


Abstract
Background: The cytochrome P450 3A4 (CYP3A4) inhibitor clarithromycin may also inhibit liver-specific organic anion–transporting polypeptides (OATP1B1 and OATP1B3). We studied whether concurrent use of clarithromycin and a statin not metabolized by CYP3A4 was associated with an increased frequency of serious adverse events.
Methods: Using large health care databases, we studied a population-based cohort of older adults (mean age 74 years) who were taking a statin not metabolized by CYP3A4 (rosuvastatin [76% of prescriptions], pravastatin [21%] or fluvastatin [3%]) between 2002 and 2013 and were newly prescribed clarithromycin (n = 51 523) or azithromycin (n = 52 518), the latter an antibiotic that inhibits neither CYP3A4 nor OATP1B1 and OATP1B3. Outcomes were hospital admission with a diagnostic code for rhabdomyolysis, acute kidney injury or hyperkalemia, and all-cause mortality. All outcomes were assessed within 30 days after co-prescription.
Results: Compared with the control group, patients co-prescribed clarithromycin and a statin not metabolized by CYP3A4 were at increased risk of hospital admission with acute kidney injury (adjusted relative risk [RR] 1.65, 95% confidence interval [CI] 1.31 to 2.09), admission with hyperkalemia (adjusted RR 2.17, 95% CI 1.22 to 3.86) and all-cause mortality (adjusted RR 1.43, 95% CI 1.15 to 1.76). The adjusted RR for admission with rhabdomyolysis was 2.27 (95% CI 0.86 to 5.96). The absolute increase in risk for each outcome was small and likely below 1%, even after we considered the insensitivity of some hospital database codes.
Interpretation: Among older adults taking a statin not metabolized by CYP3A4, co-prescription of clarithromycin versus azithromycin was associated with a modest but statistically significant increase in the 30-day absolute risk of adverse outcomes.
See also commentary on page 163 and at www.cmaj.ca/lookup/doi/10.1503/cmaj.150030
Statins may soon be recommended for more than a billion people worldwide.1 Although past clinical trials have generally proven statins to be safe,2 a 2012 Internet-based survey suggested that almost one-third of statin users experience adverse effects.3 In a small number of individuals, statin use has been associated with serious effects, including rhabdomyolysis, acute kidney injury, hyperkalemia and death.4–6 The risk of statin toxicity increases with higher blood statin concentrations, which can arise when concurrent medications alter the pharmacokinetics of statins.7 Traditional pharmacokinetic models attribute this increase to the inhibition of the drug-metabolizing enzyme cytochrome P450 3A4 (CYP3A4).
More recent evidence supports an additional cause that involves reduced drug transporter–mediated hepatic uptake of statins.8–13 For example, several haplotypes of commonly occurring genetic polymorphisms in the liver-specific organic anion–transporting polypeptide 1B1 (OATP1B1) were associated with increased blood concentrations of the non–CYP3A4-metabolized statins rosuvastatin and pravastatin in humans.13–16 Clarithromycin has been shown to inhibit OATP1B1 and OATP1B3 in hepatocyte cell cultures.10 However, we found no data to show the effect of clarithromycin on the clinical pharmacokinetics of rosuvastatin, pravastatin and fluvastatin.
All of these findings provided us with the opportunity to investigate the interaction between clarithromycin and statins not metabolized by CYP3A4 in the context of frequency of serious adverse events.17 We compared the risk of statin-associated adverse events (rhabdomyolysis, acute kidney injury, hyperkalemia and death) when rosuvastatin, pravastatin or fluvastatin is co-prescribed with clarithromycin (a macrolide antibiotic and inhibitor of OATPs18–20) versus azithromycin (a macrolide antibiotic that does not inhibit OATPs10).
