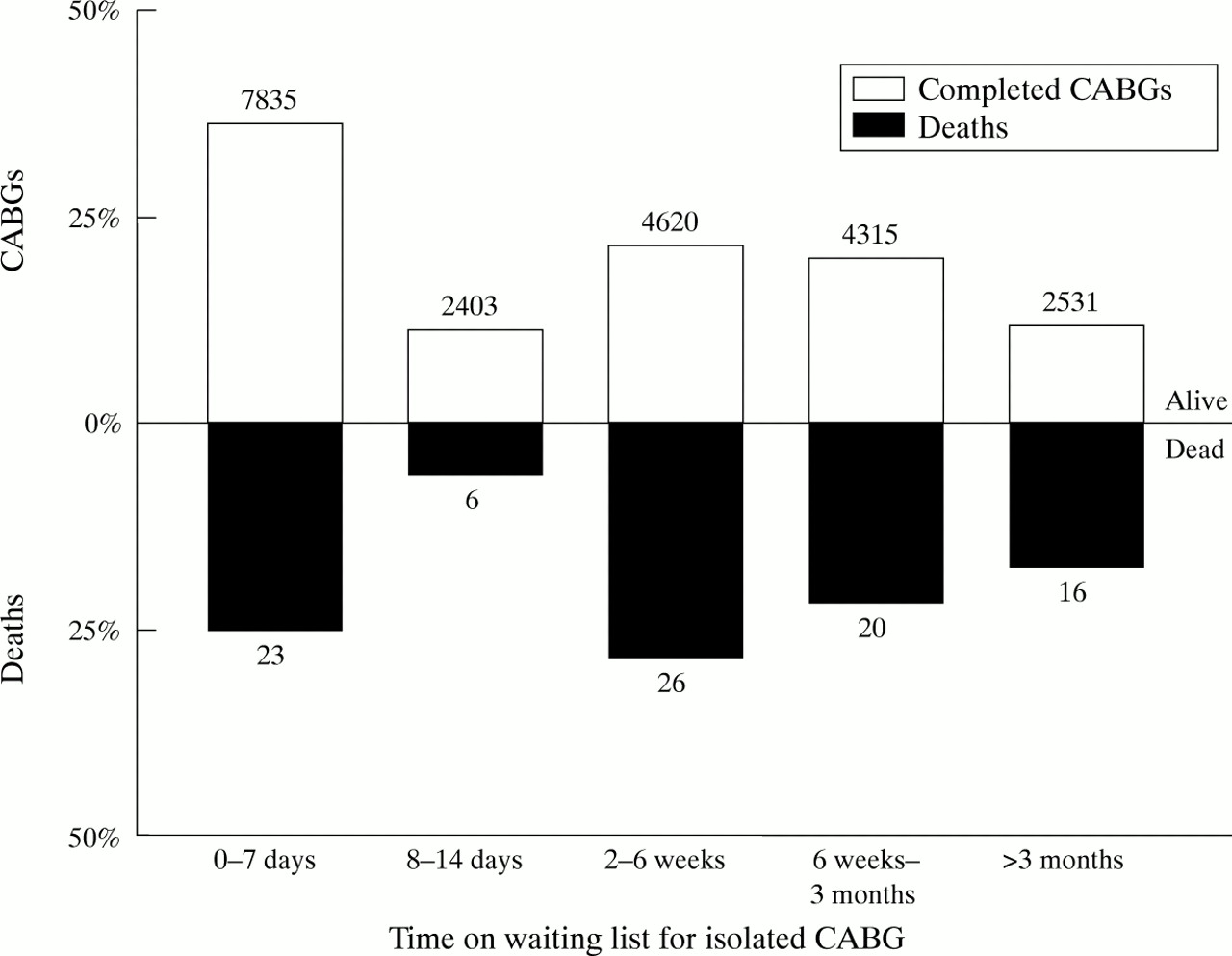
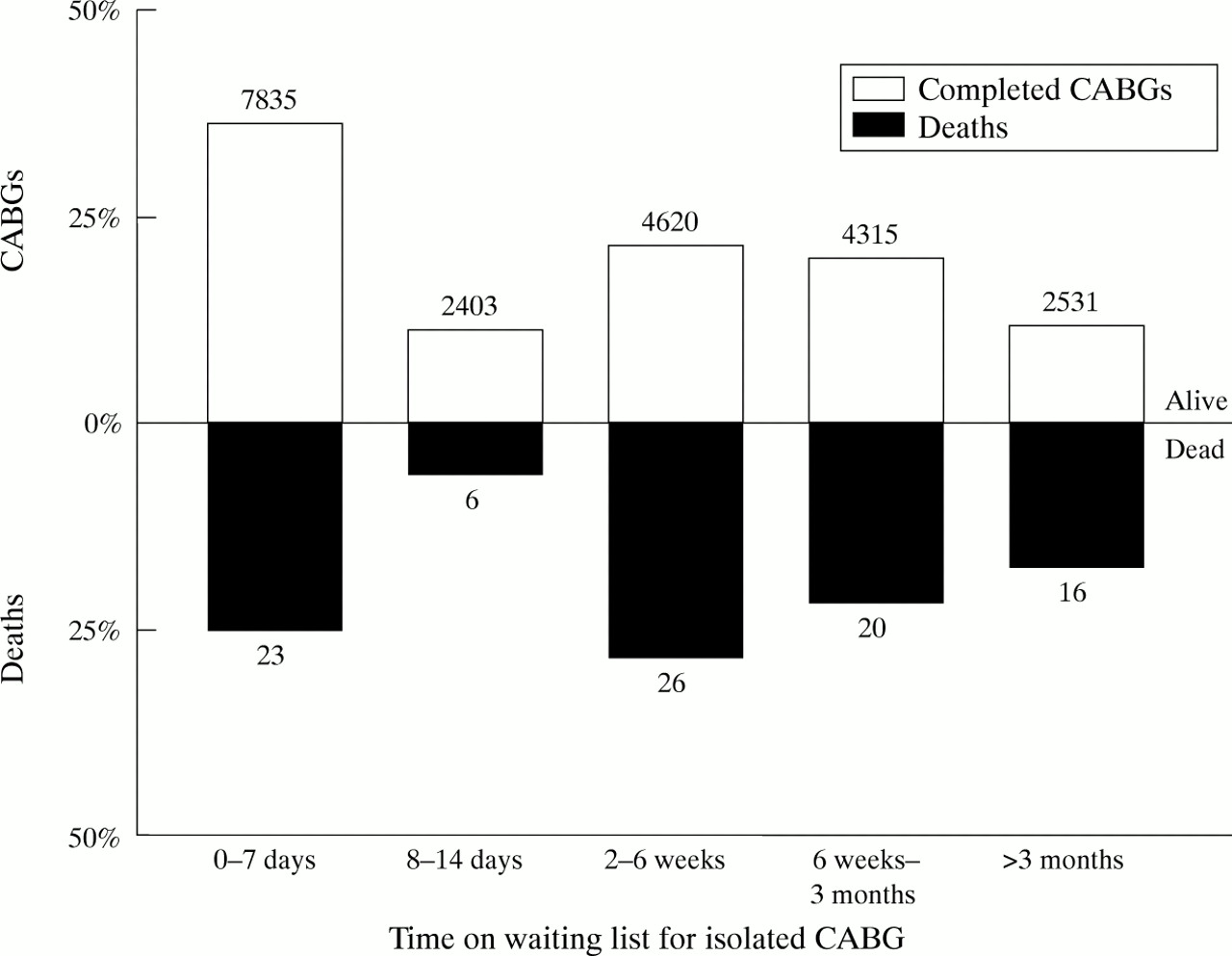
A histogram (fig 2) of time to surgery or death highlights the variability in time to death across typical urgency categories, with one third of deaths occurring within 14 days of joining the waiting list and others occurring randomly. Among patients surviving to surgery, 25.3% underwent surgery outside the maximum waiting time recommended for their risk profile (“overdue”), compared with 34.1% who were overdue and died while waiting for surgery. Multivariate analysis showed that overdue status was borderline significant (odds ratio 1.59, p = 0.044) (table2).
