Article Text

Abstract
Background The risk for acidic reflux is mainly determined by the position of the gastric acid pocket. It was hypothesised that compounds affecting proximal stomach tone might reduce gastro-oesophageal reflux by changing the acid pocket position.
Objective To study the effect of azithromycin (Azi) on acid pocket position and acid exposure in patients with gastro-oesophageal reflux disease (GORD).
Methods Nineteen patients with GORD were included, of whom seven had a large hiatal hernia (≥3 cm) (L-HH) and 12 had a small or no hiatal hernia (S-HH). Patients were randomised to Azi 250 mg/day or placebo during 3 days in a crossover manner. On each study day, reflux episodes were detected using concurrent high-resolution manometry and pH-impedance monitoring after a standardised meal. The acid pocket was visualised using scintigraphy, and its position was determined relative to the diaphragm.
Results Azi reduced the number of acid reflux events (placebo 8.0±2.2 vs Azi 5.6±1.8, p<0.01) and postprandial acid exposure (placebo 10.5±3.8% vs Azi 5.9±2.5%, p<0.05) in all patients without affecting the total number of reflux episodes. Acid reflux occurred mainly when the acid pocket was located above, or at the level of, the diaphragm, rather than below the diaphragm. Treatment with Azi reduced hiatal hernia size and resulted in a more distal position of the acid pocket compared with placebo (below the diaphragm 39% vs 29%, p=0.03). Azi reduced the rate of acid reflux episodes in patients with S-HH (38% to 17%) to a greater extent than in patients with L-HH (69% to 62%, p=0.04).
Conclusion Azi reduces acid reflux episodes and oesophageal acid exposure. This effect was associated with a smaller hiatal hernia size and a more distal position of the acid pocket, further indicating the importance of the acid pocket in the pathogenesis of GORD.
clinical trial registration http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=1970 NTR1970.
- Gastro-oesophageal reflux disease
- gastro-oesophageal junction
- prokinetic agent
- acid-related diseases
- anti-reflux therapy
- gastro-oesphageal junction
- nuclear medicine
- colorectal motility
- liver function test
- liver imaging
- gastric motility
- achalasia
- functional bowel disorder
- motility disorders
- dyspepsia
- achalasia
Statistics from Altmetric.com
- Gastro-oesophageal reflux disease
- gastro-oesophageal junction
- prokinetic agent
- acid-related diseases
- anti-reflux therapy
- gastro-oesphageal junction
- nuclear medicine
- colorectal motility
- liver function test
- liver imaging
- gastric motility
- achalasia
- functional bowel disorder
- motility disorders
- dyspepsia
- achalasia
Significance of this study
What is already known about this subject?
-
After food intake, gastric acid floats on top of the ingested food; this is also referred to as the gastric acid pocket.
-
The acid pocket functions as a reservoir from which acid refluxes into the oesophagus.
-
The position of the acid pocket relative to the crural diaphragm is an important determinant of the acidity of the refluxate.
-
The position of the acid pocket is largely determined by the presence of a hiatus hernia.
What are the new findings?
-
Azithromycin (Azi) reduces acid reflux episodes and oesophageal acid exposure in patients with gastro-oesophageal reflux disease (GORD).
-
A reduction in hiatal hernia size results in a more distal position of the acid pocket relative to the diaphragm, probably explaining the reduction in acid reflux. This effect is mainly seen in patients with a small hiatal hernia.
-
Azi significantly reduces hiatal hernia size, providing evidence for a new potential explanation of the effect of prokinetics on acid exposure.
How might it impact on clinical practice in the foreseeable future?
-
These data indicate that modulation of the position of the acid pocket has an impact on the acidity of the refluxate, further confirming that the acid pocket is a potential target in GORD treatment.
Introduction
Gastro-oesophageal reflux is a physiological phenomenon in which gastric contents flow back into the oesophagus. When reflux causes symptoms such as heartburn or regurgitation and/or oesophageal damage, it is referred to as gastro-oesophageal reflux disease (GORD), a common chronic condition affecting 10–20% of the adult population.1 ,2
Most reflux episodes occur after a meal, when the stomach is filled with ingested food. In contrast to the belief that meal ingestion buffers gastric acid, acid reflux episodes occur even in the early postprandial period.3 Fletcher et al elegantly showed that gastric acid floats on top of the meal, acting as a reservoir from which acid can enter the oesophagus during episodes of opening of the oesophago-gastric junction. This unbuffered pool of gastric acid is referred to as the gastric acid pocket.4
The position of the acid pocket relative to the crural diaphragm is an important determinant of the acidity of the refluxate. We previously showed that 74–85% of reflux episodes are acidic when the acid pocket is located above, or at the level of, the diaphragm. In contrast, only 7–20% of reflux episodes are acidic if the acid pocket is located below the diaphragm.3 The position of the pocket relative to diaphragm, on the other hand, is largely determined by the presence of a hiatal hernia. Especially in patients with a large hiatal hernia (L-HH), the acid pocket is commonly located above the diaphragm, facilitating the occurrence of acid reflux events.3 ,5 This insight implies that drugs affecting the position of the acid pocket (hiatal hernia) may alter acid exposure.
Prokinetic agents such as macrolides increase gastric emptying and, in addition, increase proximal stomach tone and lower oesophageal sphincter (LOS) pressure, presumably via a cholinergic pathway mediated by motilin receptors or possibly by serotonin receptors.6 Such properties make these compounds interesting candidates to alter the acid pocket position. Recently, Mertens et al reported that the macrolide azithromycin (Azi), a macrolide similar in structure and function to erythromycin,7 reduced the rate of reflux episodes in patients with a lung transplant.8 Interestingly, Azi mainly affected the rate of acidic reflux, leaving the number of weakly acid reflux events unchanged. As the acidity of the refluxate is mainly determined by the position of the acid pocket, we hypothesised that this action of Azi was mediated by a reduction in hiatal hernia size, thereby leading to an alteration in the position of the acid pocket. To evaluate this hypothesis, we examined the effect of Azi on gastro-oesophageal reflux and the acid pocket position in patients with GORD.
