Article Text

Abstract
Background The combined effect of resting heart rate (RHR) and physical activity (PA) on ischaemic heart disease (IHD) has never been assessed. The objective of this study was to assess the association of RHR with IHD mortality, and to evaluate the potentially modifying effect of PA on this association.
Methods In a prospective cohort study of 24 999 men and 25 089 women free from cardiovascular disease at baseline, Cox proportional hazard models were used to estimate adjusted hazard ratios of death from IHD related to RHR measured at baseline. The combined effect of RHR and self-reported PA on the risk of death from IHD was also assessed.
Results During a mean of 18.2 (SD 4) years of follow-up, 2566 men and 1814 women died from cardiovascular causes. For each increment of 10 heart beats per minute, risk of death from IHD was 18% higher in women <70 years of age (p<0.001); no such association was observed among women ≥70 years. Among men, there was a corresponding 10% higher risk in the younger (p = 0.004), and 11% higher risk in the older age group (p = 0.01). Among women, the risk associated with high RHR was substantially attenuated in those who reported a high level of PA, whereas in men, there was no clear indication that PA could modify the positive effect of RHR.
Conclusion RHR is positively associated with the risk of death from IHD, and among women, the results suggest that by engaging in PA, the risk associated with a high RHR may be substantially reduced.
Statistics from Altmetric.com
Heart rate is a well recognised and accessible clinical parameter. Recent reviews1–4 and previous epidemiological studies have shown a strong positive association of resting heart rate (RHR) with cardiovascular mortality, both in the general population5–8 and in subgroups of patients (patients with hypertension, patients with suspected or proven coronary heart disease, patients with metabolic syndrome, and in studies of the elderly).9–15
RHR is affected by numerous factors, including but not limited to drugs, diet, psychological status, physical fitness, and the interaction of genetics and the environment.4 Physical activity (PA) is a consistent and robust indicator associated with good health and low mortality, and cardiovascular disease prevention by means of PA is highly recommended.16–18 Indeed, high levels of PA significantly reduce the RHR, and it has also been suggested that physically active people have lower levels of cardiovascular risk factors, and lower risk of cardiovascular events.18–21
However, it is not known if RHR and PA may have a combined effect on cardiovascular mortality. Previous studies have not combined information of RHR and PA in the analyses, and it remains uncertain if the positive association of RHR with cardiovascular deaths (CVDs) could be influenced by levels of PA.
Therefore, the aim of the present study was to prospectively assess the association of RHR with cardiovascular mortality, and, specifically, to evaluate the potentially modifying effect of PA on this association.
Materials and methods
Study population
Between 1984 and 1986, the total adult population of 20 years and older in Nord Trøndelag County in Norway was invited to participate in a health survey (the HUNT study). A total of 75 043 (88.2%) out of 85 100 eligible individuals accepted the invitation. Respondents filled in the questionnaire that was included with the invitation, and attended a clinical examination where they received a second questionnaire that was to be filled in and returned from home in a pre-stamped envelope. Briefly, information was collected on a range of health and lifestyle-related topics, and included past and present smoking, alcohol consumption, educational attainment, marital status, self-reported PA, and among other items, the clinical examination included standardised measurements of RHR, blood pressure, diabetes status (non-fasting glucose), body height and body weight.
Heart rate
After at least 4 min of rest in sitting position, heart rate was measured by palpating the radial pulse over a period of 15 s with a stop watch. If the pulse was irregular or difficult to count, the test was extended to 30 s, if necessary with the aid of a stethoscope placed over the heart.
