Article Text

Abstract
Objectives: Autoimmune pancreatitis (AIP) is a unique form of chronic pancreatitis, and has a favourable response to corticosteroid treatment (CST). Little is known, however, about the long-term outcome of AIP. This study aimed to document the prognosis without and with CST, and to examine the indication for CST.
Patients and methods: The prognosis and clinical features of 23 patients without CST and 19 patients treated with CST from onset were investigated. In addition, factors concerning the late occurrence of unfavourable events related to AIP were examined.
Results: The patients without CST were 19 men and four women, with an average age of 66 years. After an average observation period of 25 months, 16 patients (70%) developed unfavourable events including obstructive jaundice as a result of distal bile duct stenosis in four, growing pseudocyst in one, sclerogenic changes of extrapancreatic bile duct in nine, hydronephrosis as a result of retroperitoneal fibrosis in one, and interstitial nephritis in one. Patients with obstructive jaundice at onset showed a higher cumulative event occurrence rate (p = 0.025). The patients treated with CST were 16 men and three women, with an average age of 64 years. After an average observation period of 23 months, six patients (32%) developed unfavourable events consisting of interstitial pneumonia in three, and a recurrence of obstructive jaundice in three. In multivariate analysis, CST (HR 0.33, 95% CI 0.12–0.89, p = 0.029) and obstructive jaundice at onset (HR 3.09, 95% CI 1.14–8.32, p = 0.026) were significant predictive factors for unfavourable events.
Conclusion: CST could reduce AIP-related unfavourable events. The early introduction of CST is recommended especially for patients with obstructive jaundice.
- autoimmune pancreatitis
- corticosteroid
- prognosis
- sclerosing cholangitis
- obstructive jaundice
Statistics from Altmetric.com
Autoimmune pancreatitis (AIP) is a unique form of chronic pancreatitis characterised by irregular narrowing of the pancreatic duct, swelling of the pancreas, lymphoplasmacytic infiltration and fibrosis, and favourable response to corticosteroid treatment (CST).1–12 Serologically, elevation of IgG4 is the most remarkable characteristic of this disease.13 14 Pathologically, IgG4-positive plasma cells and obliterative phlebitis are characteristic features.15 16 There are also many reports about associated extrapancreatic lesions such as sclerosing cholangitis,2 5 7 15,17 retroperitoneal fibrosis,5 18 sialoadenitis,19–21 interstitial nephritis,21 22 and interstitial pneumonia.23 24 They often appear simultaneously at the diagnosis of AIP, but sometimes appear before or after the diagnosis of pancreatic lesions. As the concept of AIP becomes widespread, atypical cases without remarkable pancreatic swelling or ductal change have also been reported.6
Previous studies have shown that CST is effective for patients with AIP at least in the short term.1–3 5–12 17–19 22–24 Some studies have, however, reported that clinical symptoms of patients were resolved without CST.3 10 25 As the long-term prognosis of AIP especially without CST is not well known, it still remains to be determined whether CST is necessary for all patients with AIP.
We conducted the present study to elucidate these issues. Initially, we had basically treated the patients without CST by relieving symptoms such as by biliary drainage. We then began to employ CST in many patients after we noticed the late occurrence of sclerosing cholangitis without CST.5 Such AIP-related sclerosing cholangitis, which represents multiple bile duct strictures affecting the intra and extrahepatic biliary trees, has been recognised as one form of extrapancreatic lesion.2 5 7 11 12 15 17 We thus investigated the precise incidence of unfavourable events in these patients. In addition, some non-CST cases are still being followed, especially atypical or asymptomatic cases. We reviewed the outcome and clinical features of all cases with AIP, especially focusing on patients followed without CST, and evaluated the indication for CST in AIP.
