Article Text

Abstract
Purpose: Whether central adiposity contributes independently of total adiposity to the risk for gall stones is inconclusive. We examined prospectively indicators of central adiposity in relation to the occurrence of gall stone disease.
Methods: We evaluated the relationship between abdominal circumference and waist to hip ratio and risk of cholecystectomy in a cohort of women who had no history of gall stone disease. As part of the Nurses’ Health Study, the women reported on questionnaires their weights, heights, and waist and hip circumferences, and the occurrence of cholecystectomy. A total of 42 312 women, aged 39–66 years in 1986, who were free of prior gall stone disease, provided complete waist and hip circumference measurements in 1986.
Results: We documented 3197 cases of cholecystectomy during 514 283 person years of follow up. After adjusting simultaneously for regional (waist circumference or waist to hip ratio) and total adiposity (body mass index) measures as well as for other risk factors of gall stone disease, women with a height adjusted waist circumference of 36 inches or larger had a relative risk (RR) of 1.96 (95% confidence interval (CI) 1.53–2.51; p trend <0.0001) compared with women with a height adjusted waist circumference of less than 26 inches. Waist to hip ratio was directly associated with the risk, with an RR of 1.39 (95% CI 1.16–1.66; p trend <0.0001) for women with a waist to hip ratio of 0.86 or higher compared with women with a waist to hip ratio of less than 0.70.
Conclusion: Abdominal circumference and waist to hip ratio were associated with an increased risk of cholecystectomy, independently of body mass index in women.
- HDL, high density lipoprotein
- BMI, body mass index
- central obesity
- gall bladder
- cholecystectomy
- gall stone
- women
Statistics from Altmetric.com
Gall stones are a major source of morbidity in the USA, and result in more than 800 000 cholecystectomies each year.1 In developed countries, gall stone disease is the most common abdominal morbidity for which patients are admitted to hospitals.2,3 In most Western populations, an estimated 80% of gall stones are cholesterol stones.4 Many factors have been associated with the risk of cholesterol gall stones, but hypersecretion of cholesterol into the biliary tree is an important determinant of gall stone formation.4 Low plasma high density lipoprotein (HDL) cholesterol and hyperinsulinaemia were shown to be associated with greater risk of gall stone disease.4,5 Central or abdominal obesity, which is a powerful contributor to metabolic abnormalities such as insulin resistance, hyperinsulinaemia, reduced number of insulin receptors, and low plasma HDL cholesterol,6–8 may play an important role in gall stone formation.9,10 The studies available on the relationship between regional fat distribution and gall stones are controversial.11–14 These studies were limited by short follow up periods, incomplete control of confounding, or a small number of end points. Moreover, whether regional obesity represents an independent risk factor for gall stone disease after taking total adiposity into account is still not well defined. Thus we examined prospectively indicators of central obesity in relation to the risk for cholecystectomy in a large cohort of women in the USA.
METHODS
Study population
In the Nurses’ Health Study, 121 700 female registered nurses, predominantly Caucasian, aged 30–55 years, completed a mailed questionnaire on their medical history and lifestyle characteristics in 1976. Every two years, follow up questionnaires were sent to update information on potential risk factors and to identify newly diagnosed illnesses. This analysis is based on the follow up of 42 312 women who provided complete waist and hip circumference measurements in 1986, who answered the 1986 diet questionnaire, and who did not have a cholecystectomy, a gall stone diagnosis, or a diagnosed cancer before 1986. The study was approved by the institutional review board on the use of human subjects in research of the Brigham and Women’s Hospital in Boston.
Identification of cases of cholecystectomy
We inquired about the occurrence and date of cholecystectomy on each biennial questionnaire. A validation study of the self report was conducted in a random sample of 50 nurses who reported cholecystectomy. Forty three of 50 participants responded, and of these, all reiterated their earlier report, and surgery was confirmed in all 36 for whom medical records could be obtained. Cholecystectomy was used as an end point mainly because gall stone disease is mostly treated surgically15 and because women are more likely to accurately report the occurrence and timing of a surgical procedure rather than untreated gall stones. In addition, symptomatic gall stones are the main indication for cholecystectomy. In contrast, only a minor proportion of asymptomatic gall stones are diagnosed, typically incidentally, making this clinically less relevant condition an unreliable end point.