Patients and methods
Patients
The study was performed in 19 patients with proven GORD, defined by the presence of oesophagitis observed during upper endoscopy and/or pH-metry with an acid exposure of >4.5%, in combination with typical GORD symptoms.9 None of the patients had undergone previous gastrointestinal surgery or was taking medication known to influence oesophageal motor function. Hiatal hernia size was measured by high-resolution manometry (HRM), and patients were divided into L-HH (≥3 cm) or small or no hiatal hernia (S-HH) (<3 cm) according to the size of the hiatal hernia. One patient withdrew consent after the first study day owing to discomfort. The study was approved by the medical ethics committee of the Academic Medical Center. Written informed consent was obtained from all subjects before enrolment in the study.
Study design
The study had a randomised, double-blind, crossover design. Patients were randomised to Azi 250 mg or placebo by the pharmacy where the code was stored until the end of the study. Both the investigators and the patients were blinded to the treatment. Study medication was taken during a 3-day course ending on the study day, with comparable dosing of Azi to that used in the earlier study by Mertens et al.8 Acid-suppressive medication was stopped at least 7 days before each study day. The study day protocol was repeated after a minimal wash-out period of 2 weeks.
Study day protocol
Subjects were studied after an overnight fast of at least 12 h. Reflux episodes were detected using concurrent HRM and pH-impedance monitoring, and scintigraphy was performed to localise the acid pocket relative to the crural diaphragm.
At 30 min before insertion of the catheters, 350 MBq 99mTc-pertechnetate was injected intravenously. Pertechnetate behaves as a chloride ion, and is secreted by the parietal cells of the stomach.10 When this technique is used, acid distribution in the stomach can be visualised scintigraphically as validated previously.3
Before introduction of the HRM catheter, two sealed markers impregnated with 99mTc-pertechnetate were attached to the catheter, one to the distal end of the catheter and one between sensors 13 and 14 to visualise the exact location of the catheter during scintigraphy. These markers were used to integrate manometry and scintigraphy as described below in more detail.
The HRM catheter and the pH-impedance catheter were inserted transnasally. The HRM catheter was positioned with the five most distal sensors positioned in the stomach. The pH sensor of the pH-impedance catheter was placed 5 cm above the upper border of the LOS. Subsequently, the patients were positioned in upright position in front of the scintigraphy camera. First, a baseline fasting recording was obtained during 5 min. Then subjects consumed a standardised meal in 10 min consisting of 200 ml orange juice and two pancakes with jam (510 kcal). After the meal scintigraphic, HRM and pH-impedance recordings were obtained for 105 min.
Recording methods
HRM was performed using a solid-state HRM catheter (Unisensor, Attikon, Switzerland) with 36 solid-state pressure transducers spaced 1 cm apart. Pressure sensors were zeroed before insertion. The sample rate was 50 Hz, and data were collected and analysed with the MMS Solar system (MMS, Enschede, the Netherlands).
For pH-impedance measurement a Unisensor pH-impedance catheter (Unisensor, Attikon, Switzerland) containing one ISFET pH sensor and eight impedance electrodes was used, allowing impedance recordings at 3, 5, 7, 9, 15 and 17 cm above the upper border of the LOS. Data were collected using the MMS Solar system. Before each study the pH electrode was calibrated with pH 4.0 and pH 7.0 solutions (Medtronic A/S, Skovlunde, Denmark).
Dynamic scintigraphic images were acquired on a gammacamera system (Diacam; Siemens Medical Solutions, Illinois, USA), equipped with a low-energy, all-purpose collimator. Dynamic recordings were made for 2 h (720 views, 10 s/view, 120 min total acquisition time). Every acquisition was processed on a Hermes processing station (Hermes Medical Solutions, Stockholm, Sweden) for further analysis.
Data analysis
Reflux episodes were detected by pH impedance and each liquid or mixed reflux event was defined as acidic reflux when pH<4, as weakly acidic when pH≥4 and pH<7 and as non-acidic when pH≥7. A liquid reflux was defined as a fall in impedance of ≥40% of baseline impedance starting at the most distal segment and propagating retrograde to at least the next measuring segment. Pure gas reflux was defined as a rapid (>3000 Ω/s) rise in impedance, occurring simultaneously in at least two impedance sites, in the absence of swallowing. Mixed reflux was defined as gas reflux occurring during or immediately before liquid reflux. Oesophageal clearance time and proximal extent of refluxate were determined for each reflux episode.
For each reflux episode, HRM recordings were used to determine the exact distance from the crural diaphragm to the markers on the catheter for the position of the acid pocket and to the LOS for hiatal hernia size. The lower and upper border of the crural diaphragm and the middle of the LOS zone were determined (figure 1). Hiatal hernia size was defined as the distance from the lower end of the diaphragm to the middle of the LOS. Additionally, we determined whether the hiatal hernia was in the reduced (one high-pressure zone) or non-reduced state (two high-pressure zones), as described and validated by Bredenoord et al.11 For the non-reduced state, a trough with a pressure of at least 10 mm Hg lower than the two high-pressure zones had to be present.

(A) A schematic view of the study set-up. Two radionuclide markers are attached to the high-resolution manometry (HRM) catheter, which can be observed on the scintigraphic images (B), on the proximal and distal end of the acid pocket. The representative image of the HRM and pH-impedance (pH-Imp) recording is shown in (C), with a mixed reflux episode as a result of a transient lower oesophageal sphincter relaxation in a patient with a large hiatal hernia. The lower oesophageal sphincter is marked with 1, and the upper and lower borders of the crural diaphragm are marked with 2 and 3, respectively.