PATIENTS AND METHODS
Between 1997 and 2005, 42 patients were diagnosed as having AIP at the University of Tokyo Hospital and affiliated hospitals. Diagnosis was based on the following clinicopathological findings: enlargement of the pancreas or narrowing of the main pancreatic duct; increased serum γ-globulin including IgG and IgG4; the presence of autoantibodies; and characteristic histological findings of fibrotic change with lymphoplasmacytic infiltration. The diagnosis of AIP was made prospectively in all patients except one (patient 13 in table 1), who was diagnosed with unidentified obstructive jaundice in 1993 before the publication of the paper by Yoshida et al.,1 and who was diagnosed as having AIP six years later. As a result, patients diagnosed with AIP by us turned out to fulfill the diagnostic criteria of AIP recently proposed by the Mayo Clinic11 or the revised criteria of the Japan Pancreas Society.12 We diagnosed patients with sclerogenic changes (diffuse irregular strictures) of the extrapancreatic bile duct as sclerosing cholangitis, based on the findings of endoscopic retrograde cholangiograpy or percutaneous transhepatic cholangiography. When bile duct stricture was limited to the distal (intrapancreatic) area, we did not regard it as sclerosing cholangitis because it could be influenced by pancreatic oedema. Sialoadenitis was diagnosed on the basis of the findings of palpation, imaging studies such as gallium scintigraphy, and the absence of sicca syndrome A and sicca syndrome B antibodies. Retroperitoneal fibrosis was diagnosed on the basis of the findings of computed tomography; that is, a soft tissue density mass around the abdominal aorta was diagnosed as retroperitoneal fibrosis. Obstructive jaundice was defined as a condition in which increased levels of biliary enzymes and total bilirubin (>1.5 mg/dl), together with dilatation of the bile duct, were observed. Abdominal pain included abdominal discomfort in this study.
Among 42 patients, 23 patients were followed up without CST because they were asymptomatic or became asymptomatic after biliary drainage. Most of them (20/23) had been diagnosed before 2003, from when we became concerned about the late occurrence of sclerosing cholangitis in AIP without CST.5 The other 19 patients received CST from onset. CST was indicated for obstructive jaundice caused by distal bile duct stenosis, sclerosing cholangitis, and pancreatic pseudocyst.26 Prednisolone at an initial dose of 25–50 mg/day (30–40 mg in most cases) was administered for 2–4 weeks. It was then tapered by 5 mg every 2–4 weeks until reaching 5 mg/day, and 2.5–5 mg/day was continued as maintenance therapy.
After diagnosis, all patients were carefully followed, with particular attention being paid to the probability of the occurrence of AIP-related unfavourable events such as obstructive jaundice from distal bile duct stenosis, increased levels of biliary enzymes caused by sclerosing cholangitis confirmed on imaging findings, growing pancreatic pseudocyst, and others associated with extrapancreatic lesions,5 18 19–24 for which simple observation seemed very inadequate. Imaging studies (ultrasonography, computed tomography or magnetic resonance imaging) were performed every six months, and biochemical parameters were assessed every 3–6 months.
Differences were evaluated by Student’s t-test, Welch t-test or Fisher’s exact test. Cumulative event occurrence rate curves were analysed using the Kaplan–Meier technique with log-rank test. Possible predictors for unfavourable events included seven variables: age, gender, obstructive jaundice, abdominal pain, diffuse pancreatic ductal change, serum IgG4 levels, and CST. Age and serum IgG4 levels were transformed into categorical data consisting of two ordinal numbers by median values. Parameters that proved to have a low p value (<0.2) in the univariate analysis were tested by the stepwise multivariate Cox proportional hazards model. A p value of less than 0.05 was considered statistically significant. In the subgroup analysis (group with CST and group without CST), predictive factors for unfavourable events were examined by log-rank test because of the small number.