Anthropometric assessment
In 1986, participants were instructed to measure their waist at the level of the umbilicus and their hips at the largest circumference with a tape measure while standing relaxed and to report values to the nearest quarter inch. Waist to hip ratio and waist circumference were used to measure the relative distribution of fat. Because waist circumference tends to be correlated with height, we adjusted waist for height by using residual analysis to remove extraneous variation related to height. We first regressed waist on height using linear regression and then added the individual’s residual to the average waist for a woman of average height to convert this measure back to the initial scale. We used body mass index (BMI), which was calculated by dividing weight (in kilograms) by the square of height (in metres), as a measure of total adiposity. BMI is correlated with absolute fat mass, as determined by hydrostatic underwater weighing (r = 0.84–0.92).16
In 1987, the validity of self reported waist and hip measures was assessed in a random sample of 140 participants living in the greater Boston, Massachusetts area.17 The average of two technician measurements spaced six months apart was compared with the self reported current weight and waist and hip circumference values on the most recent questionnaire. Women reliably reported waist circumferences but slightly underestimated hip circumference by an average of 1.4 cm (0.54 inches). Reported waist-hip ratio was thus slightly higher than that obtained from directly measured values. Crude Pearson correlation coefficients for reported and measured circumferences for waist and hip and the waist-hip ratio were 0.89, 0.84, and 0.70, respectively. After adjusting for age, the Pearson correlation between self report and the average of the technicians’ two measurements was 0.89 for waist circumference, 0.84 for hip circumference, and 0.68 for waist to hip ratio. The Spearman correlation between self reported and measured weight was 0.96. The mean self reported weight was 1.5 kg lower than directly measured weight, compatible with the difference between a casual weight with light clothing and a morning postvoid nude weight.
Data analysis
We calculated person time of follow up for each participant from the date of return of the 1986 questionnaire to the date of cholecystectomy, diagnosis of cancer, date of last questionnaire return, death, or the end of the study period in 2000, whichever came first. We computed incidence rates of cholecystectomy by dividing the number of events by person years of follow up in each category of waist circumference and waist to hip ratio. The relative risk was calculated as the incidence rate in a specific category of waist circumference and waist to hip ratio divided by that in the lowest category of each index, with adjustment for age in one year categories.
Multivariable relative risks were computed using the Cox proportional hazards regression model.18 In multivariable analyses, we simultaneously adjusted for the following known or suspected confounding variables: time period, age, physical activity, parity, oral contraceptive use, postmenopausal hormone use, pack years of smoking, thiazide diuretics, non-steroidal anti-inflammatory drugs, total energy intake, intakes of energy adjusted dietary fibre, carbohydrates, polyunsaturated fat, monounsaturated fat, saturated fat, and trans fat, alcohol, and coffee. While reported diabetes mellitus was associated with obesity and gall stone disease, we did not control for it in the multivariable models, as adjusting for risk factors in the causal pathway would inappropriately attenuate the true relative risk of obesity.19 Tests of linear trend across increasing categories of anthropometric measurements were conducted by assigning the median values for categories and treating these as a single continuous variable. All relative risks were presented with 95% confidence intervals (CI), and reported p values were based on two sided tests. All analyses were performed using the Statistical Analysis System software, release 8.2 (SAS Institute, Cary, North Carolina, USA).
RESULTS
The relationships of waist-hip ratio and height adjusted waist circumference to baseline characteristics in 1986 are shown in tables 1 and 2. Participants with a higher waist-hip ratio and height adjusted waist circumference were more likely to be sedentary but were less likely to use hormone replacement therapy and to consume dietary fibre. Waist circumference was weakly correlated with height (r = 0.15) and strongly correlated with weight (r = 0.80) and BMI (r = 0.79) while waist-hip ratio was not correlated with height (r = −0.01) and was more weakly associated with weight (r = 0.35) and BMI (r = 0.39).