Physical activity
The recreational PA questionnaire included exercise frequency, intensity and duration. The participants were asked about their average frequency of physical exercise in a week, with five response options (0, <1, 1, 2–3, ≥4 times; coded 1–5). Those who reported exercising once a week or more were also asked about the average duration (four categories: <15, 15–30, 30–60, >60 min; coded 1–4) and intensity (three categories: light, moderate, vigorous; coded 1–3) of the activity. These three questions on PA have been shown to provide a reproducible measure of leisure-time PA and found to correlate with measured oxygen uptake and heart rate.18 22
To assess the effect of total exercise volume, a summary score was constructed combining information on frequency, duration and intensity. The score was calculated for those who exercised once a week or more, and thus had answered the questions on duration and intensity. To give equal weight to each measure of activity, the score was constructed according to the following equation: 1/5 × Frequency + 1/4 × Duration + 1/3 × Intensity. Due to the classification and coding of the response options in the questionnaire, this approach gave a maximum score of 1.0 for each of the three components of the summary score. The median score value was 2.02 for men and 1.83 for women (range 1.18–3.00). A summary score below the median was classified as low activity, whereas a score at the median or above was classified as high activity. This summary score has been used in previous studies from the same population; both in relation to risk of cancer23 and mortality from CVDs associated with metabolic clustering.24 The properties of an approximately similar measure of exercise volume were assessed in a validation of the PA questions and found to perform well.22
Exclusions
The aim of this study was to follow-up people with no apparent sign of cardiovascular disease at baseline. Based on self-reports, 6878 participants were excluded who had a history of myocardial infarction or known angina pectoris, as well as those with a history of stroke or prevalent diabetes mellitus. Also, 6964 participants were excluded who were either current or past users of blood pressure medication. In addition, 121 participants with missing information on RHR, and 307 participants for whom height and weight measurements were missing were excluded. Information on PA was collected in the second questionnaire that was to be returned from home. A total of 10 685 persons failed to return the second questionnaire, and were therefore excluded from the analysis. This left 50 088 participants (24 999 men, and 25 089 women), who were followed up for cause-specific mortality.
Ascertainment of outcomes
The mandatory reporting of deaths by physicians and public health officers to the National Cause of Death Registry in Norway is the basis for coding underlying causes of death. Mortality follow-up to the Cause of Death Registry is virtually complete, and in this study, the primary endpoint was cardiovascular deaths (International Classification of Disease (ICD) 9: 390–459; ICD 10: I 00–I 99). Specific emphasis was given to deaths from ischaemic heart disease (ICD 9: 410–414; ICD 10: I 20–I 25). The mortality follow-up of the HUNT cohort was approved by the regional committee for ethics in medical research and by the Norwegian Data Inspectorate.
Statistical analysis
Person-years were calculated from the date of attendance to the clinical examination at baseline (1984–6) until death, or until the end of follow-up, 31 December 2004, whichever came first. Heart rate was divided into quintiles: first (≤60 beats per minute (bpm)), second (61–72 bpm), third (73–87 bpm), fourth (88–100 bpm) and fifth (≥101 bpm). A heart rate below 60 bpm is widely referred to as sinus bradycardia and in the absence of electrocardiogram recordings, the second quintile (61–72 bpm) of heart rate is used as the reference group in the analyses, as previously recommended.25 Cox regression analyses were used to compute hazard ratios (HR) of CVDs, and specifically, deaths from ischaemic heart disease, where the rate of death of people within a specified heart rate quintile was compared with the rate in the reference group. Precision of the estimates was assessed by 95% confidence intervals (CI). The basic models were age-adjusted using attained age as the time variable. Adjustments were made for body mass index (<18.5, 18.5–24.9, 25.0–29.9, ≥30.0 kg/m2), PA score categories (no activity, <1 per week, low summary score and high summary score), smoking status (never, former, current and unknown), use of alcohol (frequency last 2 weeks: 0, 1–4, ≥5, total abstainer and unknown), marital status (married, unmarried, widowed and divorced/separated) and education (<10, 10–12, ≥13 years and unknown). Departure from the proportional hazards assumption was evaluated by Schoenfeld residuals, and there was no evidence of departure. The association with deaths caused by ischaemic heart disease per increment of 10 bpm was also examined, and the interactions between heart rate or change in heart rate quintile and ischaemic heart disease by sex and age were assessed; p values were calculated by likelihood ratio tests comparing models with and without the interaction terms. Similarly, the rate of death among participants was calculated within a given category of PA score (no activity, <1 per week, low summary score) compared with the rate of death in the reference category of high summary score.
In a separate analysis, the combined effect of RHR and PA were assessed on the risk of deaths from ischaemic heart disease. For this purpose, heart rate was divided into four categories, ie ≤60 bpm, 61–73 bpm, 74–87 bpm and ≥88 bpm, and PA summary score categories were used. In the combined analysis, participants who had a heart rate of 61–73 bpm and simultaneously reported high PA served as the reference group. In the analysis, rates of death from ischaemic heart disease in combinations of heart rate and PA were compared to the rate in the reference group.
The potential influence of preclinical disease was evaluated at baseline by excluding cases that occurred during the first 5 years of follow-up. All statistical tests were two-sided, and the statistical analyses were conducted using Stata for Windows (Version 10.0 StataCorp LP, 1985–2007).