RESULTS
Patient profile
The detailed clinical profiles of 23 patients without CST (19 men and four women, average age 66 years) are shown in table 1. The mean follow-up was 61 months (range 11–162 months). The characteristics of 19 patients treated with CST from onset (16 men and three women, average age 64 years) are shown in table 2. The mean follow-up was 41 months (range 10–114 months), shorter than that of patients without CST (p = 0.031). There were 11 patients whose serum IgG4 was not measured at onset, but the serum IgG4 measured during follow-up was high (⩾135 mg/dl) in all of them. The clinical characteristics at onset of the 23 non-CST patients and the 19 CST patients are compared in table 3. Body weight loss (>5 kg in the past three months) was more frequently observed in CST than in non-CST patients (p<0.001). Patients with extrapancreatic lesions at onset were more frequent in the CST than in the non-CST group (p = 0.010).
Prognosis of patients without CST
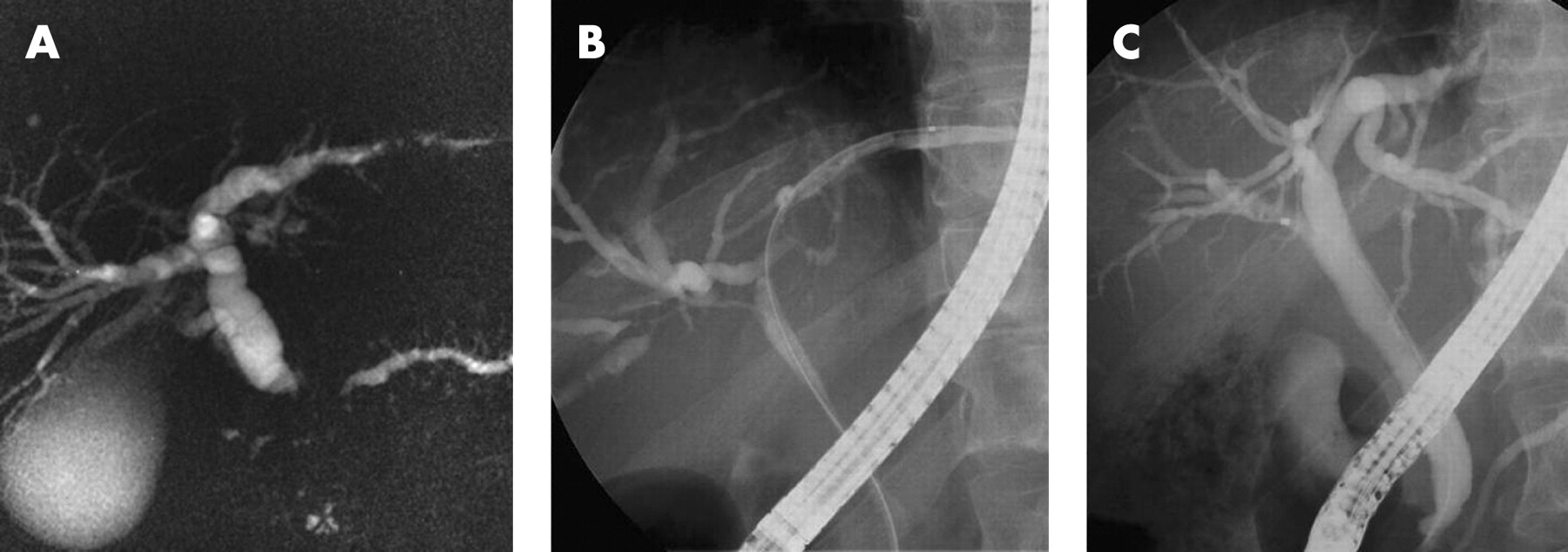
During follow-up, unfavourable events were observed in 16 out of 23 patients (70%) after 25 months on average (range 1–92 months) from onset. Among these 16 patients, sclerosing cholangitis was observed in nine, obstructive jaundice caused by distal bile duct stenosis in four, growing pseudocyst in one, hydronephrosis caused by retroperitoneal fibrosis in one, and interstitial nephritis in one. The nine sclerosing cholangitis cases were diagnosed at 30 months on average (median 12 months) after onset. Diagnosis was made during the periodic exchange of biliary plastic stents in five, and after their removal in four. We had one troublesome case for drainage therapy, in which multiple bile duct strictures appeared in a short period of just one month after the occurrence of distal bile duct obstruction, necessitating the use of multiple stents to control biliary infection (fig 1). The rate of event occurrence was 30.7% at one year and 49.6% at two years according to cumulative event occurrence rate curves.