Subsequently, calibrated Hermes software was used to measure the distance from the proximal end of the gastric acid pocket to the markers on the catheters on one image before the reflux event to calculate the distance between the acid pocket and the crural diaphragm. The position of the acid pocket was classified in three categories relative to the crural diaphragm: below the diaphragm, at the level of the diaphragm or above the level of the diaphragm.
Measurements of the distances between the acid pocket and the diaphragm were made through a straight line in a planar posterior view of the stomach. A pocket was considered as present when a clear pool of radiolabelled activity was distinguishable in the proximal stomach. The radiolabelled markers on the catheter were scintigraphically visualised as clear dots. Acid pocket length and width were determined for each reflux event by measuring the distance from the proximal to the distal end of the radiolabelled activity for the length, and between both lateral ends for the width, respectively.
For each reflux episode the underlying mechanism was classified using previously described criteria12 as a transient lower oesophageal sphincter relaxation (TLOSR), swallow induced, low LOS pressure, abdominal straining or of unknown cause. Briefly, a TLOSR was defined as a decrease in LOS pressure at a rate of ≥1 mm Hg/s, with a duration of 10 s, a nadir pressure ≤2 mm Hg and absence of swallowing from 4 s before, to 2 s after, the start of the relaxation. Swallow-induced reflux was defined similarly to TLOSRs but with the presence of a swallow. Low LOS pressure was defined as a period of at least 30 s with an end-expiratory LOS pressure of ≤3 mm Hg. Abdominal straining was detected as a sharp and brief increase in gastric pressure of at least 30 mm Hg with a simultaneous rise in oesophageal pressures.
Statistical analysis
Based on data from previous studies3 ,13 a mean number of postprandial acid reflux episodes of 10 per study day was assumed in patients with GORD. To detect a difference of 30% in acid reflux episodes with a statistical power of 80% and a two-sided α of 0.05, a total of 16 patients was required in a crossover design. Thirty per cent reduction in reflux episodes is a clinically relevant difference and is seen in studies with a comparable design.14 ,15 To compensate for drop-outs, we decided to include 19 patients.