{kind=link}
{kind=link}
Distribution of waiting times and deaths while waiting for isolated coronary artery bypass graft surgery (CABG) by typical urgency categories used in Ontario9: surgery scheduled for one to two weeks after joining the waiting list is deemed to be “urgent” or “semi-urgent”; patients scheduled for operation at two to six weeks are considered to be on the “short list”; procedures scheduled for six weeks to three months are considered to be “elective”; and those of more than three months are low priority.
This relation was not found on scaling time as a percentage above or below the recommended maximum waiting time according to the URS (odds ratio 1.00, 95% CI 1.00 to 1.00, p = 0.984 for untransformed data; odds ratio 1.20, 95% CI 0.94 to 1.33, p = 0.202 after log transformation). When time to surgery or death was scaled simply as the number of days waiting for surgery, waiting time re-emerged as an independent risk factor for death (odds ratio 1.003, 95% CI 1.000 to 1.006, p = 0.03 for untransformed data; odds ratio 1.13, 95% CI 0.99 to 1.30, p = 0.074 after log transformation). Weights for the other risk factors remained similar regardless of how time was scaled.
Discussion
This study draws on a cardiac surgery waiting list registry in a universal health care system unique in its population based scope, size, and consistent capture of consecutive cases. While most attention to waiting lists has focused on coronary artery bypass grafting, we have shown that waiting for cardiac valve surgery is associated with a significantly higher risk of death than waiting for isolated coronary surgery. Most patients who died were waiting for surgery for aortic stenosis; however, the numbers remain far too small and clinical details too limited to allow a more conclusive assessment of the risk associated with different valve lesions. This is the subject of ongoing research. In the interim, these findings have led us to convene a delphi panel to develop queuing criteria for valve surgery, similar to those already developed for isolated CABG.9 Because of the lack of randomised trials comparing medical and surgical treatments for valve disease, pathophysiological inferences are necessary to select patients with primary valve lesions according to their risks from delayed surgery—for example, all things being equal, an individual with “tight” aortic stenosis and congestive heart failure or syncope, is assumed to be at a higher risk of death while waiting for surgery than one with a modest gradient and no symptoms.
The death rate for isolated coronary artery surgery was 0.40% or about one in 250. For comparison, one Swedish study reported a death rate of 2.1% among 718 patients waiting for either CABG or percutaneous transluminal coronary angioplasty.5 A later study10 reported eight deaths among 1039 patients waiting for CABG at seven Swedish centres, and 11 deaths among 1061 patients waiting for elective CABG at 10 centres in the Netherlands (a waiting list death rate of about 1% in both jurisdictions). Although deaths while waiting for surgery are a cause for concern, the low death rate in Ontario suggests that clinicians are generally making sound decisions in prioritising patients.
The large sample size allowed us to carry out the first multivariate analysis based on a prospective cohort study to confirm or refute some predictors suggested by earlier univariate analyses and a retrospective case-control study. Our findings confirm that impaired left ventricular function is a strong and independent risk factor for death while waiting for surgery. This conclusion is consistent with experience in randomised trials of medical versus surgical treatment for chronic stable angina, if patients in the medical arms of these trials are considered to be analogous to patients waiting for surgery. Pooling 10 year follow up data across these arms, Yusuf and colleagues7 found that mortality in medically treated patients was 13.3% in those with normal left ventricular function versus 25.2% in those with impaired left ventricular function. In future, patients with impaired left ventricular function should receive higher priority and have shortened waiting times, particularly those with grade IV ventricles.
