Article Text

Abstract
Increasing rates of prescription opioid-related death are well documented in Ontario (ON) but little is known about prescription opioid-related harms in other Canadian provinces. Using administrative mortality data from 2004 to 2013, we found that rates of prescription opioid-related death in British Columbia (BC) were higher but more stable than published rates for ON over the same period. Methadone was involved in approximately 25% of the prescription opioid-related deaths in BC. The majority of prescription opioid-related deaths among men and women were unintentional. Men had higher overall rates of prescription opioid-related deaths in BC; women had lower rates of prescription opioid-related deaths but a larger proportion of them were suicides. Efforts to reduce prescription opioid-related deaths must consider sex differences in patterns of prescription opioid use and associated harms.
Statistics from Altmetric.com
Introduction
The recent increase in the rate of prescription opioid overdose death in the USA has been labelled a public health crisis.1 ,2 Dramatic increases in rates of prescription opioid-related deaths are also documented in Australia.3 However, little is known about the nature of prescription opioid deaths in most Canadian provinces as opioid-related harms are not systematically monitored.4 Research from Ontario (ON) indicates that rates of prescription opioid-related death in Canada's largest province parallel upward trends in the USA and Australia.5 However, there is wide regional variation in prescription opioid death rates in the USA,6 suggesting that ON data may not be generalisable to other Canadian provinces.
We describe trends in prescription opioid-related deaths from 2004 to 2013 in British Columbia (BC) and compare them with trends in ON. Additionally, we report sex differences in prescription opioid-related deaths in BC by drug type (methadone and non-methadone prescription opioids) and intent of death (suicide or unintentional). The documented trends are important as BC is a leader in harm reduction efforts in Canada. Further, previous studies indicate that sex should be accounted for when examining prescription opioid-related harms.7 ,8
Methods
We based our analysis of prescription opioid-related deaths on de-identified mortality data from the BC Vital Statistics Agency. Demographic information for rate calculations is from registration files from BC's universal public health insurance plan. Our data were provided by Population Data BC with approval of relevant data stewards and the University of British Columbia's Behavioral Research Ethics Board.9 Data were unavailable for individuals whose prescription drug coverage fell under federal jurisdiction (military veterans, registered First Nations people and Inuit and federal penitentiary inmates, comprising approximately 4% of the BC population).
Deaths were classified by BC Vital Statistics Agency using the International Classification of Diseases, Tenth Revision (ICD-10) codes. The ICD is a standardised coding system used by WHO member states to report mortality data and facilitate regional comparisons. The study cohort included individuals with a cause of death equal to poisoning, including X40–X49 (unintentional), X60–X69 (suicide), X85–X90 (homicide) and Y10–Y19 (undetermined intent). Deaths were further classified using specific codes for drug poisonings recorded in contributing causes of death (ICD-10 codes): drug poisoning (T36.0 to T50.9), non-methadone prescription opioids (T40.2, T40.4), methadone (T40.3), heroin (T40.1); benzodiazepines (T42.4).
Mortality data from ON is reproduced from published literature10 and draws on data from Coroner's records. Owing to differences in coding and information sharing practices between Vital Statistics and Coroner's offices, our data likely underestimate prescription opioid-related deaths in BC.
Results
From 2004 to 2013, there were 3775 drug poisoning-related deaths in BC; prescription opioids were involved in 1674 of these deaths. In BC, we found no significant trends (p=0.60) in the overall and sex-specific rates of prescription opioid-related deaths over the study period (figure 1). The average prescription opioid-related death rate in BC was 3.9 deaths per year per 100 000 population. In contrast to the stable rates in BC, reported rates of prescription opioid-related death in ON significantly increased from 2.7 per 100 000 in 2004 to 4.2 per 100 000 (p=0.001) in 2010 (figure 1).

Rates of prescription opioid-related death in British Columbia (BC) and Ontario (ON) from 2004 to 2013.