Statistical analysis was preformed using SPSS V.20.0 software (IBM corporation). Data are presented as mean ± SEM. Continuous data were compared using a paired t test or with a linear mixed model (LMM) when multiple measurements for patients were made. Comparisons of proportions were performed using a generalised estimating equations (GEE) logistic regression model, with subject as clustering factor, and treatment as independent variable. Pearson's correlation was used for correlations. All p values were two-tailed and a p value <0.05 was considered as statistically significant.
Results
Patients
Nineteen patients with GORD (13 male; median age 56 years, range 45–67 years) were included. HRM analysis showed that seven patients had a L-HH (≥3 cm) and 12 had a S-HH (<3 cm).
Acid reflux episodes and oesophageal acid exposure
In the 19 patients studied, a total of 494 reflux episodes was detected, of which 245 (49.6%) episodes were acidic. The total number of reflux episodes for each patient was not altered by Azi in comparison with placebo (13.8±2.0 vs 14.0±1.7, p=0.79) (figure 2). However, the number of acid reflux events and postprandial acid exposure were significantly reduced by Azi compared with placebo (8.0±2.2 vs 5.6±1.8, p<0.01 and 10.5±3.8% vs 5.9±2.5%, p=0.01 respectively). Conversely, the number of weakly acid reflux episodes was increased in Azi in comparison with placebo (figure 2). A TLOSR was the underlying cause in 328 (66.4%) of the 494 reflux episodes recorded. The number of TLOSRs did not differ between Azi and placebo.

The number of reflux events is not altered by azithromycin (Azi) (A), but the oesophageal acid exposure and the number of acid reflux events is lowered by Azi compared with placebo in all patients (B and C). As a result, the number of weakly acid reflux episodes is higher during treatment with Azi (D).
Acid pocket position before a reflux event
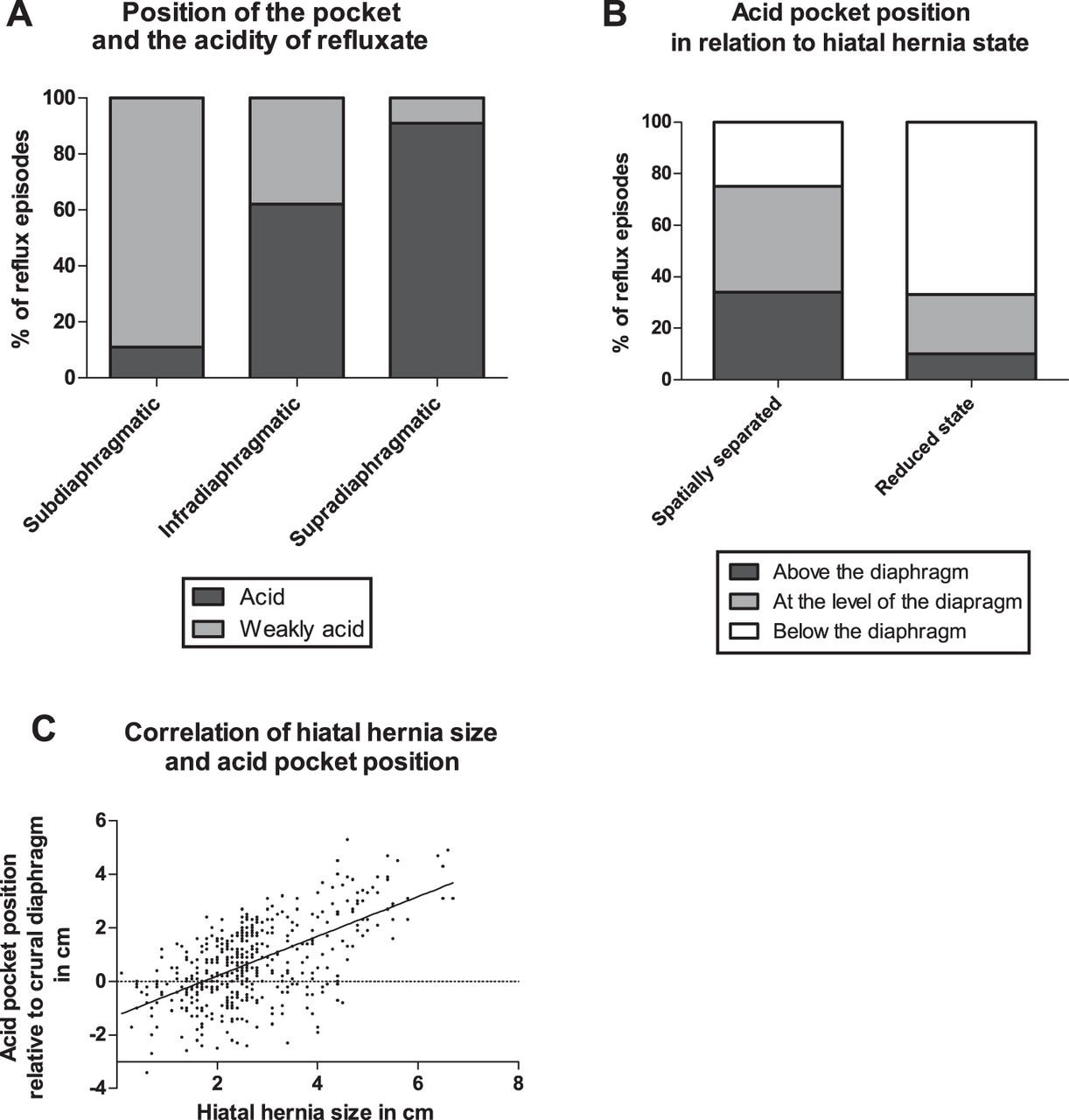
The acid pocket was scintigraphically visible in all patients within 15 min after meal ingestion. Acid reflux occurred mainly when the acid pocket was located above (117/129 reflux episodes (91%)), or at the level of (106/171 (62%)), the diaphragm, but seldom when the pocket was located below the diaphragm (18/168 (11%)) (figure 3).
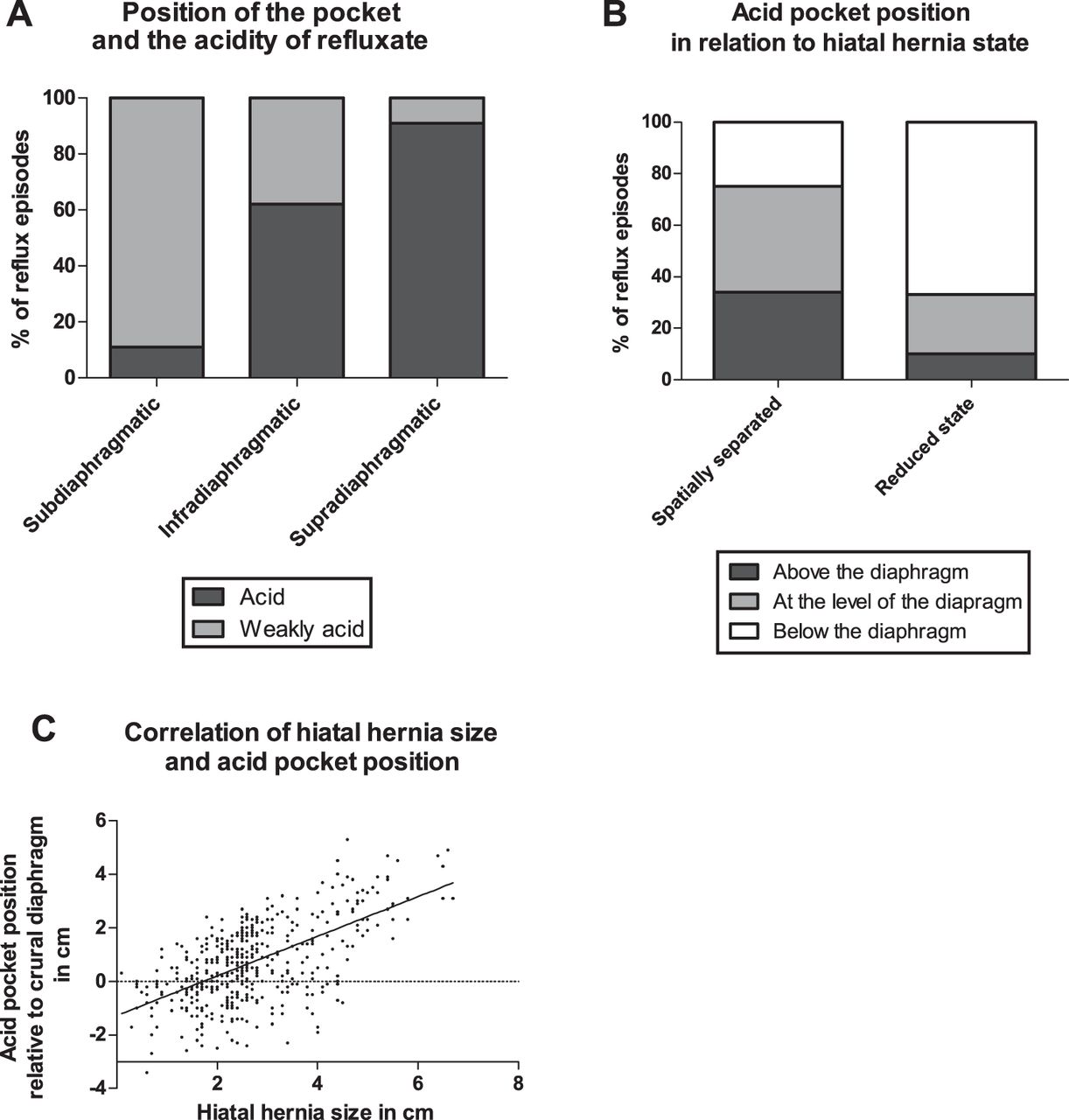
The acidity of the refluxate is mainly determined by the position of the acid pocket relatively to the crural diaphragm (A). When the crural diaphragm and the lower oesophageal sphincter are spatially separated, the acid pocket is located significantly more often above, or at the level of, the diaphragm than when the hiatal hernia is in the reduced state (B). The hiatal hernia size in all patients correlates with the distance of the acid pocket relative to the diaphragm (C).