Results
Baseline characteristics of the study population are presented in table 1. During 18 years of follow-up (approximately 1 000 000 person-years), a total of 10 475 people died (6033 men and 4442 women). Cardiovascular disease caused 4380 of the deaths (2566 (58.6%) men and 1814 (41.4%) women). In men, 1419 deaths (55.3%) were attributed to ischaemic heart disease and 552 (21.5%) to stroke. Among women, 718 (39.6%) died from ischaemic heart disease and 587 (32.4%) from stroke.
Characteristics of study population
Heart rate levels and cardiovascular mortality
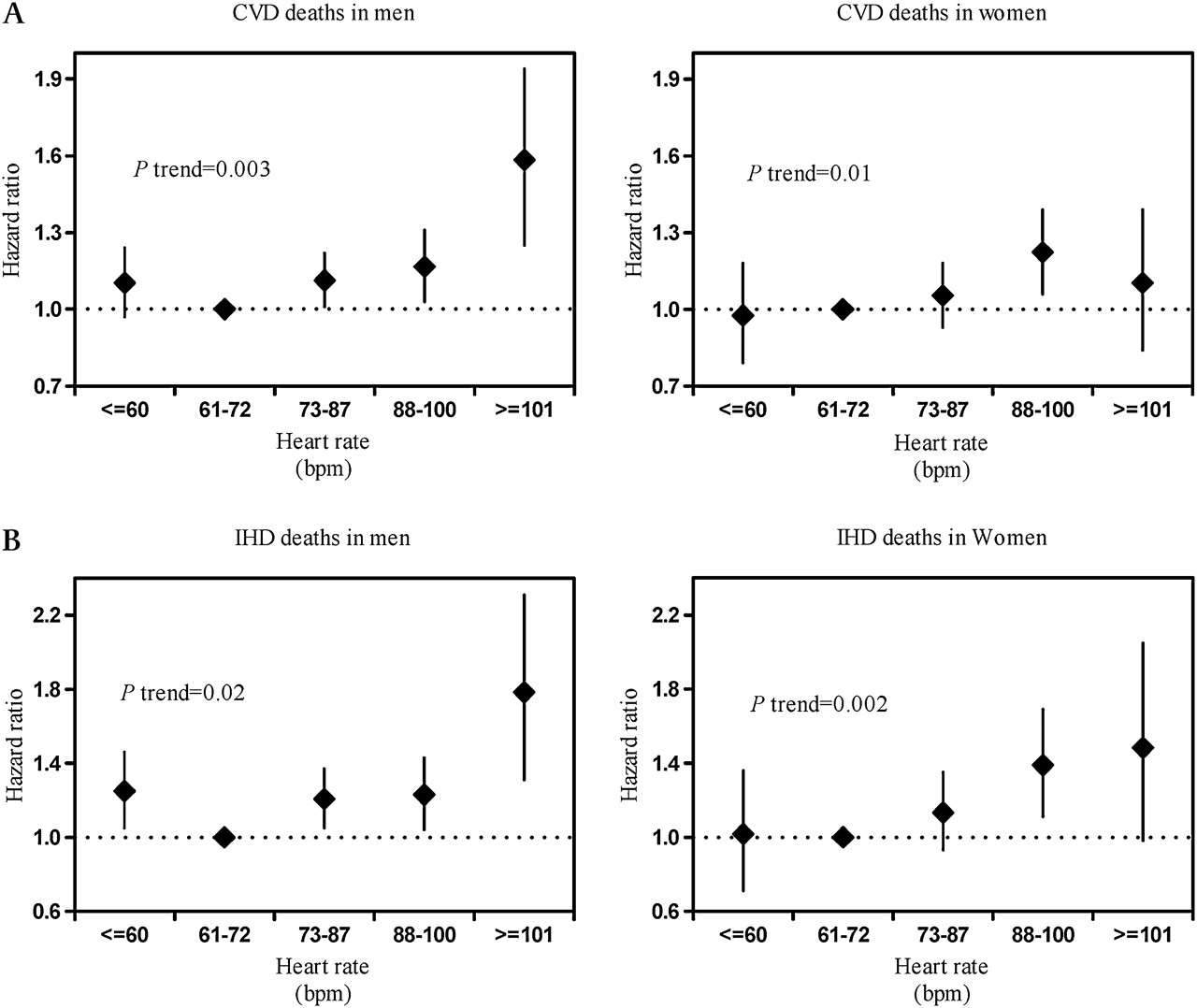
Resting heart rate was positively associated with the risk of CVD in men, showing a gradual increase in mortality with increasing RHR (p for trend, 0.003), as shown in figure 1 (panel A). Among men in the highest quintile (≥101 bpm), the adjusted hazard ratio of CVD was 1.56 (CI 1.25 to 1.94), compared to men in the reference group (61–72 bpm). Among women, there was a weak but not consistent positive association of heart rate with cardiovascular mortality. Compared to the reference, the adjusted hazard ratio associated with a heart rate of 88–100 bpm was 1.22 (CI 1.06 to 1.39), whereas the hazard ratio for women in the highest quintile was 1.08 (CI 0.84 to 1.39) (fig. 1, panel A).