Unfavourable events occurred in two of the three patients treated by pancreatectomy. One had re-occurrence of obstructive jaundice caused by swelling of the residual pancreas head (patient 9 in table 1), and the other had left hydronephrosis caused by retroperitoneal fibrosis (patient 16 in table 1).
Comparing the event-occurrence group with the event-free group, the ratio of patients with obstructive jaundice was significantly higher in the former group (table 4).
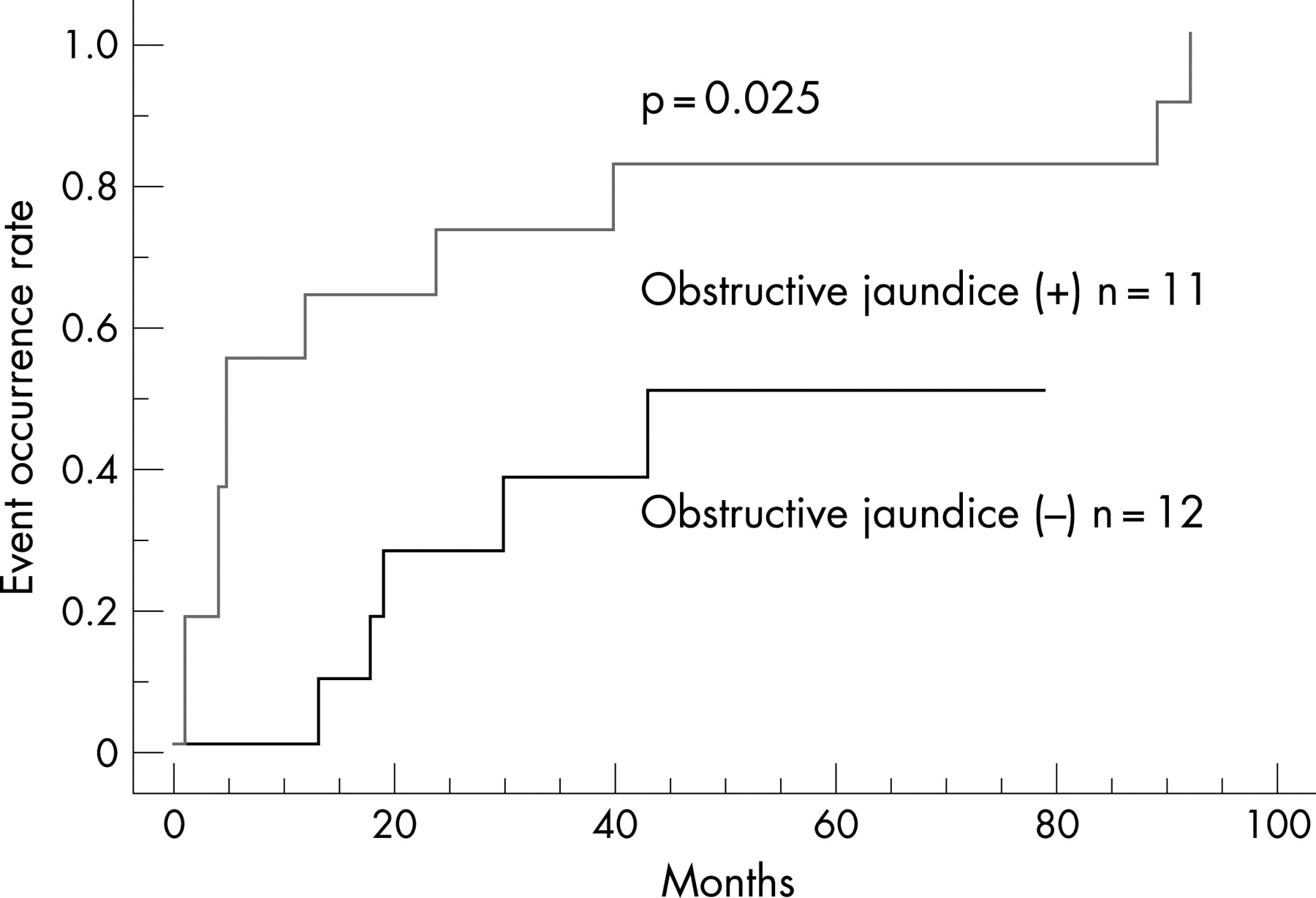
When patients were divided into two groups by age (⩾ median or < median), sex, obstructive jaundice, abdominal pain, diffuseness of pancreatic ductal change, and IgG4 levels at onset (⩾ median or < median, for the 15 patients with IgG4 measured at onset), patients with obstructive jaundice (p = 0.025) and abdominal pain (p = 0.013) had higher cumulative event occurrence rates (log-rank test). The cumulative event occurrence rate curves of patients with and without obstructive jaundice at onset are shown in figure 2.

{kind=link}
{kind=link}
Three patients died during follow-up. One died from cerebral infarction, one from lung cancer, and the other from pancreatic cancer. Judging from clinical symptoms, imaging findings and laboratory data, no patient developed liver cirrhosis or portal hypertension. Steatorrhea or emaciation suggestive of pancreatic insufficiency was not observed. Patients suffering from diabetes mellitus increased from five to seven.
Prognosis of patients treated with CST from onset
Imaging findings and laboratory data were improved in all cases four weeks after CST, as reported previously.5 9 10 During follow-up, unfavourable events occurred in six out of 19 patients(32%) at an average of 23 months (range 4–45 months) after CST (table 2). Two of the six patients had discontinued maintenance therapy. Three developed interstitial pneumonia and three obstructive jaundice caused by distal bile duct stenosis. Sclerosing cholangitis was not observed. The rate of event occurrence was 5.1% at one year and 19.6% at two years according to cumulative event occurrence rate curves.