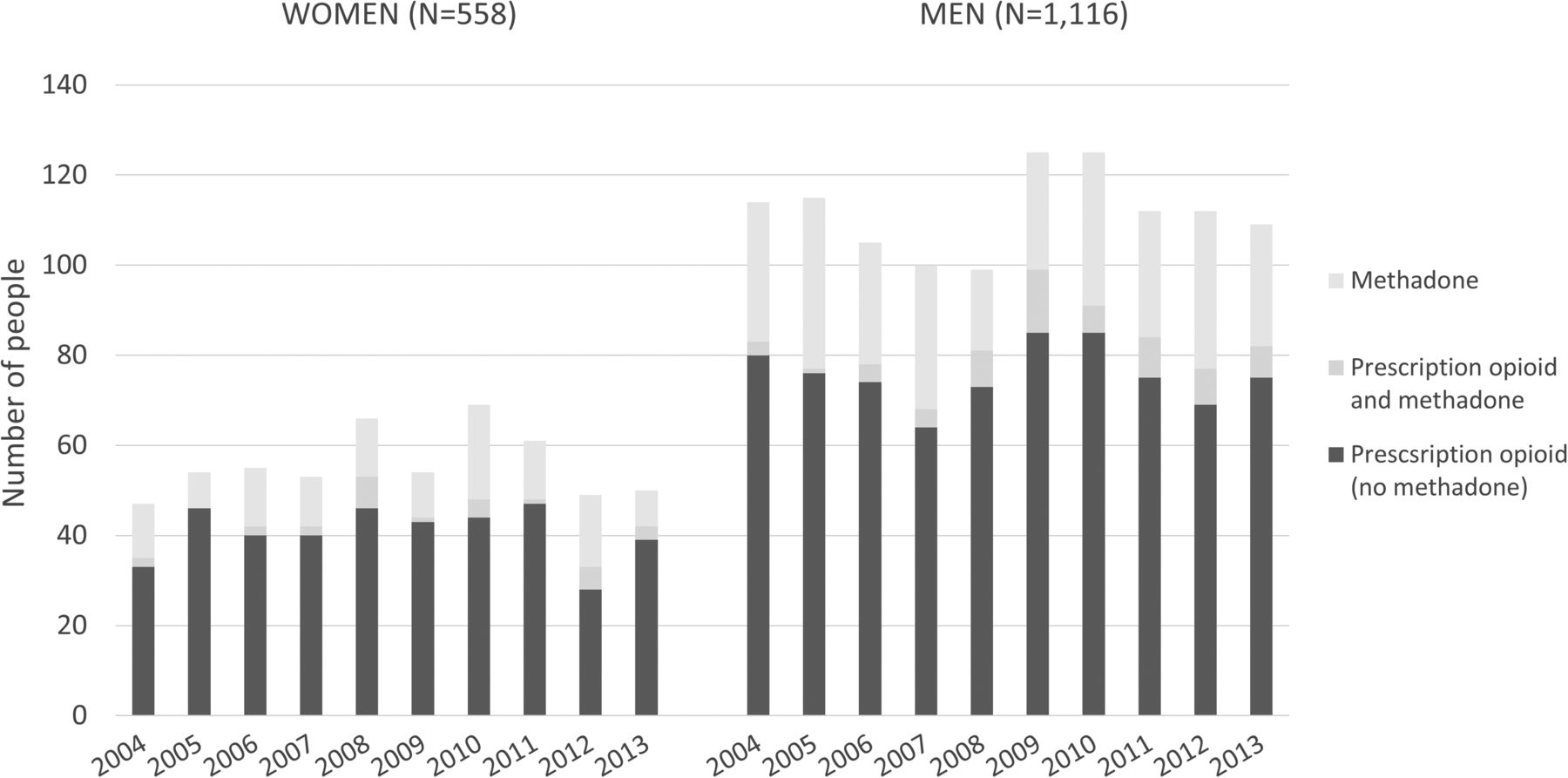
The majority of prescription opioid-related deaths in BC involved non-methadone prescription opioids (figure 2). However, 25% of all prescription opioid-related deaths involved methadone—a drug prescribed in BC primarily to treat opioid addiction—without other prescription opioids. Heroin was a contributing cause of death in only 6% of methadone-related deaths. A small proportion of deaths (5%) involved both methadone and non-methadone prescription opioids. While rates of prescription opioid-related deaths in BC were stable in the study period, deaths involving both prescription opioids and benzodiazepines increased steadily, rising from 2% of prescription opioid-related deaths in 2004 to 14% in 2013.

{kind=link}
{kind=link}
Sex differences in prescription opioid-related deaths in British Columbia (BC) by opioid type (2004–2013).
Prescription opioid mortality rates in BC differed by sex throughout the study period. Men experienced higher mortality rates than women; in 2013, there were 109 prescription opioid-related deaths among men and 50 among women (figure 1). Methadone alone accounted for 27% of these deaths among men and 22% among women. The proportion of prescription opioid-related deaths involving benzodiazepines did not differ substantially for men (10%) or women (12%) over the study period. From 2004 to 2013, the majority of prescription opioid deaths in BC were unintentional—for both women (73%) and men (82%). Equal numbers of men and women died from prescription opioid-related suicide; however, the proportion of prescription opioid-related deaths attributed to suicide was higher among women (23%) than among men (14%). Approximately 4% of deaths for both sexes were of unknown intent.