Baseline characteristics of US women according to waist-hip ratio in the Nurses’ Health Study
Baseline characteristics of US women according to height adjusted waist circumference in the Nurses’ Health Study
We documented 3197 cases of cholecystectomy during 514 283 person years of follow up. Age adjusted risk of cholecystectomy was positively associated with waist-hip ratio and waist circumferences (model 1 in tables 3–5). In multivariable analyses adjusting for multiple potential confounding variables (model 2 in tables 3–5), waist to hip ratio was directly associated with risk, with a relative risk of 1.97 (95% CI 1.66–2.35; p trend <0.0001) for women with a waist to hip ratio of 0.86 or higher compared with women with a waist to hip ratio of less than 0.70. Women with a height adjusted waist circumference of 36 inches or larger had a relative risk of 3.87 (95% CI 3.12–4.79; p trend <0.0001) compared with women with a height adjusted waist circumference of less than 26 inches. For women with a crude waist circumference of 36 inches or larger compared with women with a crude waist circumference of less than 26 inches, the relative risk was 3.40 (95% CI 2.84–4.07; p trend <0.0001).
Adjusted relative risks of cholecystectomy according to waist-hip ratio among US women in the Nurses’ Health Study
Adjusted relative risks of cholecystectomy according to height adjusted waist circumferences among US women in the Nurses’ Health Study
Adjusted relative risks of cholecystectomy according to crude waist circumferences among US women in the Nurses’ Health Study
Relative risks were attenuated when multivariable models were fit to adjust simultaneously for regional (waist circumference or waist to hip ratio) and total adiposity (BMI) measures as well as for other risk factors of gall stone disease (model 4 in tables 3–5). Waist to hip ratio was directly associated with risk, with a relative risk of 1.39 (95% CI 1.16–1.66; p trend <0.0001) for women with a waist to hip ratio of 0.86 or higher compared with women with a waist to hip ratio of less than 0.70. Women with a height adjusted waist circumference of 36 inches or larger had a relative risk of 1.96 (95% CI 1.53–2.51; p trend <0.0001) compared with women with a height adjusted waist circumference of less than 26 inches. For women with a crude waist circumference of 36 inches or larger compared with women with a crude waist circumference of less than 26 inches, the relative risk was 1.72 (95% CI 1.39–2.13; p trend <0.0001).
To compare waist-hip ratio and waist circumference using similar distributions, we also performed multivariable analyses using deciles of waist-hip ratio and waist circumference. After adjustment for BMI, recent weight change, and other potential risk factors, as in model 4 in tables 3–5, women in the highest decile of height adjusted waist circumference had a relative risk of 1.86 (95% CI 1.49–2.32; p trend <0.0001) for cholecystectomy compared with those in the lowest decile. The relative risk was 1.47 (95% CI 1.27–1.70; p trend <0.0001) when women in the highest decile were compared with those in the 5th decile. For crude waist circumference measure, the relative risk was 1.72 (95% CI 1.39–2.12; p trend <0.0001) when extreme deciles were compared. The relative risk was 1.46 (95% CI 1.26–1.70; p trend <0.0001) when women in the highest decile were compared with those in the 5th decile. Women in the highest decile of waist-hip ratio had a relative risk of 1.35 (95% CI 1.14–1.60; p trend = 0.0001) compared with those in the lowest decile. The relative risk was 1.23 (95% CI 1.09–1.38; p trend = 0.0001) when women in the highest decile were compared with those in the 5th decile.
We deliberately did not control for diabetes because diabetes is a potential biological mediator and may be an effect of obesity. However, to assess residual effects we added the potential biological mediator into the multivariable models. After adjustment for diabetes and other covariates, as in model 4 in tables 3–5, the relative risk was 1.38 (95% CI 1.16–1.65; p trend <0.0001) for women with a waist to hip ratio of 0.86 or higher compared with women with a waist to hip ratio of less than 0.70. Women with a height adjusted waist circumference of 36 inches or larger had a relative risk of 1.95 (95% CI 1.53–2.50; p trend <0.0001) compared with women with a height adjusted waist circumference of less than 26 inches. For women with a crude waist circumference of 36 inches or larger compared with women with a crude waist circumference of less than 26 inches, the relative risk was 1.72 (95% CI 1.39–2.12; p trend <0.0001). The significant positive association persisted even after controlling for the potential biological mediator.
Measurements of central obesity were associated with increased risk of gall stone disease in stratified analyses, independently of BMI (figs 1, 2). Participants were cross classified by both measurements of central obesity and BMI in quartiles. As shown in fig 1, a higher waist to hip ratio was associated with an increased risk of gall stone disease regardless of BMI quartile. The relative risk was 3.44 (95% CI 2.87–4.13) for the combination of the highest BMI and the highest waist to hip ratio quartiles compared with the opposite extreme. The test of interaction between waist to hip ratio associated gall stone disease risk gradient and BMI was not significant (p = 0.34). As shown in fig 2, larger height adjusted waist circumference was also associated with increased risk of gall stone disease, regardless of BMI quartile. The relative risk was 3.63 (95% CI 3.14–4.20) for the combination of the highest BMI and the largest height adjusted waist circumference quartiles compared with the opposite extreme. There was no statistically significant interaction between BMI and height adjusted waist circumference (p = 0.67).