Methods
Study design and setting
We conducted a population-based, retrospective cohort study at the Institute for Clinical Evaluative Sciences (ICES) according to an established protocol approved by the Research Ethics Board at the Sunnybrook Health Sciences Centre (Toronto, Canada). Data on adults 66 years of age and older between June 2002 and March 2013 were obtained and analyzed through linked health care databases in the province of Ontario. The province has about 13.6 million residents, 16% of whom are 65 years or older and have universal coverage for prescription drugs.21 We followed guidelines for observational studies for the reporting of this study.22
Data sources
We ascertained patient characteristics, drug use, covariate information and outcome data using records from 5 large administrative databases housed at ICES. The Ontario Registered Persons Database contains demographic and vital status information for all residents of the province who have ever been issued a health card. We used the database of the Ontario Drug Benefit Program to identify prescription drug use. The database contains accurate records (error rate < 1%) for all outpatient prescriptions dispensed to people 65 years or older.23 We obtained detailed diagnostic and procedural information on all hospital admissions in the province, including up to 25 unique diagnostic codes assigned per admission, from the Canadian Institute for Health Information’s Discharge Abstract Database. We collected covariate information from the Ontario Health Insurance Plan (OHIP) database. This database includes fee-for-service health claims for inpatient and outpatient physician services. Finally, we obtained information on antibiotic prescribers from the ICES Physician Database, which comprises data from the Corporate Provider Database, the Ontario Physician Human Resource Data Centre database and the OHIP database of physician billings. All of the data were linked anonymously with the use of encrypted health card numbers, a method that has been used previously for studies on adverse drug events, health outcomes and health services.24–29
All variables used in this study were complete except for neighbourhood income (missing for 0.25% of patients) and prescriber specialty (missing for 13.21%). We used the International Classification of Diseases, 9th revision (ICD-9) codes before April 2002 and ICD-10 codes after Apr. 1, 2002, to assess baseline comorbidities in the 5 years before the co-prescriptions (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.140950/-/DC1). We used ICD-10 codes to ascertain outcomes (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.140950/-/DC1), because all events would have occurred after the implementation of this coding system.
Study population
Our cohort comprised all older adults in Ontario who had continuous prescriptions for statins not metabolized by CYP3A4 (study statins: rosuvastatin, fluvastatin and pravastatin) and who received a co-prescription for either clarithromycin or azithromycin (control group) between June 2002 and March 2013. Azithromycin is an antibiotic with indications similar to those of clarithromycin, but it does not substantially inhibit CYP3A4 or OATP1B1 and OATP1B3.10,30,31 In a previous study of provincial data, we showed that clarithromycin and azithromycin have similar indications, clinical use patterns and rates of adverse events when used independently.32 Thus, we felt that the comparison of outcomes among older adults prescribed these antibiotics would serve as a useful model for studying drug interactions in routine clinical practice.
The date of the first co-prescription of a study antibiotic served as the index date. We confirmed that all patients in the study were continuously taking a study statin (≥ 2 prescriptions in the 210 days before the index date) and that the most recent statin prescription covered the index date. This ensured that a study statin and macrolide antibiotic were co-prescribed.
We excluded patients if they met any of the following criteria: (a) they were in their first year of eligibility for provincial coverage of prescription drugs (aged 65 years), to avoid incomplete medication records; (b) they received a prescription for more than one type of antibiotic or statin on the index date, to compare mutually exclusive groups; (c) they received any antibiotic in the 30 days before the index date, to ensure new antibiotic use and to exclude patients with severe infections that failed to respond to initial antibiotic treatment; (d) they had one or more prescriptions for a non-study statin (including CYP3A4-metabolized statins) in the 180 days before antibiotic prescription, to ensure that any observed adverse events were associated with the study drugs; (e) they were discharged from hospital in the 2 days before their index date, to ensure inclusion of new outpatient antibiotic prescriptions (in Ontario, patients continuing antibiotic treatment started in hospital have their outpatient antibiotic prescription dispensed on the same day or the day after discharge); or (f) they had a prescription for a potent CYP3A4 inhibitor (protease inhibitor, chloramphenicol or antifungal) dispensed in the 6 months before the index date, to exclude drugs that are often also potent inhibitors of OATPs.33,34
A patient could be entered into the cohort only once. We restricted analysis to the first prescription of a study antibiotic that the patient received in follow-up (subsequent prescriptions were not considered).
Outcome measures
We followed patients for 30 days after the index date to assess outcomes. We examined the 4 outcomes specified in a previous study of statin toxicity from drug interactions:24 hospital admission because of rhabdomyolysis, admission because of acute kidney injury, admission because of hyperkalemia, and all-cause mortality (the diagnostic codes are shown in Appendix 2). Patients with multiple hospital admission codes were accounted for in the assessment of each type of admission.