{kind=link}
Hazard ratio of death from cardiovascular disease (panel A) and from ischaemic heart disease (panel B) among men and women associated with quintiles of resting heart rate. Adjusted for age (continuous), body mass index (<18.5, 18.5–24.9, 25.0–29.9, >30 kg/m2), physical activity index (high score, low score, <1 per week, no activity), marital status (married, unmarried, widow(er), divorced/separated), education (<10, 10–12, ≥13 years and unknown), alcohol consumption (frequency last 2 weeks: 0, 1–4, ≥5, total abstainer and unknown), and smoking status (never, former, current and unknown). Participants in the second quintile of heart rate served as the referent. Heart rate quintiles: First (≤60 bpm), second (61–72 bpm), third (73–87 bpm), fourth (88–100 bpm) and fifth (≥101 bpm). Diamonds represent risk estimates, and bars represent 95% confidence intervals.
The associations of RHR with deaths from ischaemic heart disease were stronger than for CVDs as a whole, both in men and women (p trend, 0.02 for men and 0.002 for women). The adjusted hazard ratio associated with a heart rate of 101 bpm and higher was 1.73 (CI 1.31 to 2.31) for men, and 1.42 (CI 0.98 to 2.05) for women, compared to the reference group (61–72 bpm) (fig 1, panel B).
Age-specific effects of RHR with cardiovascular mortality were studied, showing an effect modification by age at a cutoff of 70 years, and also tested for interaction with age. Among men, the association (including deaths from ischaemic heart disease) did not substantially differ between age groups. Among women, however, the effects were strongly dependent on age, especially for deaths due to ischaemic heart disease (p value for interaction, 0.01), showing a positive association in women younger than 70 years at baseline, and no association in women 70 years and older (table 2). Thus, in the younger age group, the adjusted hazard ratio associated with a heart rate ≥101 bpm was 2.11 (CI 1.28 to 3.46), compared to the reference group, and the corresponding hazard ratio in the older age group was 0.95 (CI 0.55 to 1.65). In men, the corresponding age specific hazard ratios were 1.67 (CI 1.17 to 2.38) in the younger (<70 years) and 1.84 (CI 1.15 to 2.96) in the older (≥70 years) age group.
Hazard ratio (HR) of death from ischaemic heart disease (IHD) among Norwegian men and women, by heart rate at baseline
In the absence of electrocardiogram recordings, people with possible arrhythmias could not be excluded, eg sinus bradycardia that could affect the association of RHR with cardiovascular mortality; a strong rational for choosing second quintile as referent. Among men, the risk of death from ischaemic heart disease was slightly higher in the RHR category ≤60 bpm; showing a HR of 1.23 (CI 1.00 to 1.52) among those younger than 70 years at baseline, and 1.27 (CI 0.95 to 1.69) in older men.
In a separate analysis, heart rate was used as a continuous variable, and excluded people with heart rate ≤60 bpm. For each increment of 10 bpm, there was 18% higher risk of death from ischaemic heart disease in women younger than 70 years (p<0.001), and no such association was observed among women 70 years or older. Among men, there was a corresponding 10% higher risk in the younger (p = 0.004), and 11% higher risk in the older group (p = 0.01).