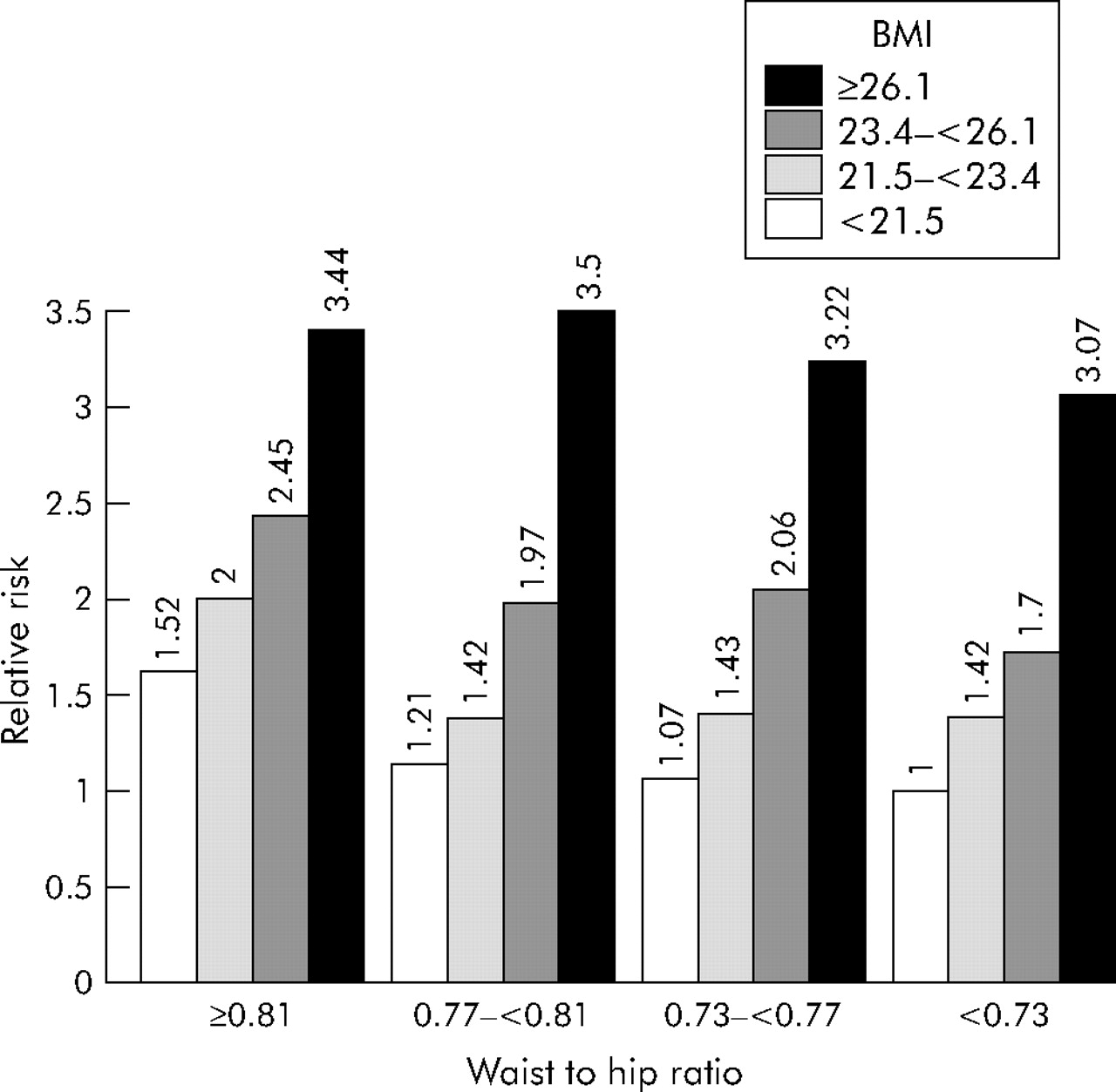
Multivariable relative risks (RRs) of cholecystectomy are illustrated according to waist hip ratio and body mass index (BMI). Waist-hip ratio and BMI are stratified by quartiles and RRs are adjusted for the same covariates as those of model 2 in tables 3–5. The 95% confidence intervals for the 16 RRs are as follows: 1.00 (referent), 1.07 (0.84–1.36), 1.21 (0.94–1.57), 1.52 (1.11–2.08), 1.42 (1.13–1.78), 1.43 (1.14–1.79), 1.42 (1.12–1.79), 2.00 (1.57–2.55), 1.70 (1.34–2.14), 2.06 (1.67–2.56), 1.97 (1.60–2.43), 2.45 (2.00–3.01), 3.07 (2.41–3.92), 3.22 (2.60–4.00), 3.50 (2.89–4.25), 3.44 (2.87–4.13).