During treatment with Azi, the acid pocket was more often located below the diaphragm (39±9 vs 29±8%, p=0.03, GEE) (figure 4). The mean acid pocket length did not differ between Azi and placebo (4.2±0.5 cm and 4.6±0.5 cm respectively, p=0.76, LMM).
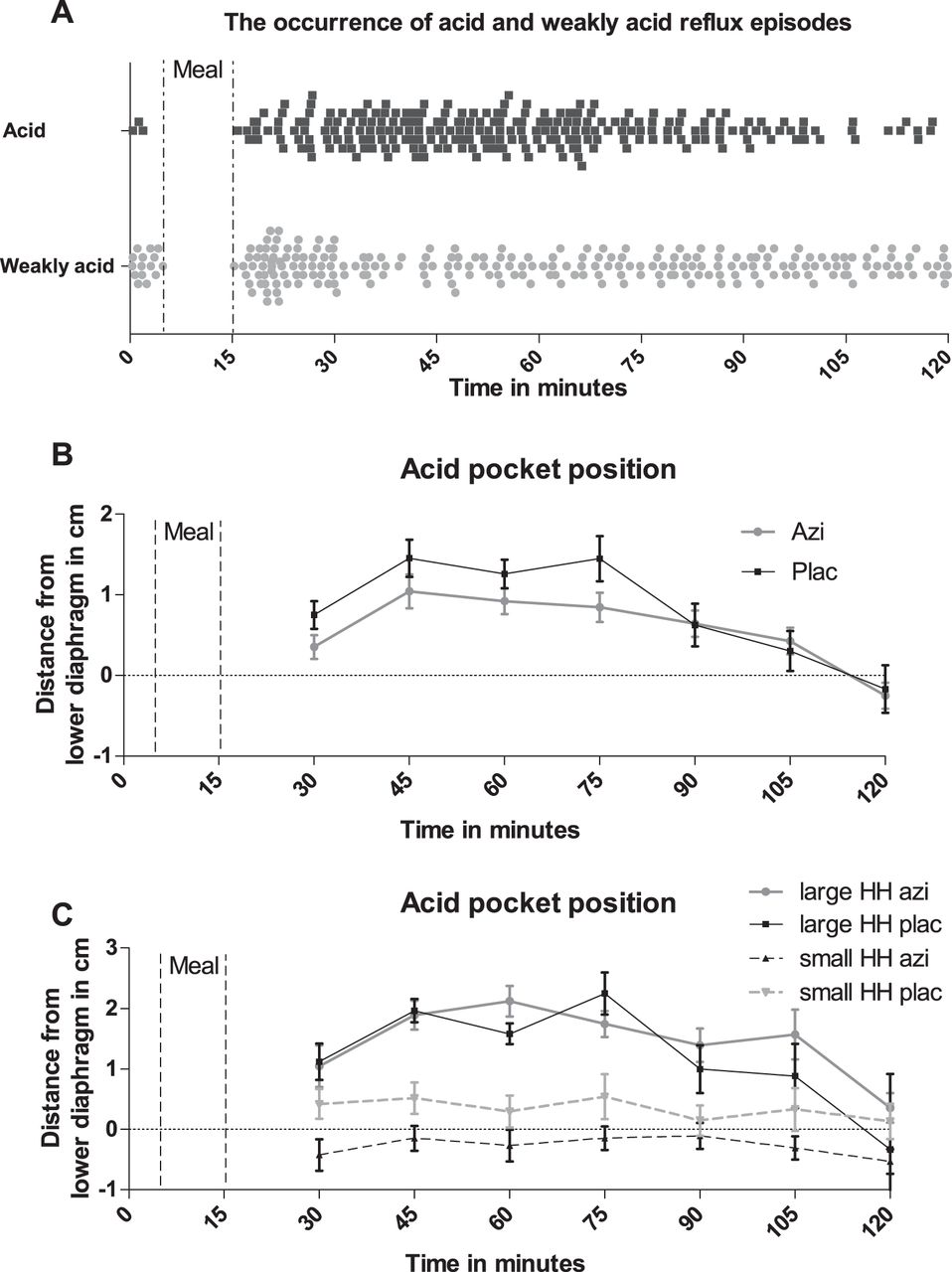
Most acid reflux episodes occur starting from 10–15 min postprandial till 60 min postprandial (A). In this period, the acid pocket has its most proximal position. Azithromycin (Azi) leads overall to a more distal position of the acid pocket compared with placebo (B). In (C) the acid pocket position relative to the crural diaphragm is shown when the subdivision in small and a large hiatal hernia (HH) is formed, demonstrating that the observed effect on altered acid pocket position mainly results from patients with a small HH.
Hiatus hernia size and acid reflux
Hiatal hernia size was measured using HRM as the distance from the lower end of the diaphragm to the middle of the LOS, as shown in figure 1. The size of the hiatal hernia varied during the study affecting the acidity of the refluxate, as previously shown by Bredenoord et al.11 When reflux episodes were acidic, the mean hiatal hernia size was larger than when reflux episodes were weakly or non-acidic (acid 2.8±0.2 vs non-acid 2.4±0.2 cm, p<0.05, LMM). Moreover, when the hiatus hernia was in a non-reduced state (spatial separation between diaphragm and LOS), the risk of acid reflux was significantly increased compared with in the reduced state (59±7% compared with 30±8% of reflux events respectively, p<0.001, GEE). The distance of the acid pocket to the crural diaphragm correlated significantly with hiatal hernia size (r=0.61, p<0.0001 Pearson's correlation), with a larger hiatal hernia size thus leading to a more proximal position of the acid pocket (figure 3). In the reduced state, hiatal hernia size was never more than 2.0 cm.