No significant difference was noted between the event-occurrence and event-free groups in terms of age, sex, existence of obstructive jaundice and abdominal pain, pancreatic ductal change, IgG4, initial dose of prednisolone, and cessation of CST (table 5). Analysis by log-rank test revealed no significant risk factors for unfavourable events.
Among the 19 patients treated with CST, one patient had lumbar vertebra fracture and one had avascular necrosis of the femoral head during follow-up. These were possibly related to CST.
One patient died from acute myelocytic leukemia during follow-up. No patient developed liver cirrhosis or portal hypertension. Steatorrhea or emaciation suggestive of pancreatic insufficiency was not observed. Two patients discontinued maintenance therapy because of exacerbated diabetes mellitus, but an improvement in diabetes mellitus was not attained. Among eight patients diagnosed as having no diabetes mellitus at the initial evaluation, there was no new onset of diabetes mellitus except for these two patients.
Predictive factors for unfavourable events in AIP patients
Seven parameters were analysed to clarify the predictors of unfavourable events. Univariate analysis using the Cox proportional hazards model revealed no significant parameters, but obstructive jaundice at onset and CST had a comparatively low p value (<0.2). Stepwise multivariate analysis by the Cox proportional hazards model was performed using these two parameters. Results indicated that obstructive jaundice (p = 0.026) and CST (p = 0.029) retained significance as independent predictive factors (table 6).