Discussion
Rates of prescription opioid-related death in BC did not increase from 2004 to 2013. The annual death rate from prescription opioids in BC remained close to 4 per 100 000 population throughout the study period. These stable rates of prescription opioid-related mortality contrast increasing rates in the USA1 and in ON.10 This is not to suggest that prescription opioid-related deaths are not at crisis levels in BC. In fact, the recent prescription opioid crisis in ON may be less severe than BC's equilibrium level, as the Vital Statistics data used in our study likely underestimate prescription opioid deaths in BC. Differences in trends in prescription opioid-related deaths between BC and ON may reflect divergent trends in prescription opioid dispensing. For example, the volume of oxycodone and fentanyl dispensed in ON has increased more rapidly than in BC.11
A stable minority of prescription opioid-related deaths in BC involved methadone. From 2004 to 2013, methadone alone contributed to one in four prescription opioid-related deaths. This figure is high, although slightly lower than findings from a similar study in West Virginia, where methadone alone contributed to one in three prescription opioid-related deaths.12
Sex differences in prescription opioid morality rates indicate that prescription opioid-related harms impact men and women differently. Deaths among men account for approximately two-thirds of all prescription opioid-related deaths in BC—a result comparable with studies of prescription opioid-related deaths in the USA.13 ,14 Our finding that suicide accounted for a higher proportion of prescription opioid-related deaths among women than among men is also consistent with published literature.15 This sex difference is driven by lower rates of unintentional death among women, and not by sex differences in suicide rates involving prescription opioids. The latter point is notable because the overall suicide rate in Canada is three times higher for men than for women.16
Our results also suggest that efforts to reduce the burden of prescription opioid-related deaths should consider sex differences in patterns of prescription opioid use and associated harms. For example, efforts to reduce unintentional overdose deaths may be particularly important among men. Similarly, knowledge of the high proportion of prescription opioid suicides among women may lead to practices and policies to help prevent suicides.
Of some concern is the stable but significant rate of deaths involving methadone. Populations using methadone often deal with serious addiction, and are consequently at elevated risk of harm; further research may help reduce methadone-related harms while maintaining access to treatment for those living with opioid addiction.
There are limitations to the use of Vital Statistics data. For example, limitations of the ICD-10 coding system used in Vital Statistics data do not allow for a detailed analysis of non-methadone prescription opioids by drug type. Further, although professionally abstracted from death certificates, Vital Statistics data likely underestimate the absolute level of prescription opioid-related deaths in BC. It is not known whether potential under-reporting is changing over time; however, it is unlikely that prescription opioid deaths are differentially reported by sex.17 Rates of prescription opioid-related death may differ among populations not captured in this analysis; this topic should be investigated among First Nations and incarcerated populations. Further, results from BC may not be generalisable to other regions of the country. Prescription opioid-related deaths should therefore be examined in other Canadian provinces.
While prescription opioid-related death rates in ON have increased rapidly over the past decade, rates in BC are stable but high. This suggests that the stage and extent of prescription opioid crises differ across provinces, affected by differences in prescription drug monitoring, prescribing practices and harm-reduction efforts. Further, the observed sex differences in prescription opioid-related deaths indicate that approaches to reduce prescription opioid-related harms might best be tailored for men and women.
What is already known on the subject
Deaths from prescription opioids are a leading cause of injury mortality in North America and Australia.
There are sex differences in health behaviors and in the risk of injury mortality.
What this study adds
There is wide geographic variation in the stage and extent of the prescription opioid crisis in Canada.
Men have higher rates of prescription opioid-related death than women in British Columbia, Canada.
Methadone alone contributes to one quarter of prescription opioid-related deaths in British Columbia, Canada.
National Rifle Association helps keep deadly guns on the market
George Zimmerman, a retired police officer, listed his PF-9 pistol in an online auction with a starting bid of $5000. This was the gun he used in 2012 to kill Trayvon Martin, an unarmed teenager. In support of this sort of activity, CNN reports that in the past 8 years, 11 states have passed NRA-backed laws encouraging or requiring police to resell confiscated guns.
References
Footnotes
Twitter Follow Emilie Gladstone at @emiliegladstone
Contributors EJG conceptualised the study, conducted the data analysis, interpreted the data and drafted the manuscript. KS and SGM contributed to the study design, acquisition and interpretation of data, and revised the manuscript for important intellectual content. All authors give approval of the final version to be published and are responsible for the overall context as guarantors.
Funding This research was funded by the Canadian Institute for Health Research (CIHR DCO150GP).
Competing interests None declared.
Ethics approval The University of British Columbia's Behavioral Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.