The significant impact of age and borderline significant impact of sex are more difficult to address. In comparison with younger individuals, the elderly have dramatically higher mortality for various ischaemic syndromes, including acute myocardial infarction,11-13and this is the logical mechanism for their higher death rate while waiting for surgery. Surveys of Ontario physicians suggest that their preference would be to give higher priority to younger persons,14 but in actual practice advancing age does not appear to be an independent determinant of longer waiting times.3 Ethically guided debate is needed about how to balance the higher death rates for elderly patients waiting for CABG, and the greater number of life years lost when younger patients die while waiting for surgery.
We are unable to account for the increased risk among men. This finding may be an artefact arising from incomplete characterisation of our patients—for example, if men smoke more frequently while waiting than women, this could contribute to their higher risk. Further research is underway to determine the potential reasons for this result.
As for waiting times themselves, we confirmed that patients were at higher risk of death if they waited longer than recommended under the Ontario URS.9 These effects were small (0.59% mortality for those “over time” versus 0.35% for those “on time” or “early”), however, and not confirmed when the patient’s waiting time was scaled as a percentage over or under his recommended maximum wait. Indeed, about two thirds of deaths (60 of 91) occurred among patients who were not unduly delayed by our criteria.
It is not surprising that cumulative time alone appears to confer a small but independent risk for death. This is tantamount to a follow up effect—that is, if there are two groups of patients at similar baseline risk for coronary events, and one group is followed for longer than the other, then the group with longer follow up would be expected to have more adverse events. Such an effect would be expected to persist even if waiting list management was improved to eliminate the impact of discretely identifiable risk factors such as left ventricular dysfunction. Furthermore, although the impact of waiting for surgery on quality of life was not addressed, almost by definition these adverse effects must be cumulative with time. Reduction in waiting times therefore remains desirable, notwithstanding the relatively small time effects shown here.
In conclusion, by prioritising patients on the basis of clinical factors and related risk, Ontario practitioners have limited the vital toll of cardiac surgery waiting lists. Small additional reductions in mortality may be achieved by better queuing of valve patients, keeping waiting times for CABG inside the recommended boundaries, and upgrading the weight given to left ventricular dysfunction as a risk factor. All things being equal, longer waits are associated with modest increases in the risk of death, and most deaths while waiting for isolated CABG occur among patients who are not overdue by Ontario’s current criteria. Thus, a reduction in target and actual waiting times across all levels of acuity is necessary if the number of deaths is to be cut further.
Acknowledgments
This research was supported in part by grant number MA 13695 from the Medical Research Council of Canada. Professor Naylor is supported by a career scientist award (02377) from the Ontario Ministry of Health and by the Institute for Clinical Evaluative Sciences in Ontario, which is funded by the Ontario Ministry of Health and co-sponsored by the Ontario Medical Association. No official endorsement by the funding or sponsoring agencies is intended or should be inferred. The authors thank the many cardiologists and cardiac surgeons of the Provincial Adult Cardiac Care Network of Ontario, the institutional and regional coordinators responsible for data collection and patient follow up, and staff of the Cardiac Care Network coordinating office at Victoria Campus of the London Health Science Centre, Ontario, particularly Mr Steven Jefferson.
Appendix
Members of the steering committee of the Adult Cardiac Care Network of Ontario: Seewa Aul, Sudbury Memorial Hospital; Donald S Beanlands, University of Ottawa Heart Institute; Lorna Bickerton, University of Ottawa Heart Institute; Robert Chisholm, St Michael’s Hospital, Toronto; Martin Goldbach, Victoria Campus, London Health Science Centre; Joseph Homer, Hamilton Civic Hospitals; Christopher Lai, Thunder Bay Regional Hospital; Jeffrey Lozon, St Michael’s Hospital, Toronto; John Marshall, Kingston General Hospital; Neil Mckenzie, University Campus, London Health Science Centre; Barry J Monaghan, West Park Hospital, Toronto; Christopher D Morgan, Sunnybrook Health Science Centre, Toronto; Hugh Scully, Toronto Hospital; B William Shragge, Hamilton General Hospital; and James Swan, Scarborough Centenary Health Centre (term ended 1996).