{kind=link}
{kind=link}
Multivariable relative risks (RRs) of cholecystectomy are illustrated according to height adjusted waist circumference and body mass index (BMI). Waist circumference and BMI are stratified by quartiles and the RRs are adjusted for the same covariates as those of model 2 in tables 3–5. The 95% confidence intervals for the 16 RRs are as follows: 1.00 (referent), 1.37 (1.11–1.69), 1.61 (1.14–2.26), 3.10 (1.57–6.10), 1.37 (1.11–1.71), 1.54 (1.28–1.84), 1.79 (1.47–2.19), 1.97 (1.33–2.90), 2.11 (1.55–2.86), 1.80 (1.48–2.20), 2.11 (1.79–2.49), 2.72 (2.25–3.28), 1.95 (0.86–4.40), 2.80 (1.97–3.97), 3.41 (2.85–4.07), 3.63 (3.14–4.20).
We also examined whether the association between height adjusted waist circumference and risk of cholecystectomy varied across strata of women based on various potential confounders for gall stone disease. After repeating the multivariable analyses within subgroups, the positive associations between height adjusted waist circumference and risk of cholecystectomy persisted in all subgroups without apparent effect modification of the relationship (table 6).
Multivariable relative risks of cholecystectomy stratified by selected risk factors according to adjusted waist circumference among US women in the Nurses’ Health Study*
To evaluate the potential for detection bias due to increased medical surveillance of overweight women, we additionally excluded women without a routine medical check-up during the first two year follow up period. After adjustment for BMI, recent weight change, and other potential risk factors, waist to hip ratio was directly associated with risk, with a relative risk of 1.49 (95% CI 1.22–1.81; p trend <0.0001) for women with a waist to hip ratio of 0.86 or higher compared with women with a waist to hip ratio of less than 0.70. The relative risk for women with a height adjusted waist circumference of 36 inches or larger had a relative risk of 2.04 (95% CI 1.56–2.68; p trend <0.0001) compared with women with a height adjusted waist circumference of less than 26 inches. For women with a crude waist circumference of 36 inches or larger compared with women with a crude waist circumference of less than 26 inches, the relative risk was 1.88 (95% CI 1.49–2.38; p trend <0.0001).
Women who did not provide complete waist and hip circumference measurements were excluded from the analysis. To explore the possibility that the remaining study population might differ in their relation between BMI and risk of cholecystectomy, we compared the multivariable relative risks, after adjustment for potential confounding variables, between those who provided complete waist and hip circumference measurements and those who did not. Among women who provided complete waist and hip circumference measurements, those with a BMI ⩾ 40.0 had a relative risk of 2.71 (95% CI 1.96–3.74; p for trend <0.001) compared with those with a BMI <20.0. Among women who did not provide complete waist and hip circumference measurements, the relative risk was 2.66 (95% CI 1.86–3.80; p for trend <0.001). Among this subset, the risk for cholecystectomy associated with BMI was not materially different from those of the original population for analysis.
DISCUSSION
In this large prospective cohort study, we found that measures of regional fat distribution were independently associated with the risk of cholecystectomy in women. Both waist-hip ratio and waist circumference were significantly associated with an increased risk of cholecystectomy, even after controlling for BMI. These measures of central adiposity appeared to capture additional information about risk that was not encompassed by BMI. Control for several risk factors had only a small effect on these relations. Our results suggest that regional fat distribution and central adiposity may be important for identifying women at high risk for cholecystectomy.