In Ontario, we have previously observed that a hospital diagnostic code for rhabdomyolysis identifies patients with a median peak creatine kinase level of 1835 (interquartile range [IQR] 680 to 3986) U/L, whereas the absence of such a code indicates patients without a creatine kinase level or with a measured median level of 130 (IQR 60 to 368) U/L (unpublished data). Similarly, a hospital diagnostic code for acute kidney injury identifies a median absolute increase in serum creatinine of 98 (IQR 43 to 200) μmol/L from the most recent value before admission, and the absence of such a code represents a median increase of 6 (IQR −4 to 20) μmol/L.35 A code for hyperkalemia identifies a median serum potassium concentration of 6.0 (IQR 5.1 to 6.7) mmol/L, and its absence defines a median concentration of 4.1 (IQR 3.8 to 4.5) mmol/L.36 These validation studies showed a spectrum bias in coding: as a condition becomes more extreme, a code is more likely to be present for that diagnosis. The overall incidence is therefore underestimated, particularly for milder forms of the conditions. For example, the incidence of acute kidney injury can be underestimated up to five-fold when assessed by diagnostic code, as compared with laboratory values.35
Statistical analysis
We compared baseline characteristics between statin users co-prescribed clarithromycin and those co-prescribed azithromycin using standardized differences.37,38 This metric describes differences between group means relative to the pooled standard deviation and is considered a clinically meaningful difference if greater than 10%. We expressed the risk of an outcome in both relative and absolute terms, and we used multivariable logistic regression analyses to estimate odds ratios and 95% confidence intervals (95% CIs). We adjusted for 15 potential confounding variables based on clinical relevance: age, sex, year of cohort entry; baseline evidence of chronic kidney disease, stroke or transient ischemic attack, peripheral vascular disease, coronary artery disease, congestive heart failure, major cancer and diabetes; baseline use, in the 120 days before the index date, of β-blockers, calcium-channel blockers, diuretics, angiotensin-converting-enzyme inhibitors or angiotensin II receptor blockers, and nonsteroidal anti-inflammatory drugs.
In all outcome analyses, we interpreted 2-tailed p values of less than 0.05 as statistically significant. We interpreted odds ratios as relative risks (RR; appropriate given the incidences observed). We conducted all statistical analyses using SAS version 9.3 (SAS Institute).
Results