Physical activity and cardiovascular mortality
The association of PA with the risk of dying from cardiovascular causes, and specifically, from ischaemic heart disease, is presented in table 3. People who reported no PA were at consistently higher risk of CVD than people who reported <1 per week, low or high levels of PA. Among men, the adjusted HR associated with no activity was 1.22 (CI 1.08 to 1.38) for total CVDs, and 1.18 (CI 1.00 to 1.40) for ischaemic heart disease, compared to men who reported high PA. The corresponding HR in women were 1.32 (CI 1.15 to 1.52) for cardiovascular disease overall, and 1.39 (CI 1.12 to 1.73) for ischaemic heart disease.
Level of physical activity (PA) in men and women and hazard ratio (HR) of cardiovascular death (CVD), and specifically, deaths from ischaemic heart disease (IHD)
Combined effect of RHR and PA
The RHR was lower in men who reported high PA compared to men with no activity (69 (SD 12) bpm vs 76 (SD 13) bpm, respectively; p<0.001). Likewise, women who were highly active had lower RHR than women who reported no activity (74 (SD 12) bpm vs 78 (SD 12) bpm, respectively; p<0.001) (data not shown).
The adjusted hazard ratios among men for the combined effects of RHR and PA on deaths from ischaemic heart disease are shown in table 4. Compared to the reference group of men who reported high PA and had a heart rate of 61–73 bpm, the adjusted hazard ratios associated with a heart rate of ≥88 bpm were 1.94 (CI 1.45 to 2.59) for active men and 1.37 (CI 1.00 to 1.89) for inactive men.
Adjusted* hazard ratios (HR) of death from ischaemic heart disease in combined categories of heart rate and physical activity among Norwegian men
Among women, the combined analyses showed that at every level of RHR, women who reported high PA were at lower risk of death from ischaemic heart disease compared to women with no PA (table 5). Irrespective of RHR, women who reported high PA appeared to have an advantage over those who were inactive. Compared to the reference group of active women with a heart rate of 61–73 bpm, the adjusted HR of death from ischaemic heart disease associated with a heart rate ≥88 bpm were 2.10 (CI 1.43 to 3.07) for inactive women, and 1.37 (CI 0.89 to 2.12) for women who reported high PA.
Adjusted* hazard ratios (HR) of death from ischaemic heart disease in combined categories of heart rate and physical activity among Norwegian women
Discussion
Principal findings
In this large prospective study of men and women without cardiovascular disease at baseline, a strong, positive association of RHR with risk of CVD was found. The higher risk was particularly striking for deaths caused by ischaemic heart disease in women younger than 70 years at baseline. It was also found that the risk associated with a high RHR was substantially attenuated among women who reported a high level of PA, suggesting that by engaging in PA, women with a high RHR could reduce their risk of cardiovascular disease.
The present results contribute to extend the literature on the epidemiology of cardiovascular disease among women, as previously, data among women have been sparse, except for one large cohort study of post-menopausal women showing that RHR is an independent predictor of coronary events.5 To the authors' knowledge, this is the first study to account the combined effect of RHR and PA on deaths from ischaemic heart disease in a population that was reported to be free from cardiovascular disease at baseline.
Strengths and limitations
The strengths of this study include large size, diversity of cohort, long follow-up and detailed information on potentially confounding factors, which allow assessment of the combined effect of RHR and PA on the risk of dying from ischaemic heart disease. A clear limitation, however, is that heart rate was measured at only one occasion. Information on PA was self-reported and quite crude, and misclassification due to subjective interpretation of the questions and individual perception of the activity could have influenced the estimated effects of PA. Furthermore, other issues like recall bias cannot be ignored, especially in elderly and social desirability bias where the participants could tend to report high volumes of PA that would be viewed favourably by others. Also, there is no information about occupational activity levels, thus this was not adjusted in the analysis. In prospective studies, however, the nature of the misclassification of such factors is most likely non-differential in relation to future disease, and therefore, likely to yield underestimates of the true effects. Moreover, validation studies have shown that questionnaires may be useful in classifying people into broad categories of PA (eg high, moderate or low active), but less appropriate for quantifying energy expenditure.26
It is possible that preclinical disease can influence both RHR and the participant's response to the PA questions. To reduce this possibility, the first 5 years of follow-up were excluded, but the results were essentially identical. Other unmeasured or unknown factors could also have confounded the estimates of effect. Thus, it cannot be excluded that adjustment for such factors could have influenced the results. For example, lipoprotein sub-fractions related to heart rate and to coronary heart disease,27 and thyroid hormone function that affects RHR,28 and appears to be associated with cardiovascular mortality, could be important, but information on these factors was not available in this study.