The validity of BMI as a measure of total body fatness has been assessed by comparison with densitometry. Correlation coefficients with per cent body fat have generally been approximately 0.8.16 However, BMI as a useful measure of total obesity does not distinguish between lean body mass and body fat. Even though weight or BMI remains stable or may even decrease because of loss of lean body mass due to chronic diseases or inactivity, adiposity in older people still may increase.20,21 Fat mass tends to accumulate intra-abdominally with age,22 so the importance of abdominal adiposity in metabolic disturbances and health hazards is greater in older persons.23 Waist measurement may be a good estimate of overall body fat, because a large waist is an unambiguous indicator of excess body fat except in the presence of abdominal tumours, pregnancy, or fluid accumulation. It has been shown that BMI tends to peak at approximately 60 years of age and declines thereafter, whereas the average waist circumference and waist to hip ratio increase through all age groups.24
Both waist to hip ratio and waist circumference are relatively easy to obtain and appear to impart clinically useful information regarding risk of gall stone disease. A larger waist circumference or waist to hip ratio among persons of equal weight may be a marker of increased abdominal visceral adiposity as well as overall adiposity. However, individual circumference measures, rather than waist to hip ratios, have less measurement errors,25 and may be more practical for weight guidelines. Because adjusting waist for height did not appreciably influence the magnitude of association with risk of gall stone disease, and because waist measurement is easy to make, simple waist circumference may have practical importance in clinical and public health settings.
Epidemiological evidence for an association of abdominal obesity with gall bladder disease has been mixed. An ultrasonographic survey in a Mexican population reported that waist to hip ratio was not related to gall bladder disease.14 There was no significant association of waist-hip ratio, after adjusting for BMI, with gall bladder disease in a study of middle aged Japanese military officials.13 However, in a population ultrasonographic survey of gall stone prevalence in England, gall stone prevalence had a stepwise relationship with waist to hip ratio.9 In a US population ultrasonographic survey for gall stones, waist to hip ratio was also found to be related to gall bladder disease.26
There are plausible biological pathways through which central adiposity may cause development of gall stone disease.27–29 Visceral fat is more metabolically active and thus increases hepatic exposure to unesterified fatty acids and decreases insulin sensitivity. Studies have suggested a relationship between gall stone disease and the metabolic syndrome linked to abdominal obesity, of which the cardinal feature is hyperinsulinaemia. Hyperinsulinaemia may cause increased hepatic cholesterol secretion and cholesterol supersaturation of bile by upregulating hepatocyte low density lipoprotein receptors or by activating hydroxymethylglutaryl coenzyme A reductase.30 Insulin might also increase gall stone risk through an effect on gall bladder motility.31 In a recent study, gall bladder volume in the fasting state increased with increasing intra-abdominal fat mass and was higher in subjects with impaired glucose tolerance.32 Gall stone pathogenesis in obesity appeared to be influenced by total body fat mass and its regional distribution.
In this cohort, because we collected data prior to the end points, it is unlikely that self reported anthropometric measurements were influenced by gall stone disease. In addition, we have demonstrated the validity of self reported measurements of body weight and of waist and hip circumferences.17
It was not feasible to perform screening ultrasonography for the presence of gall stones in this large study population. Hence we focused on gall stone disease resulting in cholecystectomy. It is likely that there was considerable under-ascertainment of gall stones because most gall stones are asymptomatic. Some undiagnosed gall stone cases might be present at baseline; however, it was unlikely that the presence of asymptomatic gall stones at baseline was associated with the reporting of anthropometric measurements. Our findings were unlikely biased due to asymptomatic gall stones because relative risk estimation in follow up cohort studies would not be biased by uniform under-ascertainment.19 We attempted to estimate the incidence of newly symptomatic gall stones resulting in cholecystectomy, which is the clinically relevant portion of gall stone disease.
In conclusion, these prospective data suggest a significant association between central adiposity and risk of cholecystectomy in women. Abdominal circumference and waist to hip ratio as measures of abdominal adiposity predict the risk independently of body mass index.
Acknowledgments
We are indebted to the participants in the Nurses’ Health Study for their continuing dedication and commitment to the study. We also thank the research staff in the Nurses’ Health Study for their expert help.
REFERENCES
Footnotes
-
Grant support for the study was obtained from research grants (CA55075 and DK46200) from the National Institutes of Health.
-
Conflict of interest: None declared.
Linked Articles
- Digest