We identified 104 041 people who met the eligibility criteria, with almost equal numbers in the clarithromycin (n = 51 523) and azithromycin (n = 52 518) groups (Figure 1). The most commonly prescribed statin was rosuvastatin (76%), followed by pravastatin (21%) and fluvastatin (3%). Baseline characteristics of the 2 groups were similar, including type and dose of statin used (Table 1). The median dosage was 1000 mg/d for 10 days for clarithromycin prescriptions and 300 mg/d for 5 days for azithromycin prescriptions, which was consistent with drug-prescribing references.41 Co-prescriptions of study statins and clarithromycin continued to occur in each year of the study period, including the most recent years of data accrual (Table 1).
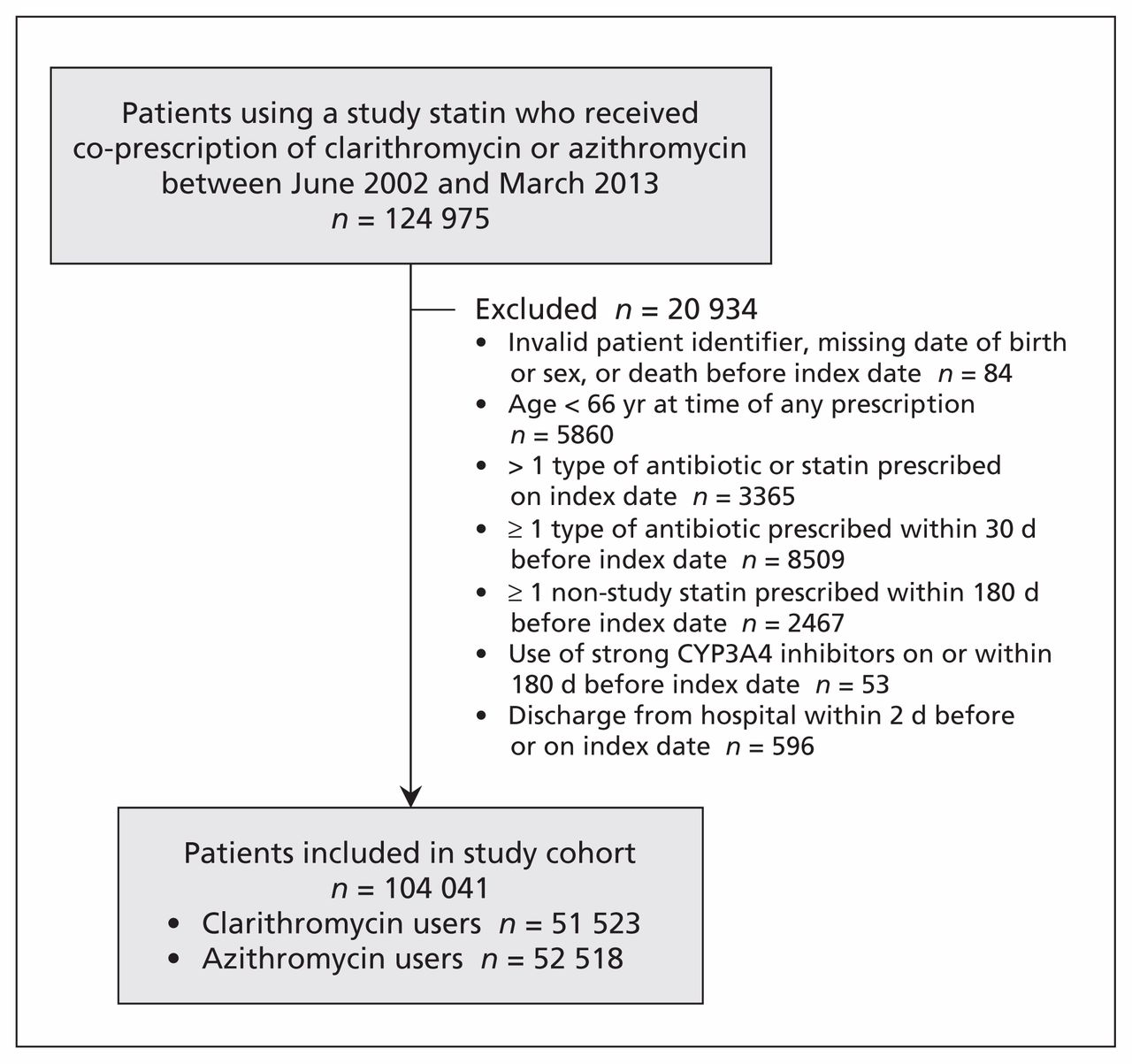
Selection of the study cohort.
Baseline characteristics of patients co-prescribed clarithromycin or azithromycin with a statin not metabolized by CYP3A4
Patient outcomes are presented in Table 2. Co-prescription of clarithromycin with a study statin was associated with a higher risk of most of the outcomes: hospital admission with acute kidney injury (RR 1.46, 95% CI 1.16 to 1.84), hospital admission with hyperkalemia (RR 1.87, 95% CI 1.05 to 3.32) and all-cause mortality (RR 1.32, 95% CI 1.07 to 1.62). The number of admissions with rhabdomyolysis was limited (clarithromycin 13, azithromycin 6); the confidence intervals around the estimate of this adverse event were wide, and the increase in relative risk was not statistically significant (RR 2.21, 95% CI 0.84 to 5.81). All of the results were consistent after adjustment for the confounders (Table 2). The absolute increase in risk for each outcome was small. Even under the assumption that the diagnostic codes underestimated the incidence by five-fold, the absolute increase in risk for each outcome would remain less than 1%.
Outcomes within 30 days after co-prescription of clarithromycin or azithromycin with a statin not metabolized by CYP3A4
Interpretation
In this population-based cohort study, we observed that co-prescription of clarithromycin versus azithromycin in older adults taking a statin not metabolized by CYP3A4 was associated with a modest but statistically significant increase in the absolute risk of hospital admission with acute kidney injury or hyperkalemia and in the absolute risk of all-cause mortality. The population impact of this preventable drug–drug interaction can be considered in the context of the high frequency of clarithromycin and statin co-prescription (rosuvastatin, or Crestor, was the second most commonly dispensed drug in Canada in 201042).
The main mechanism underlying interactions between macrolide antibiotics and statins is often ascribed to the inhibition of the drug-metabolizing enzyme CYP3A4.43–45 For this reason, the US Food and Drug Administration (FDA) currently warns against the co-administration of strong CYP3A4 inhibitors, including clarithromycin, with CYP3A4-metabolized statins.46 However, the inhibition of CYP3A4 cannot explain the increased risk of statin toxicity observed in our study, because we examined interactions with statins not metabolized by CYP3A4.