The RHR and blood pressure could act on the same causal pathway towards cardiovascular disease. In the primary analyses, therefore blood pressure was not taken into account, but in a separate analysis, with blood pressure included as possible mediating factor, the effect of RHR was attenuated, suggesting that the effect could be partly mediated by blood pressure.
Relation to other studies
The present findings suggest stronger associations of RHR with deaths from ischaemic heart disease than for CVDs as a whole, for reasons that have been extensively discussed.1–4 This observation is also in line with a direct effect of RHR on the outcome of patients with ischaemic heart disease, resulting in decreased events with reduction in RHR.9 Furthermore, tachycardia is largely a physiological compensatory response in heart failure, and this effect appears to be beneficial only up to a certain level, after which it may be a marker for increased neuroendocrine activation.29
The present results in men are consistent with previous reports in showing that RHR is positively associated with cardiovascular mortality both at younger7 8 and older ages.14 Among the few previous studies of elderly women, some have reported a strong positive association of RHR with cardiovascular mortality,11 12 whereas others reported no clear association.5 7 8 In the present study, there was a stronger association in women younger than 70 years at baseline, and this effect could be caused by deaths at a relatively young age in women who were particularly vulnerable to a high RHR. Thus, a “selective survival” effect, dependent on heart rate, could be one plausible explanation for the particular effect related to age. Another possibility could be that prevalent cardiovascular risk factors may be less likely to be detected in the younger age group. If these risk factors are associated with higher RHR, the failure to detect early clinical signs of cardiovascular disease could have contributed to the stronger association with deaths from ischaemic heart disease in women younger than 70 years.30 Moreover, chronotropic insufficiency is more frequent in the older women, which could affect the association of RHR with ischaemic heart disease mortality. However, the present findings in men are not compatible with these possible explanations, and future studies need to address that the association of RHR with premature CVD may differ, related to both age and sex.
It was found that the mortality from ischaemic heart disease associated with a high RHR was substantially attenuated among women who reported a high level of PA, suggesting that by being physically active, women with a high RHR could avoid cardiovascular complications. Experimental studies have repeatedly shown that PA reduces the RHR of healthy individuals,19 20 by improving the sympathetic and parasympathetic balance, suggesting that exercise-induced enhanced vagal modulation may reduce the risk of arrhythmias and sudden death.31 In men with high PA, the association of high RHR with deaths from ischaemic heart disease was not attenuated in this study. It can only be speculated what the reasons are for the different results in men and women. A possible explanation could be that men, more so than women, tend to overestimate their level of PA,32 and this, in turn, could have influenced the results. Future studies are warranted to investigate the association of RHR and PA to assess the combination of intensity and volumes to have an optimal influence on IHD mortality.
Conclusion
To summarise, RHR was positively associated with risk of CVDs and particularly, with deaths caused by ischaemic heart disease. Especially among women, there was also evidence for a combined effect of RHR and PA, suggesting that by engaging in PA, the risk associated with a high RHR may be substantially reduced, but PA alone does not fully explain the association of RHR with IHD deaths.
What is already known on this subject
Resting heart rate is positively associated with ischaemic outcomes in a disease-free population.
High physical activity is associated with low mortality.
Combined effect of resting heart rate and physical activity is uncertain and has never been assessed.
What this study adds
Much clearer positive association of resting heart rate with ischaemic outcomes in women younger than 70 years.
High physical activity attenuates the positive association of resting heart rate with ischaemic events among women, but not in men.
Physical activity may be used as a non-invasive and non-pharmacological method for heart rate lowering treatment in disease-free population.
Acknowledgments
Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between HUNT Research Centre (Faculty of Medicine, Norwegian University of Science and technology NTNU), Nord-Trøndelag County Council and the Norwegian Institute of Public Health. We are indebted to the participants of the HUNT Study and to the management of the study for using these data.
References
Footnotes
Funding The present study was supported by grants from the Norwegian Council of Cardiovascular Disease, the Norwegian Research Council (Funding for Outstanding Young Investigators, UW), Funds for Cardiovascular and Medical Research at St. Olav's University Hospital, Trondheim, and the Torstein Erbo's Foundation, Trondheim. Role of the funding source: The funding organisations had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript.
Competing interests None.
Ethics approval Regional committee for ethics in medical research and by the Norwegian Data Inspectorate.
Provenance and peer review Not commissioned; not externally peer reviewed.