DISCUSSION
CST has become accepted as a standard treatment for AIP. Because this disease was only recognised quite recently, however, its long-term prognosis is still obscure. In addition, some reports have suggested that patients can be treated without the use of CST.3 10 24 In this regard, CST carries the risk of a variety of adverse effects including susceptibility to infection, impaired glucose tolerance and osteoporosis. Therefore, it remains unclear whether CST is indispensable for all patients with AIP. With these issues in mind, we closely reviewed the outcome of AIP patients treated with and without CST in the present study.
The cumulative event occurrence rate was higher, especially in patients with obstructive jaundice or abdominal pain at onset when they did not receive CST. Obstructive jaundice remained as an only predictive factor after the analysis shown in table 6. The number of patients with abdominal pain in the non-CST group might be too small for a precise analysis.
All nine patients whose unfavourable event was sclerosing cholangitis had shown obstructive jaundice at onset, perhaps indicating that obstructive jaundice at onset is particularly related to the late occurrence of sclerosing cholangitis. Here, it is noteworthy that the late occurrence of sclerosing cholangitis was not observed in any of the CST-treated patients. As CST seems very effective, especially in preventing bile duct lesions, this treatment appears reasonable for patients with obstructive jaundice. As shown in fig 1, a particularly difficult condition is that of sclerosing cholangitis accompanied by biliary infection.
In patients treated with CST from the onset, unfavourable events were recognised in six (interstitial pneumonia and distal bile duct stenosis in three each). Because of the small number of unfavourable events, it was difficult to indicate significant risk factors. The cessation of CST may, however, have had a negative influence on prognosis, as both patients who discontinued CST suffered from late unfavourable events (interstitial pneumonia and distal bile duct stenosis in one each; table 2). An issue requiring further investigation will be the optimal duration of maintenance therapy, as continued CST may reduce AIP-related unfavourable events but may also increase the risk of CST-induced adverse events.
The late occurrence of interstitial pneumonia was remarkable in patients treated with CST. Although this condition was improved by increased prednisolone, a higher dose was necessary to maintain remission than for biliary involvement.24 CST may be less preventive of interstitial pneumonia.
Whether asymptomatic patients, most of whom present with localised pancreatic changes and are free of obstructive jaundice, should be treated with CST or not is a question that might be answered only after a long observation period. The late occurrence of obstructive jaundice as a result of aggravated residual pancreas swelling was observed in one patient even after distal pancreatectomy. This might imply the gradual progression of pancreatic lesions leading to severe symptoms in presently asymptomatic patients. In addition, there is a possibility of extrapancreatic lesions appearing during long-term follow-up without CST.10 Furthermore, the potentially beneficial effect of CST on pancreatic endocrine and exocrine function should also be taken into account.19 27 28 Taken together then, observation may be acceptable for asymptomatic patients in consideration of their lower incidence of unfavourable events for now (fig 2), but this issue must be revisited in the near future.
It is unknown whether high serum IgG4 is related to prognosis, although its elevation is the most characteristic feature in AIP.13 14 As we previously reported cases in which IgG4 increased at the time of the later occurrence of interstitial pneumonia,24 we expected that serum IgG4 levels were related to the prognosis of AIP. In our series, however, serum IgG4 levels at onset showed no correlation with prognosis. Although changes in IgG4 levels may give clinically useful information, singly tested IgG4 levels are not likely to be sufficiently informative for the prediction of severity or prognosis.
The major weak point of this study was that it was not a randomised controlled trial. There were background differences between patients with and without CST. Considering that AIP is still a rare disease without a long history, however, planning a randomised controlled trial several years ago would have been difficult.
In conclusion, CST could reduce AIP-related unfavourable events. The early introduction of CST is recommended especially for patients accompanied by obstructive jaundice in order to prevent the late occurrence of complicated sclerosing cholangitis.
REFERENCES
Footnotes
Conflict of interest: None declared.
- Abbreviations:
- AIP
- autoimmune pancreatitis
- CST
- corticosteroid treatment