Proximal extent and oesophageal clearance time
In the total group, the proximal extent of liquid and mixed reflux episodes varied between 5 and 17 cm. During treatment with Azi, the proximal extent was significantly reduced compared with placebo (9.9±0.50 cm vs 8.6±0.44 cm, p<0.01). As acid exposure is also determined by clearance of the refluxate, we assessed the effect of Azi on acid clearance time. Mean clearance time was not significantly altered by Azi (13±1.5 s with Azi vs 17±2.1 s with placebo (p=0.10)).
Small versus large hiatal hernia
Motilides increase proximal stomach tone, thereby reducing the volume of the proximal stomach. We hypothesised that this would affect the position of acid pocket, particularly in patients with a S-HH, by reducing the size of the hiatal hernia. In patients with a L-HH, however, the acid pocket is continuously positioned above the diaphragm,3 reducing the potential of Azi to affect the position of the acid pocket. Based on previous findings, patients were divided into L-HH (≥3 cm) or S-HH (<3 cm) according to the size of the hiatal hernia. Seven patients had a L-HH, whereas 12 had a S-HH.
The total number of reflux episodes was comparable in the two groups (249 in patients with L-HH, and 245 in patients with S-HH). In patients with L-HH, the acid pocket was located above the diaphragm in 45% of reflux episodes, and 99 (91%) of these reflux episodes were acidic. In patients with S-HH, however, the acid pocket was mostly located below (63%) or at the level (29%) of the diaphragm.
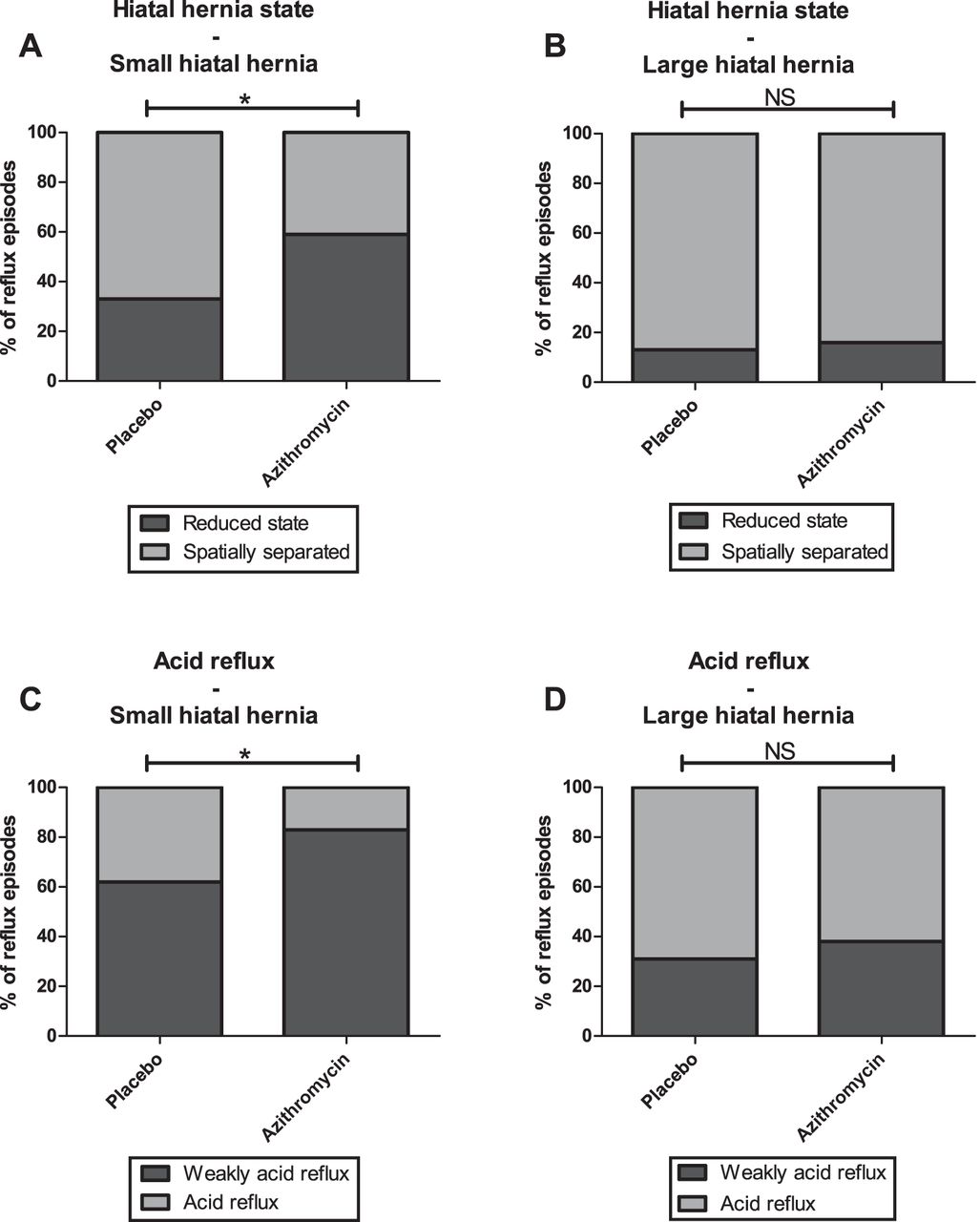
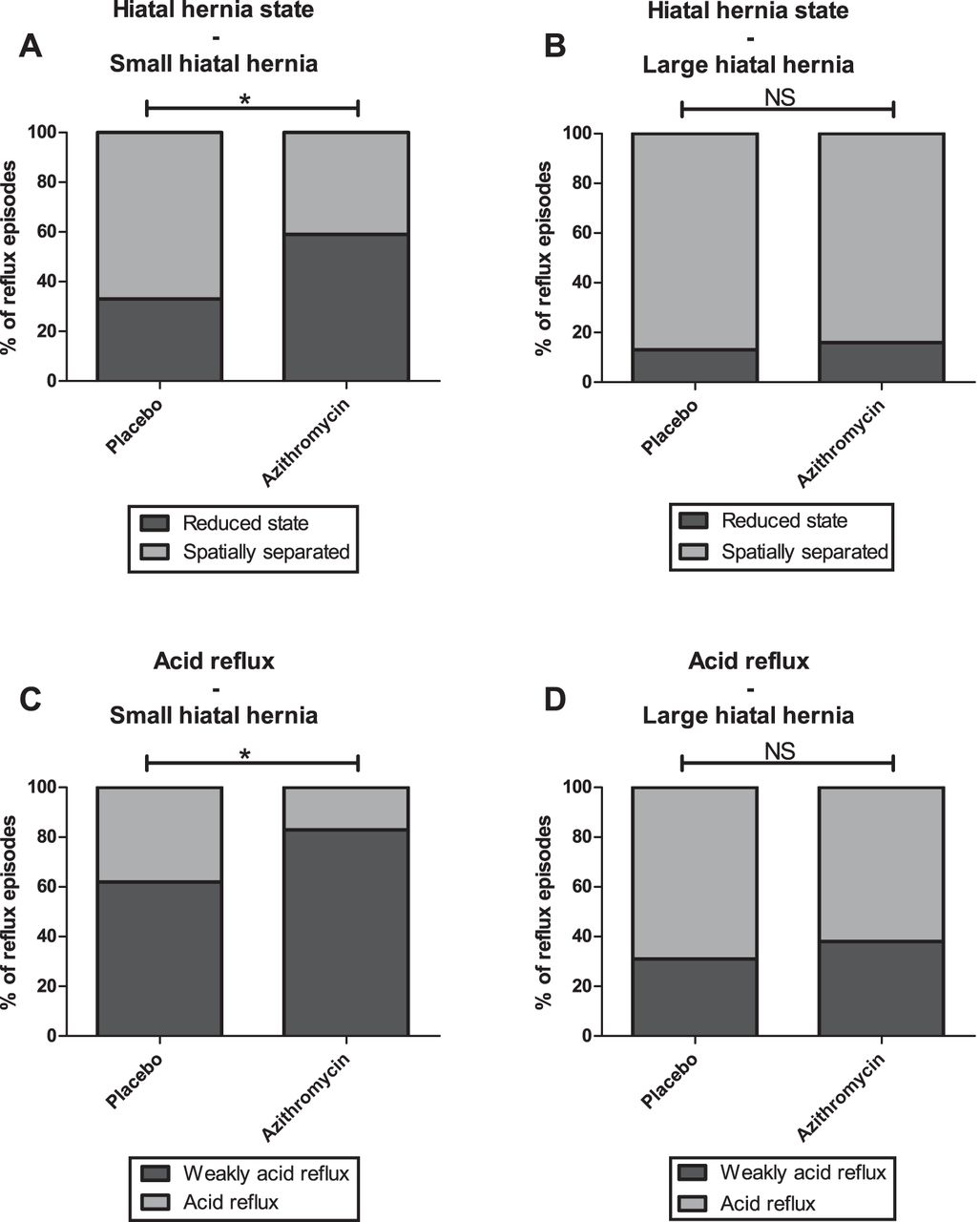