A growing body of evidence highlights the role of transporter-mediated mechanisms in such interactions, notably the inhibition of human OATPs.19,47–50 Pharmacogenetics research as well as in vitro and clinical drug experiments have shown that reduced activity of OATP1B1 and OATP1B3 is associated with increased systemic exposure of non–CYP3A4-metabolized statins.10,14–16,51,52 In addition, we now know that statins are substrates of a liver-specific bile acid transporter known as sodium taurocholate co-transporting polypeptide (NTCP). Available data suggest that nearly 30% of statin transport into the liver may be mediated by this polypeptide. Thus, observed in vivo inhibitory effects may reflect not only the inhibition of OATP1B1 and OATP1B3, but also the inhibition of NTCP.53,54 However, the OATPs are still considered to be the key rate-limiting transporters that govern the hepatic uptake of statins.55
Limitations
Our study’s findings must be interpreted in the context of its limitations. Prospective collection of data and independent adjudication of outcomes would be the preferred methodology. However, conduct of such a study might not be possible if physicians were required to intervene after learning about concurrent use of drugs with the potential to interact. The increases in absolute risk are underestimated owing to limited sensitivity of the diagnostic codes. However, we preferentially captured the most severe forms of the conditions (i.e., requiring hospital admission), which made these findings of particular interest to clinicians and policy decision-makers. Our findings can be generalized only to older adults, because younger patients are often healthier and may not be as susceptible to drug–drug interactions.56 As with all observational studies, we may have failed to account for important unmeasured confounding variables. Given the complex nature of drug–drug interactions, we also cannot be entirely certain that the observed associations were causal or attributable to the mechanisms we suggest. This limitation may be offset by the comparable usage patterns and risk of adverse events between clarithromycin and azithromycin when used independently, although we did observe a small absolute difference in all-cause mortality with clarithromycin compared with azithromycin in the absence of potentially interacting drugs.32
Conclusion
Co-prescription of clarithromycin and a statin not metabolized by CYP3A4 was associated with a modest increase in the number of deaths and hospital admissions because of adverse events that may reflect statin toxicity among older adults. Although the US FDA recommends the use of non-CYP3A4–metabolized statins as a safer alternative when taken concurrently with CYP3A4 inhibitors,9,50,57 our findings indicate that unintended adverse events may still occur, possibly because of additional mechanisms of drug interactions independent of the CYP3A4 pathway. To prevent toxicity, the use of azithromycin or another antibiotic that does not interact with statins can be considered.
Footnotes
Competing interests: Tara Gomes has received grant funding for the Ontario Drug Policy Research Network from the Ontario Ministry of Health and Long-Term Care. Muhammad Mamdani serves on CMAJ’s Editorial Advisory Board (but had no role in the decision to publish this paper) and has been on advisory boards for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Hoffman–La Roche, Novartis, Novo Nordisk and Pfizer. Amit Garg received an investigator-initiated grant from Astellas and Roche to support a Canadian Institutes of Health Research study involving living kidney donors; his institution received unrestricted research funding from Pfizer. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Daniel Li and Amit Garg drafted the manuscript. Eric McArthur conducted the statistical analysis. All of the authors contributed to the study concept and design and the interpretation of data, revised the manuscript for important intellectual content, approved the final version submitted for publication and agreed to act as guarantors of the work.
Funding: This study was supported by ICES Western. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. Core funding for ICES Western is provided by the Academic Medical Organization of Southwestern Ontario, the Schulich School of Medicine and Dentistry, Western University, and the Lawson Health Research Institute. This project was conducted with members of the provincial ICES Kidney, Dialysis and Transplantation Research Program, which receives programmatic grants from the Canadian Institutes of Health Research. The opinions, results and conclusions are those of the authors and are independent from the funding sources. No endorsement by ICES, the Academic Medical Organization of Southwestern Ontario, the Schulich School of Medicine and Dentistry, Western University, the Lawson Health Research Institute or the Ontario Ministry of Health and Long-Term Care is intended or should be inferred.
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Association of proton pump inhibitors and concomitant drugs with risk of acute kidney injury: a nested case-control study
- Atorvastatin and standard treatment of Helicobacter pylori: Randomized Clinical Trial
- Risk of rhabdomyolysis with donepezil compared with rivastigmine or galantamine: a population-based cohort study
- Association Between Stroke Risk and Metformin Use in Hemodialysis Patients With Diabetes Mellitus: A Nested Case-Control Study
- Risk of cardiovascular events, arrhythmia and all-cause mortality associated with clarithromycin versus alternative antibiotics prescribed for respiratory tract infections: a retrospective cohort study
- Is There Potential for Repurposing Statins as Novel Antimicrobials?
- Macrolide antibiotics and the risk of ventricular arrhythmia in older adults
More in this TOC Section
Similar Articles
Collections