In patients with L-HH, Azi reduced the rate of acid reflux from 69% to 62%. In patients with S-HH, Azi reduced the rate of acid reflux from 38% to 17%, which is a significantly greater effect than in patients with L-HH (p<0.05, GEE), (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment with azithromycin leads more often to a reduced state in patients with a small hiatal hernia (A), but not in patients with a large hiatal hernia (B). As a result, the effect of azithromycin on the rate of acid reflux episodes is significantly larger in patients with a small hiatal hernia (C) than in patients with a large hiatal hernia (D). Statistical analyses are performed using a generalised estimating equations model. *=p<0.05.
In patients with S-HH treatment with Azi led to a significantly smaller mean hiatal hernia size before reflux episodes than with placebo (2.5±0.3 cm vs 2.1±0.2 cm, p<0.05, LMM). In line with this, the hiatal hernia was more often in the reduced state during Azi treatment than during placebo. (figure 5) As a result, the acid pocket in patients with S-HH was more often located below the diaphragm during treatment (69±8% vs 53±8% of reflux episodes respectively, p=0.01, GEE) (figure 4).
In contrast, Azi did not affect the state (reduced state placebo 13±5% and Azi 16±4%, p=0.63, GEE, figure 5), size or the position of the acid pocket (below the diaphragm: placebo 11±5% vs Azi 11±4% of reflux episodes p=0.92, GEE) in patients with a L-HH.
Discussion
In this study we showed that Azi reduces acid reflux episodes and oesophageal acid exposure in patients with GORD. This effect is mainly caused by a more distal position of the acid pocket, probably resulting from a reduction of the hiatal hernia size. These findings provide further insight into the role of the acid pocket and its position in the composition of the refluxate, and provide an additional mechanism explaining the beneficial effect of motilides, and perhaps other prokinetics, on gastro-oesophageal reflux.
After food intake, gastric acid floats on top of the ingested food; this is also referred to as the acid pocket. We recently provided evidence supporting the hypothesis that this pocket functions as a reservoir from which acid refluxes into the oesophagus, especially if the pocket is located above the diaphragm or in the hiatus.3 This study confirms that the risk of having acid reflux is strongly determined by the position of the acid pocket relative to the diaphragm. We found that only 11% of the reflux episodes were acidic when the acid pocket is located below the diaphragm, in contrast to 91% when the pocket is positioned above. As we previously demonstrated that the position of the acid pocket is largely determined by the presence of a hiatal hernia, accurate recording of the position of the hiatal hernia is of great importance when evaluating the interaction between hiatal hernia, acid pocket and reflux. This is particularly important in patients with a S-HH, as concurrent pH-impedance and HRM recording elegantly showed that a hiatal hernia is a dynamic entity—that is, it appears and disappears in time, thereby largely determining the risk of having acidic reflux.11 ,16 When the hiatal hernia is in the reduced state—that is, no separation between LOS and diaphragm, the risk of having acidic reflux is two- to fourfold lower than when the hernia is in non-reduced state.11 ,16 Using the same methodology, but combined with continuous recording of the acid pocket, we were able to study the dynamics of the acid pocket (in contrast to pH pull-through studies) and hiatus hernia in great detail during a prolonged period of time. Hence, we could demonstrate that spatial separation of the LOS and crural diaphragm (hiatal hernia size) is indeed larger before acid reflux events than before weakly acid reflux events, and that a reduction in hiatal hernia size results in a more distal position of the acid pocket relative to the diaphragm. When the hiatal hernia is in the reduced state, the acid pocket is more often located below the diaphragm, and the risk of acidic reflux is lower (30%) than when the hernia is in a non-reduced state (59%). These data confirm that the position of the acid pocket and the size of the hiatal hernia are closely related and are major risks factors for having acid reflux or GORD.
Clinically, the relation between GORD and a hiatal hernia is evident as hiatal hernia size correlates excellently with oesophageal acid exposure and oesophageal damage.12 ,17–19 Accepting that the position of the acid pocket largely determines the acidity of the refluxate, drugs reducing the hiatus hernia or moving the acid pocket more distally should result in reduced acid exposure. To this end, patients with GORD were treated with Azi, a broad-spectrum antibiotic with prokinetic properties, previously shown to reduce acid reflux in patients with a lung transplant.8 In this study, we showed that also in patients with GORD, Azi treatment reduced the number of acid reflux episodes and acid reflux exposure, but increased non-acid reflux. Hence, the total number of reflux events remained unchanged, in line with the finding that Azi had no effect on TLOSRs, the main mechanism underlying GORD.12 Instead, Azi significantly reduced hiatal hernia size. This effect was mainly seen in patients with a S-HH (<3 cm). This was confirmed by the observation that hiatal hernia was in a reduced state in 59% of reflux episodes during Azi compared with 33% during placebo in these patients. In patients with a L-HH (≥3 cm), however, Azi failed to affect the hiatal hernia (reduced vs separated) or alter the position of the acid pocket, probably explaining the larger effect on acid reflux rates in patients with a S-HH.
The exact mechanism by which Azi affects the hiatal hernia and acid pocket position is unclear. Motilides such as Azi and erythromycin act on motilin receptors on nerves and smooth muscle cells mediating an overall prokinetic effect.6 ,20 In the proximal stomach and distal oesophagus, motilides therefore enhance motility leading to increased proximal gastric tone and LOS pressure, presumably via a cholinergic pathway.21–23 One may speculate that increased tone reduces proximal stomach volume, thereby reducing hiatal hernia size forcing the gastric content and acid pocket more distally. This effect is mainly seen in patients with a S-HH, as illustrated by the increase in the reduced state of the HH. In contrast, in patients with a L-HH, the separation of the LOS and the crural diaphragm is too large for the HH to revert to the reduced state.24–26 Alternatively, Azi accelerates gastric emptying and improves mixing of stomach contents, potentially affecting acid pocket properties.23 ,27 Lastly, reduction in acid secretion by Azi might have contributed to the reduced number of acidic reflux events. However, no effect of Azi on acid pocket width and length was seen in our study. It should be emphasised though, that our scintigraphic technique is not sufficiently sensitive to detect subtle changes in acid secretion. Hence, we cannot exclude this possibility.
A limitation of our study is that we only analysed one dose of Azi. However, owing to the nature of the recording methods and the burden of these techniques, we chose to use one low dose comparable to that used in an earlier study on this subject.8 Another possible limitation of our study is that we did not assess gastric emptying.
Our findings provide additional evidence for the importance of the position of the gastric acid pocket as a risk factor for acidic reflux. In addition, our study confirms that the gastric acid pocket may be a possible target for GORD treatment.27–29 Finally, we provide evidence that distal migration of the acid pocket and increased time of the hiatal hernia in the reduced state are new potential explanations for the effect of prokinetics on acid exposure, although the effect of affecting the pocket position was rather limited and primarily seen in patients with a S-HH. The effect of motilin agonists and other prokinetics on gastro-oesophageal parameters has been investigated more extensively in earlier studies, showing a reduction in the proximal extent of the refluxate, accelerated gastric emptying and increased LOS pressure as potential mechanisms explaining the reduction in acid exposure.8 ,30–34 Although a 30% reduction in acid reflux episodes and oesophageal acid exposure as seen in our study is largely beneficial, earlier therapeutic studies with prokinetics have demonstrated a rather small effect on GORD symptoms.33 ,35–37 Our results provide evidence for a new potential explanation of the effect of prokinetics on acid exposure, but whether treatment with prokinetics in GORD leads to a reduction in symptoms remains to be studied.
In theory, therapeutic strategies directly intervening in the composition of the acid pocket may prove more efficient in preventing acid reflux events. Recent studies show that antacid–alginate formulations effectively eliminate or displace the acid pocket, by formation of a raft in the proximal stomach.29 ,38 We hypothesise that this intervention will be successful in patients with S-HH as well as in those with L-HH, as antacid–alginate formulations reduce acid reflux events in patients with and without a hiatal hernia.39
In conclusion, this study demonstrates that Azi reduces the number of acid reflux events and oesophageal acid exposure in patients with GORD, especially in patients with a S-HH. We hypothesise that this effect results from relocation of the acid pocket to a more distal position and a concomitant reduction in hiatal hernia. These data indicate that modulation of the position of the acid pocket has an impact on the acidity of the refluxate, further confirming the importance of the acid pocket in the pathogenesis of GORD.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was provided by medical ethics committee of the Academic Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.